


Frederico Hassin Sanchez1; Eduardo Lerner2
Keywords: EYELID NEOPLASMS; CARCINOMA, BASAL CELL; MOHS SURGERY; EAR CARTILAGE.
Various skin tumors can affect the lower eyelid and extend up to the tarsal region. Basal cell carcinoma (BCC) is the most common skin cancer, accounting for approximately 80-95% of all malign neoplasms of the eyelid.1,2
The treatment of choice for non-melanoma tumors of the eyelid is Mohs micrographic surgery (MMS), which achieves higher cure percentages with lower recurrence rates.3 It allows greater economy of healthy tissue around the tumor, favoring the preservation of important structures and surgical reconstruction.1-3
The lower eyelid has protective and lubricatingfunctions forthe eyeball, in addition to playing an important aesthetic role. Total-thickness defects of the eyelid require the reconstruction of two basic elements: the anterior lamella (which consists of skin, subcutaneous tissue, and orbicularis muscle), and the posterior lamella (which consists of the tarsus and palpebral conjunctiva).3,4 The lower tarsus is a dense conjunctive structure which lends mechanical support and stability to the eyelid,4 maintaining its shape and promoting the eyelid's adaptation to the curvature of the eye, in addition to containing the meibomian glands, which secrete a sebaceous material important for lubricating the cornea.1,3 It is connected medially to the medial canthal tendon (or ligament) and laterally to the lateral canthal ligament, both ofwhich insert into the orbital rim.
Tumors invading the tarsal plate promote total-thickness surgical defects of the eyelid, with defects ofup to one-thirdthe size of the total length of the lower eyelid generally capable of being closed. When tumors exceed this size, however, surgical reconstruction through the preparation of flaps and/or grafts is required, representing a major challenge for dermatologic surgeons.5,6
For reconstructing the posterior lamella, several graft options-such as jugal mucosa grafts, mucosal grafts from the hard palate,7,8 chondro-mucosal grafts from the nasal septum 8 and more recently, on an experimental level, nail plate xenografts in animal models for tarsal reconstruction 9-have been described.
The ear chondro-perichondrial graft was first described by Matsuo in 1987, using the auricular concha as the donor site for reconstructing the posterior lamella, combining it with a flap of adjacent skin to repair the anterior lamella.4 Many surgeons have used the auricular concha as the donor area since then. In the presentstudy, the authors propose the use of the ear helix as the donor site due to its reduced thickness, greater malleability of cartilage and, consequently, better adaptationto the eyeball, as compared to the auricular concha's cartilage.
To demonstrate the applicability of this eyelid reconstruction technique, with a chondro-perichondrial composite graft of the helix of the ear, when there is loss of the lower tarsus after MMS.
Six female patients who had undergone MMS for treatment of BCC in the lower eyelidwith invasion of the tarsus between January 2011 and April 2013, were selected. All underwent surgical reconstruction withcartilage of the ear helixand perichondrium grafts. The surgical procedures were performed at the Centro de Cirurgia Micrográfica do Rio de Janeiro, Brazil (Micrographic Surgery Center of Rio de Janeiro), a renowned private specialist center in MMS.
