


Sergio Schalka1; Christiane Monteiro Agelune2; Alessandra Torres Nogueira3; Felipe Fernandes de Abreu4
Keywords: CHEMEXFOLIATION; SKIN; COSMETICS.
Current dermatological practice presupposes the development of different therapeutic procedures for the treatment of facial aging.1
From within the existing dermatologic armamentarium, it is possible to cite procedures that exert some degree of exfoliation or abrasion on the skin, such as chemical peels, lasers, and other technologies that employ light and microdermabrasion.1
With all of these exfoliating procedures, there is an intentional generation of damage to the cutaneous barrier in order to promote the repair of the epidermis and increased cell renewal, all aimed at producing aesthetic benefits.1
By promoting damage (chemically, physically, or mechanically) to the stratum corneum or epidermis, some degree of irritation-which translates into erythema and/or edema, in addition to desquamation of greater or lesser intensity-is expected to occur clinically, depending on the depth of the damage. Facial chemical exfoliation is a well-established procedure in which the dermatologist uses some agent (usually acids) that produces aggression to the skin, with consequent damage to the cutaneous barrier.2
There are different types of chemical exfoliation (or peels) used in dermatologic practice, with the most common being superficial peels performed with the use of retinoids and hydroxy acids.1,2
Retinoic acid peeling has been proposed in the literature as an option with high tolerability and low rates of adverse reactions.3
The presence of desquamation and dryness is observed in most patients, with the possible occurrence of mild erythema.3-8 The desquamation process is usually more intense between the third and seventh day after the application of tretinoin (retinoic acid).
In the period immediately subsequent to the performing of the procedure, it is recommended that the dermatologist instruct the patient in the use of sunscreen and moisturizing agents that are able to provide a restorative action on the cutaneous barrier. This helps to relieve symptoms (such as burning, scaling, and erythema) and promotes the quick and efficient repair of the superficial structures of the epidermis-in particular the stratum corneum.9
Among the agents with a moisturizing and repairing effect on the cutaneous barrier, the use of sodium PCA, panthenol, dimethicone, cyclopentasiloxane, and karité butter stand out.10
The present study was aimed at evaluating, on a comparative basis, the efficacy and safety of a dermo-cosmetic formulation (test product) associated with the use of sunscreen versus the isolated use of sunscreen, in the care of the skin that had undergone cosmiatric procedures (facial chemical exfoliation). Evaluations were based on clinical and instrumental measurements of corneometry and evaporimetry (TEWL).
A clinical, comparative, randomized, and monocentric study was carried out with the assistance of clinical and instrumental evaluation.
After the approval by the Research Ethics Committee (REC), 64 volunteers (52 women with ages between 35 and 65 years) were recruited during the period March-June 2013 who were undergoing cosmiatric treatment, which included plans for facial peeling with retinoic acid. All volunteers expressed their willingness to participate in the study by signing the Free and Informed Term of Consent (FITC) prior to undergoing any procedure planned in the protocol.
In order to ensure the eligibility of volunteers, in addition to meeting the characteristics of the population, they could not present with any of the following criteria: pregnancy or potential risk of pregnancy, lactation, use of topical or systemic anti-inflammatory medications and/or immunosuppressants, antihistamines for up 15 days before the start of the study, previous reaction to cosmetic products for the facial area, atopic or allergic history, local and/or disseminated active skin conditions that could interfere with the study results, pathologies that could cause immune suppression, intense exposure to the sun 15 days before inclusion in the study, and any other condition deemed by the volunteer investigator reasonable for disqualification.
After initial clinical evaluation for the verification of the eligibility criteria and photographic records, all volunteers underwent measurements of skin hydration (through the corneometry technique) and integrity of the cutaneous barrier (by measuring transepidermal water loss through evaporimetry) as described below.
Evaporimetry: the Tewameter® TM 300 (Courage & Khazaka) device was used to quantify the transepidermal water loss and, consequently, the functional integrity of the stratum corneum. The greater the integrity of the cutaneous barrier, the lesser the transepidermal water loss.
