


Érico Pampado Di Santis1; Leopoldo Duailibe Nogueira Santos2; Sheila Martins Di Santis3; Iuri Vieira Dair4; Marcia Lanzoni de Alvarenga Lira5
Keywords: GYNECOMASTIA; AMBULATORY SURGICAL PROCEDURES; DERMATOLOGY; ANESTHESIA, LOCAL.
True gynecomastia (TG) is a benign proliferation of glandular tissue in the male breast. There are three peaks of incidence: in newborns, adolescents, and middle-aged adults. Gynecomastia in childhood is transient and subsides after two or three weeks, when the level of maternal estrogen in the newborn decreases. In adolescence, there is a peak between 13 and 14 years, decreasing on average in 18 months. In those cases, persistence of the condition is rare, however it may linger after puberty, continuing into adulthood. The third peak occurs in men between 50 and 80 years old.
Mammary tissue is sensitive to serum levels of free estrogen. The augmentation of the tissue is related to a higher absolute level of free estrogen, or relative to the level of testosterone, resulting in greater stimulating action, which causes its growth.1-3
The most common cause of gynecomastia in adolescence is physiological. In adults, the main causes are: persistence of juvenile gynecomastia and the idiopathic form, followed by those resulting from the use of certain drugs-such as spironolactone, nifedipine, estrogen, anti-androgen, and efavirenz. There are other causes of lesser expression, like certain diseases-such as cirrhosis, hypogonadism, and testicular tumor, among others.1,2
TG should be differentiated from pseudogynecomastia, which occurs due toan increase in theadipose tissue of the breast. Causes include obesity and lipodystrophy, including that triggered by a patient's treatment with antiretroviral therapy. In these cases, it is not possible during palpation of the breast to verify a subareolar mass-as is the case in TG. Regarding neoplastic lesions, breast cancer is an important differential diagnosis. In general, it arises as a mass eccentric to the nipple, adhered to deep planes and with a hardened consistency.
The diagnosis of TG is primarily carried out through detailed anamnesis and physical examination. In inconclusive cases, there is a need for additional tests, both laboratorial and image based, in order to exclude tumors, among other causes.
The treatment will depend on the cause,the duration of the clinical condition since onset, and the level of disruption the condition presents to the patient. Should it be secondary to the use of any medication, the first measure is to suspend the suspected drug. The time since onset is important due to the fact that, initially, the tissue is in the inflammatory phase. In such cases, it is possible to choose either a conservative approach (given that there is spontaneous regression in most cases) or to introduce medications (such as androgens, selective modulators of estrogen receptors and aromatase inhibitors) to accelerate the involution of the inflamed mammary tissue. Nevertheless, after the initial inflammatory period, the tissue becomes fibrotic, requiring surgical treatment. The excision of mammary tissue is performed as a surgical procedure. If there is excess adipose tissue associated with it, it is possible to administer supplementary liposuction treatment.5
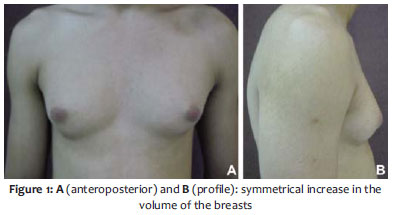
A 26-year-old male patient complained of a "lump" in the breasts since adolescence. Local symptoms were denied. Dermatological examination evidenced a symmetrical increase in breast volume (Figure 1). On palpation, it was possible to notice dense fibroelastic tissue in the subareolar region. The patient reported worsening of the increase in size after starting the use of injectable medication (was unable to refer the drug type) during training at the gym, as well as dietary supplements aimed at gaining muscle mass (creatine and protein). In addition, the patient used 1 mg finasteride per day for treatment of androgenetic alopecia-the drug was initiated in the presence of an already established gynecomastia picture.