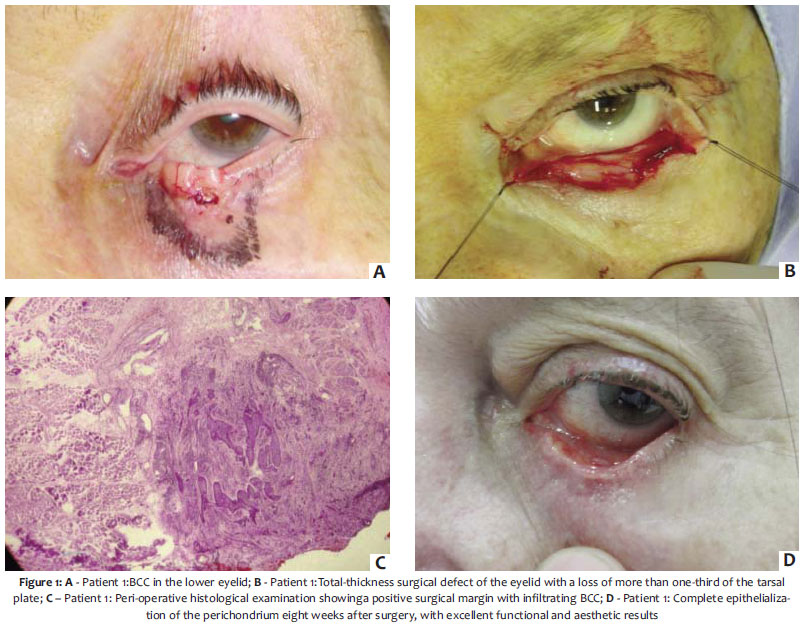
Four patients had recurrent BCC-with 1 having undergone operation twice using the traditional surgical method, with the tumor recurring less than one year from the last intervention (Figure 1). One of the patients had undergone topical chemotherapy with imiquimod and previous electrocautery (Figure 2). The other 2 had undergone prior surgical procedures, which, however, they were not able to describe with precision. All patients had their lesions previously biopsied, with the histological report describing nodular BCC in three cases, micronodular BCC in one case and infiltrative BCC in two cases. After excision of the lesions through MMS and successive stages of surgical increase of free margins, there was a loss of about three-quarters of the tarsal area in 3 patients (Figure 2) and approximately two-thirds of the lower tarsus in 3 patients (Figure 1).
The first phase of palpebral reconstruction was initiated-with the aim of reconstructing the posterior lamella. The surgical defect was duly measured, and the donor area in the ipsilateral ear helix marked with a dermographic pen. A small fusiform incision with the same length as that of the receiving area was carried out at the anterosuperior part of the helix of the ear, in the scaphoid fossa region, located between helix and anti-helix. Aband of cartilage with perichondrium, approximately 3 to 4mm wide, was carefully dissected and harvested to be grafted onto the lower eyelid. The band of cartilage that was partly covered with perichondrium was placed in contact with the eyeball (Figure 2). The graft was attached to the medial and lateral canthal tendons, which remained in the operated eyelid. The lower part of the graft was attachedto the retractor muscle of the lower eyelid using 7.0 poliglecrapone absorbable suture (Caprofyl®, Ethicon, Johnson & Johnson or Monocryl® Polysuture). Patients were asked to move the eyeball up and down in order to assess the perfect adaptation of the graft in contact with the eyeball, thereby avoiding keratitis and corneal ulceration.
After the attachment of the graft, the second phase of palpebral reconstruction was initiated, with the aim of reconstructing the anterior lamella. Usually, a myocutaneous flap or a simple advancement of the orbicularis muscle and skin remaining in the lower eyelid are positioned over the graft for nourishment purposes. In the present study, only 1 patient underwent a simple advancement flap to cover the graft. The other underwent reconstruction of the anterior lamella with the simple displacement of the tissue remaining in the lower eyelid. The skin was sutured to the superior part of the graft. A Frost suture was carried out to prevent retraction and the formation of ectropion. This type of suture is indicated when excessive traction occurs in the skin (Figure 2).
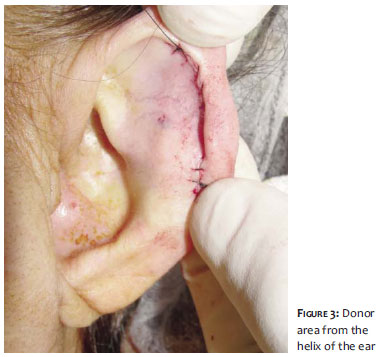
The donor area in the ear's scaphoid fossa was primarily sutured with nylon monofilament, leaving a virtually unnoticeable scar (Figure 3).