Corneometry: the Corneometer® MPA 580 (Courage & Khazaka) device was used to assess the hydration level by measuring the electrical conductivity in the skin, which takes place due to the presence of water. The higher the electrical conductivity measured, the higher the water content that is present in the skin's surface.
Measurements were carried out in the treated area (face) and in the control area (without treatment and previously defined as the volar aspect of the right and left forearm) for all instrumental evaluations.
Later on, the volunteers underwent peeling with 5% retinoic acid in hydroalcoholic vehicle, performed by a dermatologist physician. The volunteers were instructed to remove the product four hours after the application.
At the end of the session, the volunteers were randomly divided into two sub-groups, namely:
Group I-Application of standard sunscreen every two hours + study product, applied twice daily.
Group II-Application of standard sunscreen every two hours.
The products were distributed to the volunteers to be applied at home, along with a guidance booklet on how to use them.
The volunteers returned on the following days: D1 (24 hours), D2 (48 hours), D3 (72 hours), D4 (96 hours), D5 (120 hours) and D6 (7 days).
At the intervening and final visits, corneometry and evaporimetry measurements, in addition to clinical assessments, were carried out in the treatment areas and under the conditions defined at the initial visit.
The clinical evaluation consisted of observing the clinical characteristics of the facial skin based on the parameters erythema, dryness, and desquamation, grading it with the assistance of a four-point scale (0-3).
The test product (Cetaphil Advanced,® Galderma, Brazil), is a dermocosmetic that has a hydrating and reparative effect on the cutaneous barrier, which contains ERC-5® complex (whose composition includes the agents sodium PCA, panthenol, dimethicone, cyclopentasiloxane, and karité butter emulsion). One unit of the product was supplied to each volunteer in Group I (treated), along with sunscreen, for exclusive use during the study period.
The standardized sunscreen for both Groups was dispensed with SPF 30.
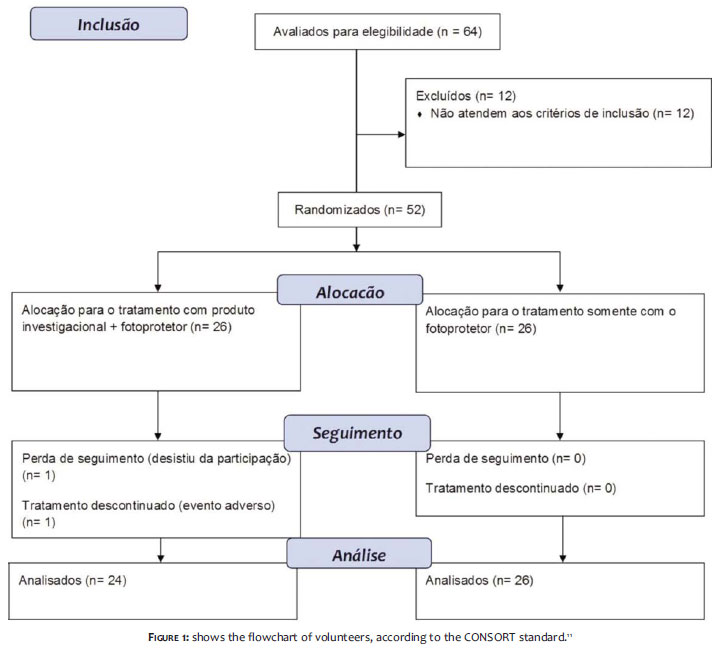
Of the 64 volunteers initially evaluated, 52 were randomized and started the study, with 26 volunteers allocated to each group.
Fifty volunteers completed the study: 24 in Group I and 26 in Group II.
One volunteer withdrew from participation for personal reasons, and the other presented with a mild contact dermatitis condition, and was discontinued from the study.
There were no other reports of adverse events.
Figure 1 shows the flowchart of volunteers, according to the CONSORT standard.11
Only volunteers who completed the study were considered for the evaluation of efficacy.
