


Érico Pampado Di Santis1; Beatriz Lopes Ferraz Elias2; Raul Vieira de Souza Barros3; Samuel Henrique Mandelbaum4
Keywords: CHEMEXFOLIATION; PHENOL; ANESTHESIA; ANALGESIA.
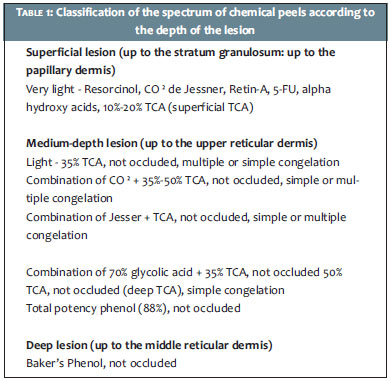
Chemical peels consist of applying one or more exfoliating agents to the skin. Such agents are strong enough to result in the controlled destruction of the cutaneous tissue. Peels are classified according to their depth of action. While there are several classifications available in the literature, the authors consider the Lawrence, Brody and Alt's classification, which is based on the level of injury caused, the more instructive.1 (Table 1) The depth to which the substance penetrates depends on its composition, concentration, and pH, as well as the amount of exposure time.1, 2
Phenol or carbolic acid (C6H5OH) (Figure 1) is derived from coaltar and when in contact with the skin, produces coagulation and denaturation of the protein's of the epidermal keratin. 4, 5
The use of phenol in dermatology began in the nineteenth century. In 1882, Paul G. Unna described the actions of salicylic acid, resorcinol, trichloroacetic acid, and phenol in the skin, establishing a reference for many other authors. 6 Mackee used phenol in peels for therapeutic effects in 1903. This British dermatologist published his studies when already a professor in the dermatology department at New York University, in 1952. 7 The use of phenol was developed in France after World War I. 8 In the 1940s, in the United States, Eller and Wollf carried out the first systematic study on the use of phenol, resorcinol, salicylic acid, and carbon dioxide criotherapy for treating scars. 9 In the 1960s, many formulas containing phenol were experimented with by dermatologists and plastic surgeons.
In 1961, Baker and Gordon described and detailed a phenol solution diluted in water and associated with croton oil and liquid soap, which to the present day is the most widely used in practice and the most frequently referred to in scientific publications on the subject. 10 Phenol peeling with the Baker-Gordon formula is indicated for the treatment of severe facial aging with deep rhytids and advanced alterations in the skin's texture. It remains among the most effective methods of chemical rejuvenation due to its effect on the remodeling of collagen fibers. It acts on the skin's color, producing a global whitening of the face. Histologically, the restructuring of the basal layer takes place, disabling melanocytes and inhibiting the transfer of melanosomes to nearby keratinocytes. 1An immunohistochemical study in rats that underwent medium and deep chemical peels showed an increase in the amount of collagen and elastic fibers. 11
Phenol peeling seems to also be effective for treating pre-malignant and malignant lesions. Furukawa and Yamamoto applied deep phenol peel in a group of patients with an aim at treating skin cancer, and obtained a good response. The same study highlights evidences in the success of the treatment of superficial basal cell carcinoma, Bowen's disease and actinic keratoses. 12
The theoretical effect of phenol peeling is directly proportional to its penetration into the skin layers. The absolute phenol (88%) immediately coagulates the proteins of the epidermis, which self-blocks its penetration, resulting in a medium peel.
The dilution of 2ml of phenol in 3ml of water-as in the Baker-Gordon formula-does not immediately cause coagulation of proteins in the epidermis. The phenol/water solution receives 8 drops of liquid soap and 3 drops of croton oil. The liquid soap acts as a surfactant (Surface active agent) i.e. it is a superficial activity agent that has the ability to alter the superficial and interfacial properties of a liquid or of its immiscible phases. It also has affinity for oils and water. It reduces the surface tension and allows the penetration of phenol into the skin.13 Croton oil is derived from the seeds of the plant Croton tiglium and acts on epidermal vesiculation, allowing the penetration of phenol. The penetration depends, therefore, on the dilution of the phenol, on the association with the surfactant, on the vesicant agent, and on the occlusion, among other factors.