Thus, an evaluation carried out by an endocrinologist was indicated, when supporting tests were requested, including prolactin, serum testosterone, liver biochemistry, renal function, thyroid evaluation, FSH, LH, lipid profile, fasting blood glucose, insulin, and scrotal ultrasonography. All tests came back within normal parameters, with tumoral or secondary causes (such as kidney or liver disease) being excluded. Breast ultrasonography was also requested, revealing a significant increase in fibroglandular tissue. In light of the above, a case of true adolescent gynecomastia with persistence in adulthood, probably exacerbated by the use of injectable drugs, was diagnosed. Due to the aesthetic discomfort experienced by the patient, surgery to decrease the breast size was indicated.
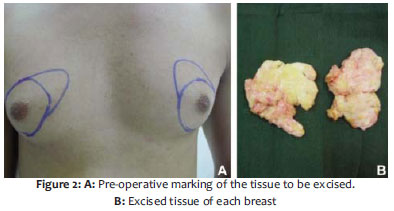
Surgery was performed under local anesthesia with tumescent solution in the proportion of 0.9% saline solution (200ml), 2% lidocaine (20ml), sodium bicarbonate (8 ml) and epinephrine (1ml). A decision was made for a semicircular periareolar incision, followed by the block exeresis of excess mammary gland (Figure 2). Suture was performed with 5.0 monofilament nylon thread. Compressive dressing with elastic mesh was used for 48 hours. There were no post-operative complications. A satisfactory cosmetic result can be noticed three months after the surgery (Figure 3).
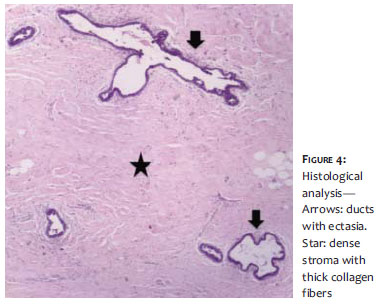
The excised tissue was sent for histological examination, revealing breast parenchyma with dense stromal tissue (and thick collagen fibers), some adipocytes, ducts with ectasia overlaid with simple cuboidal epithelium without atypia, and absence of inflammatory infiltrate (Figure 4)-all confirming the diagnosis of true gynecomastia in the fibrotic phase.
The description demonstrates a typical case of true gynecomastia persistent in adulthood. The hypothesis of TG in adolescence is strengthened by the age of onset in the studied patient-i.e. the second peak of incidence of true gynecomastia. Nevertheless, it was not possible to rule out exogenous causes (drugs).
As there was no regression after 18 months, the mammary tissue evolved from the inflammatory to the fibroticphase. In such cases, the only treatment option is surgical. According to the Moschella and Cordova's morphological classification of gynecosmastia, the patient was in Grade II, indicating hypertrophy of all structural components of the breast, with the nipple-areolar complex located above the breast fold. In such cases, surgical treatment may be associated to liposuction and glandular resection. Regarding the options for incision, these are: periareolar semicircular, intra-areolar, the pull-through approach, or endoscopic.6
After hormonal investigation and interruption of injectable medication, a decision was made for the excision of glandular tissue, discarding the need for liposuction, once there was only a small amount of adipose tissue. In this way, there was no removal of excess tissue, which could have resulted in the flattening of the chest, local irregularity or even concavity. Finally, a good cosmetic result was obtained.
1. Olsson H, Bladstrom A, Alm P. Male gynecomastia and risk for malignant tumours--a cohort study. BMC Cancer. 2002;2:26.
2. Braunstein GD. Gynecomastia. NEJM. Mass Medical Soc. 2007;357(12):1229-37.
3. Nordt CA, DiVasta AD. Gynecomastia in adolescents. Curr Opin Pediatr. 2008;20(4):375-82.
4. Ma NS, Geffner ME. Gynecomastia in prepubertal and pubertal men. Curr Opin Pediatr. 2008;20(4):465-70.
5. Gikas P, Mokbel K. Management of gynaecomastia: an update. Int J Clin Pract. 2007;61(7):1209-15.
6. Cordova A, Moschella F. Algorithm for clinical evaluation and surgical treatment of gynaecomastia. J Plast Reconst Aesthet Surg. 2008;61(1):41-9.
Study performed at the Hospital Universitário de Taubaté / Universidade de Taubaté (HUT / UNITAU)-Taubaté (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}