1-Clinical Assessment
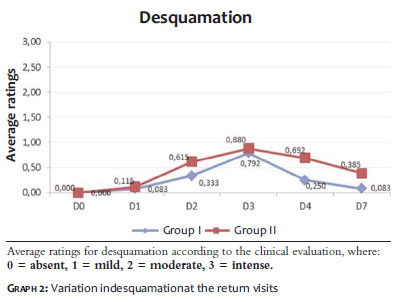
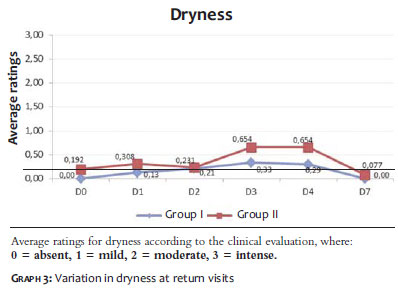
Graphs 1, 2, and 3 show the average score for clinical evaluation of erythema, desquamation, and dryness, respectively, in the different experimental times:
The graphical analysis shows that Group I has higher results (lower average) as compared to Group II in the parameters desquamation and dryness in most experimental time periods. For the parameter erythema, slightly higher values were observed in Group I as compared with Group II, except for in the final evaluation (D7).
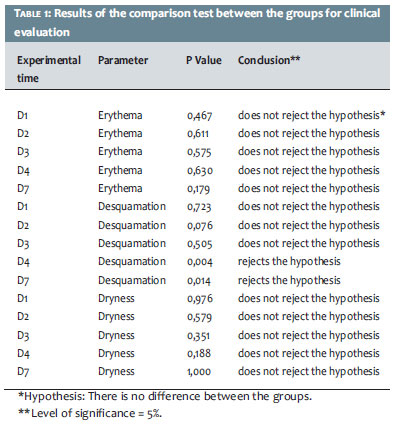
The results of the two groups were compared using the Mann-Whitney test, as shown in Table 1:
It is important to note that there is a statistically significant difference between Groups for desquamation on D4 and D7, when Group I had lower averages than those in Group II. There was no statistically significant difference between the groups for the parameters erythema and dryness.
2-Instrumental Effectiveness through Corneometry
The results of the evaluation of skin hydration through the corneometry technique are expressed in a corneometric index, a unit intrinsic to the device used to measure it.
In order to eliminate environmental and extrinsic variation from the study, the correlation between the corneometric index of the treated area (face) and the control area (forearm) must be analyzed.
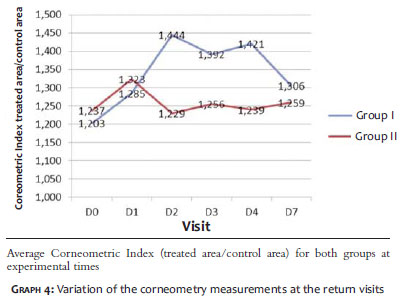
Graph 4 shows the variation of the corneometric index in different experimental times.
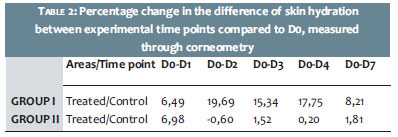
The percentage of variation in skin hydration between experimental times when compared to D0 (before the peel), is presented in Table 2. Negative values correspond to a reduction in skin hydration.
It is possible to observe (both in the table and graphically) that there is a significantly distinct behavior between the groups, with Group I's results being higher than those of Group II at all time points, except for the variation between D1 and D0, where the results were similar.
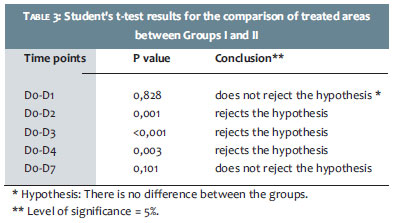
In order to compare the groups, Table 3 shows the statistical analysis of the corneometric index variation of the treated area/control area, relative to the baseline, between the various intermediate and final visits, using the Student's t-test.
It is important to note that there is a statistically significant difference in D2, D3, and D4 in the treated area, with Group II showing inferior results when compared to Group I.