There is a time lapse of between 8 to 12 hours from the initial application of the Baker-Gordon solution and the onset of phenol in the nerve endings, when it plays its anesthetic role to halt the pain process.
The patient must therefore be kept comfortable throughout the application of the phenol solution and up to 12 hours after its completion.
Thus, the excellent therapeutic effects of this formula collide with painful discomfort during application and in the succeeding hours. The effective control of pain makes the procedure more secure, fast, simple, and easily reproducible. Therefore, standardized analgesia and sedation techniques are required to minimize the discomfort of the procedure and reduce patient anxiety.
The present study was aimed at investigating what has already been published about analgesia/anesthesia for the purposes of phenol peeling using the Baker-Gordon solution, and seeking proposals for controlling the pain during and after the procedure.
A search process was initially carried out on the PubMed and Cochrane Library databases, produced by the National Library of Medicine and the Virtual Health Library, respectively. The keywords used were: chemexfoliation, peel, peeling, phenol, with cross-references to the terms anesthesia and analgesia. Specifically, no articles that matched the search parameters were found for the intersection between the descriptors chemexfoliation AND phenol AND anesthesia OR analgesia.
The search strategy phenol AND peelingwas used on the PubMed database, which yielded 151 articles, including descriptions of the risks of phenol peeling, accurate indications, action detailed histologically, complications and their prevention, in addition to the approach of arrhythmias associated with the phenol peel. 1, 4, 11, 14, 15 Two articles addressed the authors' focus of interest, without, however, being specific: Yoon and Ahn recorded that all patients in the study underwent phenol peeling under deep intravenous sedation, and Edison suggests technical changes aimed at decreasing the pain. 16, 17
A new search strategy was then used in the same database with the words: anesthesia AND peeling, which yielded 28 articles, some consideringthe use of topical anesthetic to perform superficial peeling and the use of anesthesia in fractional laser.18, 19
The following search was run in the second secondary sources database (Cochrane Library BVS), with the terms anesthesia AND phenol AND peeling, which did not yield references. Changing the terms for anesthesia AND peeling, one Cochrane record was found for controlled trials, which compared topical anesthetics in medium peels.20
Then a new search with the terms phenol AND peeling resulted in four references: two Cochrane systematic reviews and two Cochrane records on controlled trials.20-23 Finally, a search was run with the terms analgesia AND peel and with the terms anesthesia AND chemexfoliation, which did not answer the authors' question. 23, 24 Therefore, the search run on the databases (PubMed and Cochrane) for articles addressing in detail the subject of pain during, and 12 hours after the application of chemical peels withthe Baker-Gordon solution, proved negative.
In fact, in the authors' daily dermatologic practice, a lower level of scientific evidence underpins the execution of the procedure, meaning that it is the experience of the specialist that comes into play, and in the present case this is the role of the anesthesiologist.
Conscious sedation
It was possible to comfortably carry out the procedure in question-for the medical staff and especially for the patient-using this type of sedation.
Conscious sedation has become a common practice in surgical and dermatological procedures.9 It is defined as any degree of sedation that allows good perioperative anxiolytic and analgesia effect and amnesia, without the need for mechanical ventilation and preservation of ciliary reflex and light verbal physical stimulation. Due to the potential risk of cardiorespiratory depression caused by the combined intravenous administration of benzodiazepines and narcotics, conscious sedation should be administered in a hospital setting, with resuscitation and ventilation equipment available, in addition to cardiac monitoring throughout the procedure. 25, 26
It is aimed at maintaining adequate sedation with minimal risks, reducing anxiety, and promoting analgesia and amnesia. It is a safe and efficient method with immediate action, rapid regaining of consciousness, and a low incidence of post-operative side effects. 25 As there is no isolated pharmacological agent or technique that satisfies these requirements, the anesthesiologist physician must combine drugs to get closer to the ideal situation.