3-Instrumental Effectiveness through Evaporimetry
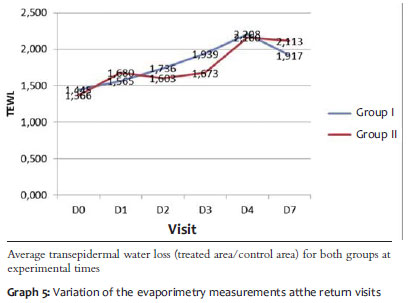
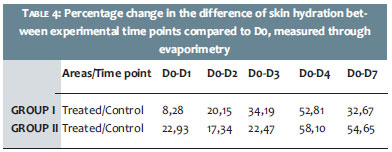
The results of the assessment of the transepidermal water loss of the skin through the evaporimetry technique are expressed in grams per square meter per hour (g/m2/h). In order to eliminate environmental and extrinsic variation from the study, it is necessary to study the correlation between the transepidermal water loss treatment in the treated area (face) and in the control area (forearm). Graph 5 shows the values for the transpidermal water loss (TEWL) in the different experimental times. The results of the percentage change in transepidermal water loss between the time points when compared with D0 (before the peeling) are presented in Table 4.
It is possible to observe increased evaporimetry measures in both groups. The development of that progression showed a distinct behavior between groups, being more marked in the early days in Group I, and more marked in the last days in Group II. At the end of the study, Group I had absolute and relative results superior to those of Group II.
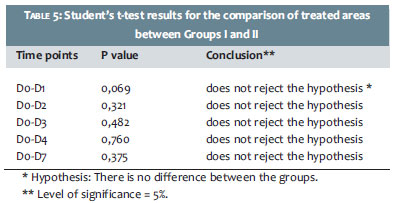
Table 5 shows the statistical analysis between the groups, in the variation of the transepidermal water loss of the treated area/control area in different visits, as compared to baseline, using the Student's t-test.
It is important to note that there was no statistically significant difference between the groups.
Superficial exfoliative procedures are common in the dermatological practice.
The purpose of these procedures is to promote a reduction in the thickness of the stratum corneum and/or deeper layers of the epidermis, inducing cell renewal and reducing the unaesthetic appearance of superficial dyschromic or hyperkeratotic lesions, leading to younger-looking skin.1
Of these procedures, the retinoic acid peel is the most frequent option among Brazilian dermatologists due to its practicality, low rate of adverse events, and the absence of restrictions on patients' daily activities, eliminating recuperation periods and time-off from work.3
Care after these procedures should include appropriate photoprotection (in order to reduce the risk of post-inflammatory hyperpigmentation) and the use of cutaneous barrier moisturizing and repairering agents (which can reduce desquamation, erythema and dryness, and at the same time, provide adequate hydration).
The present study was aimed at evaluating the ability of a topical product with 5% retinoic acid-used in the post-procedure period of peelings-to reduce signs and symptoms of exfoliation (erythema, dryness, and desquamation), simultaneously evaluating the water content and transepidermal water loss of the skin through instrumental measurements.
The study was conducted on a comparative basis, with the experimental group making use of the test product and standard sunscreen, while the control group used only the standard sunscreen.
The test product has moisturizing characteristics, exerting a reparative effect on the cutaneous barrier.
Fifty patients completed the study (per protocol population), with 24 of them having used both the sunscreen and the test product, and 26 the sunscreen only.
Regarding the clinical effects, it was possible to observe that the parameter erythema presented very low levels in both groups, (which is expected in patients who undergo retinoic acid peels), for being a superficial exfoliation. For that reason, no statistically significant difference between the groups was observed.
Desquamation is certainly the most observed event in patients undergoing retinoic acid peels, with dermatologist physicians often verifying this process peaking at between the third and fourth day of the procedure, possibly lasting from seven to ten days, depending on its intensity.
An expected progress of desquamation was found in the present study for both groups. Nevertheless, it was proved that Group I (treated with the test product and sunscreen) showed lower average desquamation as compared to Group II (treated only with sunscreen) at all time points, with statistical significance in the fourth and seventh days after the procedure. This demonstrates the added benefit that the use of the study product can offer in reducing desquamation.