The pharmacological agents used for conscious sedation are: propofol, midazolam, and fentanyl and ketamine in combination. 27
Propofol is the drug of choice for inducing and maintaining anesthesia, and the most-used intravenous agent for ambulatorial anesthesia and sedation due to its pharmacodynamic properties and its favorable pharmacokinetics. It is characterized by rapid onset and short duration of action, its short half-life, high plasma clearance (equal to or higher than the blood flow of the liver) associated with the great distribution volume, and rapid regaining of consciousness even after prolonged and continuous infusion when used as the sole anesthetic agent.
Used in sub-hypnotic doses, propofol provides an easily titratable level of sedation and anxiolysis, similar to that of midazolam. When propofol is used in low concentrations, its respiratory effects are moderate and allow spontaneous ventilation during the maintenance of anesthesia and sedation.27 It also presents a well-known antiemetic effect. Propofol does not exert an analgesic effect, making necessary the combination of analgesics, such as fentanyl. 9
Fentanyl is a widely-used opioid for ambulatorial anesthesia. It is a potent opioid agonist derived from phenylpiperidine, and acts on analgesia and sedation. Despite its cumulative potential, when used in low doses (25-100µg) it does not delay the recovery and provides adequate immediate post-operative analgesia. It can also be used as a pain killer in the early stages of recovery, for it provides analgesia in a timing sufficient to allow the onset of the action of opioid analgesics. As with all opiates, it should be used in the titration, in view of its slow onset (four minutes to achieve the effect), with respiratory ventilation equipment available.27
A potent benzodiazepine, midazolam is characterized by a slower onset of action than that of diazepam, and a short half-life of elimination (two hours). Sedative effects vary among patients, and the sedation recovery time can be prolonged, accompanied by slow recovery of higher functions, and persistent amnesia after waking. The complete recovery requires approximately 90 minutes after a single 0.1mg/kg dose. In addition to its use in conscious sedation, it is also used as a pre-anesthetic medication. Cardiovascular side effects are rare and mild in the doses used for sedation, however can be significant with higher doses, especially in hypovolemic patients.26
Ketamine is an intravenous dissociative anesthetic that plays an important role in analgesia and sedation in ambulatorial surgeries and procedures, especially as an adjuvant to other hypnotic drugs. The hypnotic sedative property results in light dissociative sleep with a potent analgesic property.
Its clinical effects are mediated by non-competitive antagonism in the opioid receptors. The analgesic properties in plasma concentrations are significantly lower than those of the drugs that produce unconsciousness. The adjuvant use of ketamine during propofol sedation offers significant analgesia and minimizes the need for additional opioids when administered in sub-hypnotic doses. 28
The choice and use of these drugs for conscious sedation by the anesthesiologist physician must be individualized. The clinical follow-up carried out by the anesthesiologist during and after the procedure is of crucial importance for the patient's comfort and therapeutic success.
Phenol peeling is an important treatment in facial skin rejuvenation, in addition to being a possible therapy in malignant and pre-malignant conditions; the interaction between the dermatologist and the anesthesiologist physician for the implementation of the procedure makes it less traumatic for the patient. Further studies should be carried out with an aimat achieving a higher level of scientific evidence.
1. Lawrence N, Brody HJ, Alt TH. Peelings químicos. In: Coleman WP, Hanke CW, Alt TH, Asken S. Cirurgia cosmetica: Princípios e técnicas. Rio de Janeiro: Revinter; 2000. p.85-111.
2. Fischer TC, Perosino E, Poli F, Viera MS, Dreno B. Chemical peels in aesthetic dermatology: an update 2009. J Eur Acad Dermatol Venereol. 2010;24(3):281-92.
3. Monheit GD, Chastain MA. Chemical peels. Facial Plast Surg Clin North Am 2001;9:239-55.
4. Lawrence N, Brody HJ, Alt TH. Peelings químicos. In: Coleman WP, Hanke CW, Alt TH, Asken S. Cirurgia cosmetica: Princípios e técnicas. Rio de Janeiro: Revinter; 2000. p.85-111.
5. Kadunc BV, Vanti AA. Avaliação da toxicidade sistêmica do fenol em peelings faciais. Surg Cosmet Dermatol. 2009;1(1):10-4.
6. Velasco MVR, Okubo FR, Ribeiro ME, Steiner D, Bedin V. Rejuvenescimento da pelepor peeling químico: enfoque no peeling de fenol. An Bras Dermatol. 2004;79(1):91-9.