Regarding the dryness sensation, it was possible to notice that the absolute rates for both groups were low. However when the two groups were compared, it was graphically possible to observe that Group I had lower average scores when compared to Group II. Statistical significance was not observed, probably due to the low values found in both groups.
The present study also sought to quantitatively evaluate the skin's hydration (carried out by measuring the skin's water content through corneometry) and transepidermal water loss (through evaporimetry).
When analyzing results for corneometry, it was possible to observe markedly distinct developments for the two groups.
It was evidenced that the treated group (Group I) showed superior results to those of Group II at all return visits, meaning that the use of a topical agent with moisturizing capacity can induce increased water content in the skin, resulting in improved hydration and contributing to a more effective recovery in the post-procedure period.
In the statistical evaluation between groups, it was observed that Group I was statistically superior to Group II in all intermediate visits (D2, D3, and D4), when compared to D0. In the first and last visits after the peeling procedure (D1 to D7), the improvement was not statistically significant.
The capacity to retain water, which is observed through the corneometry's results, demonstrates the test product's significant moisturizing capacity.
If the evaluation of the skin's water content (mainly promoted by products with high moisturizing and hygroscopicity properties) was carried out through corneometry assessments, the evaluation of transepidermal water loss was carried out by analyzing the corneum stratum's capacity for occlusion in preventing the evaporation of water from the skin's deeper layers to the environment.
Damaged skin-as it is after exfoliation-presents a rupture of the stratum corneum's structure, facilitating the evaporation of water, clearly evidenced by the evolution of evaporimetry curves of both groups.
Interestingly, the least favorable development observed in Group I (treated) in the early days of the study, is probably due to the greater supply of water on the skin's surface resulting from the use of the test product.
In other words, the supply of water provided by the hygroscopic power of the product (demonstrated in corneometry measurements) was the main factor for the increased evaporation of the water, noticed in the evaporimetry curves.
On subsequent days, however, the reparative effect of the test product on the barrier was evidenced through the improvement in the development of transepidermal water loss.
The use of the formulation containing the restorative complex ERC-5®, with hydrating and restorative action, demonstrated additional benefits in the post-procedure care of exfoliative techniques, resulting in the reduction of desquamation, promoting increased water content in the skin, and facilitating the structural recovery of the skin barrier.
1. Kadunc BV, Kede MPV, Guedes LS, Chizaki C, Bagatin E. Peelings quimícos. In: Kadunc BV, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de Cirurgia Dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier;2012. p. 311-33.
2. Bagatin E, Hassun K, Talarico S. Revisão sistemática sobre peelings químicos. Surg Cosmetic Dermatol 2009;1(2):37-46.
3. Cucé LC, Bertino MC, Scattone L, Birkenhauer MC.Tretinoin peeling. Dermatol Surg. 2001;27(1):12-4.
4. Cucé LC, Bertino M. Re: Regarding tretinoin peeling. Dermatol Surg. 2002;28(11):1097.
5. Khunger N, Sarkar R, Jain RK. Tretinoin peels versus glycolic acid peels in the treatment of melasma in dark-skinned patients. Dermatol Surg. 2004;30(5):756-60.
6. Kligman, DE. Regarding tretinoin peeling. Dermatol Surg. 2001;27(6):608.
7. Kligman DE, Sadiq I, Pagnoni A, Stoudemayer T, Kligman AM. High-strenght tretinoin: a method for rapid retinization of facial skin. J Am Acad Dermatol. 1998;39(2 pt 3):S93-7.
8. Kligman DE, Draelos ZD. High-strength tretinoin for rapid retinization of photoaged facial skin. Dermatol Surg. 2004;30(6):864-6.
9. Khunger N, IADVL Task Force. Standard guidelines of care for chemical peels. Indian J Dermatol Venereol Leprol. 2008;74(Suppl):S5-12.
10. Addor F. Terapêutica tópica em cosmiatria. In: Kadunc BV, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de Cirurgia Dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. p. 283-89.
11. Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332.
Study performed at the Medcin Instituto da Pele – São Paulo (SP), Brasil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}