7. Brody HJ, Monheit GD, Resnik SS, Alt TH. A history of chemical peeling. Dermatol Surg. 2000;26(5):405-9.
8. Mackee GM, Karp FL. The treatment of post-acne scars with phenol. Br J Dermatol.1952;64(12):456.
9. Stuzin JM. Phenol peeling and the history of phenol peeling. Clin Plast Surg.1998;25(1):1-19.
10. Eller JJ, Wolff S. Skin peeling and scarification: in the treatment of pitted scars, pigmentations and certain facial blemishes. JAMA. 1941;116(10):934- 8.
11. Baker TJ, Gordon HL. The ablation of rhytides by chemical means; a preliminary report. J Fla Med Assoc. 1961;48:541.
12. Han SH, Kim HJ, Kim SY, Kim YC, Choi GS, Shin JH. Skin rejuvenating effects of chemical peeling: a study in photoaged hairless mice. Int J Dermatol. 2011;50(9):1075-82.
13. Furukawa F, Yamamoto Y. Recent advances in chemical peeling in Japan. J Dermatol. 2006;33(1):655-61.
14. Daltin D. Sabões. In: Daltin D. Tensoativos: química, propriedades e aplicações. São Paulo: Blucher; 2011. p.11-8.
15. Fulton Jr JE, Porumb S. Chemical Peels Their Place Within the Range of Resurfacing Techniques. Am J Clin Dermatol. 2004;5(3):179-87.
16. Landau M. Cardiac Complications in Deep Chemical Peels. Dermatol Surg. 2007;33(2):190-3.
17. Yoon E, Ahn DS. Report of phenol peel for Asians. Plast Reconstr Surg. 1999;103(1):207-14.
18. Edison RB. Phenol peeling: new standards of excellence. Aesthetic Plast Surg. 1996;20(1):81-2.
19. Iannitti T, Capone S, Palmieri B. Short review on face rejuvenation procedures: focus on preoperative antiseptic and anesthetic delivery by JetPeelTM-3 (a high pressure oxygen delivery device). Minerva Chir. 2011;66(3)Suppl 1:1-8.
20. Goel A, Krupashankar DS, Aurangabadkar S, Nischal KC, Omprakash HM, Mysore V. Fractional lasers in dermatology--current status and recommendations. Indian J Dermatol Venereol Leprol. 2011;77(3):369-79.
21. Koppel RA, Coleman KM, Coleman WP. The efficacy of EMLA versus ELA-Max for pain relief in medium-depth chemical peeling: a clinical and histopathologic evaluation. Dermatol Surg. 2000:26(1):61-4.
22. Samuel M, Brooke R, Hollis S, Griffiths CEM. Interventions for photodamaged skin. Cochrane Database Syst Rev. 2005;25(1):CD001782.
23. Piacquadio D, Dobry M, Hunt S, Andree C, Grove G, Hollenbach KA. Short contact 70% glycolic acid peels as a treatment for photodamaged skin. A pilot study. Dermatol Surg.1996;22(5):449-52.
24. Dailey RA, Gray JF, Rubin MG, Hildebrand PL, Swanson NA, Wobig JL et al. Histopathologic changes of the eyelid skin following trichloroacetic acid chemical peel. Ophthal Plast Reconstr Surg. 1998;14(1):9-12.
25. Niechajev I, Ljungqvist A. Perioral dermabrasion: clinical and experimental studies. Aesthetic Plast Surg.1992;16(1):11-20.
26. Otley CC, Nguyen TH. Safe and Effective Conscious Sedation Administered by Dermatologic Surgeons. Arch Dermatol. 2000;136(11):1333-5.
27. Gross JB, Bailey PL, Connis RT, Cote CJ, Davis FG, Epstein BS, et al. Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology. 2002;96(4):1004-17.
28. Tesniere A, Servin F. Intravenous techniques in ambulatory anesthesia. Anesthesiol Clin N Am. 2003;21(2):273-88.
This study was performed at the Hospital Universitário de Taubaté (HUT), Taubaté - SP, Brazil and at ViValle Hospital de São José dos Campos - São José dos Campos (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}