The patients were instructed to use lubricant eye drops several times a day and retinol acetate and chloramphenicol based ophthalmic ointment overnight. This decreases the discomfort caused by the friction of the perichondrium with the eyeball andalso red-eye syndrome, which occurs in the first weeks.
During MMS, histological analysis showed BCC with a mixed histologic pattern in 3 patients (in a nodular and infiltrative pattern (Figure 1) in the same lesion), 1 with a purely nodular pattern, and 2 patients whose tumors were not observedduring surgery due to the fact that free margins were obtained in the first surgical stage. Surgical margins free from neoplasms were obtained after two amplification stages in 3 patients, and three required in 1 patient. All patients developed with complete adaptation of the chondro-perichondrial graft, with minimal ocular discomfort in the first few weeks, and total transformation of the perichondrial tissue in contact with the eyeball into conjunctiva (through metaplasia), after eight weeks (Figure 1).
There was a slight retraction of the lower eyelid in all cases, causing subtle scleral show, but at an aesthetically acceptable level and with no degree of ectropion (Figure 2). None of the patients had recurrence as ofthe date the present article was written, with a post-operative follow-up time of 6 to 32 months.
MMS has confirmed its importance as the gold standard in the treatment of palpebral tumors due to the fact that it allows a precise histological control of surgical margins.
Several techniques have been described for the reconstruction of the posterior lamella. Mucosal only grafts, such as in the case of hard palate grafts, do not provide sufficient mechanical stability withthe occurrence of large defects of the lamella.4,5 Composite grafts of cartilage/mucosa from the nasal septum are classically described in the literature with good results, but nevertheless they are technically difficult to harvestfrom the donor area.4,5
Chondro-perichondrial grafts from the auricular concha are also described with good results, however, due to their greater thickness, the conchal cartilage is less malleable, hampering perfect adaptation to the eyeball. Therefore, the authors believe that chondro-perichondrial grafts from the helix of the ear's cartilage are a good option, especially because they are easy to perform and adapt well to the eyeball. The technique described in the present study dismisses the need for a mucosal graft, since the perichondrium that remains in direct contact with the eyeball undergoes metaplasia and turns into a tissue similar to that of the conjunctiva. These findings are consistent with publications that demonstrate the importance of the perichondrium in the epithelialization process and the speed of transformation of the tissue into conjunctiva, which is superior when compared to cartilage only, perichondrium-free grafts.10,11
Furthermore, the chondro-perichondrial graft from the ear helix satisfactorily replaces the lost tarsal tissue, providing mechanical support and allowing foradequate palpebral mobilization and occlusion.4,11
Although the present study has worked with a small sample size, the technique described proved an excellent choice for extensive palpebral reconstructions in cases involving loss of the posterior lamella. This is due to the fact that it provided adequate stability and mobility to the eyelid, with the complete transformation of the perichondrium into conjunctival tissue in a few weeks, with minimal post-operative discomfort, and with excellent functional and aesthetic results.
1. Harvey DT, Taylor RS, Itani KM, Loewinger RJ. Mohs Micrographic Surgery of the Eyelid: An Overview of Anatomy, Pathophysiology, and Reconstruction Options. Dermatol Surg. 2013;39(5):673-97.
2. Deprez M, Uffer S. Clinicopathological features of eyelid skin tumors. A retrospective study of 5504 cases and review of literature. Am J Dermatopathol. 2009;31(3):256-62.
3. Ahmad J, Mathes DW, Itani KM. Reconstruction of the eyelids after Mohs surgery. Semin Plast Surg. 2008;22(4):306-1
4. Parodi PC, Faini G, De Biasio F, Rampino Cordaro E, Guarneri GF, Miani F. Full-thickness lower eyelid reconstruction with a conchal chondro-perichondral graft and local coverage with Mio-cutaneous flaps--our divisional experience. J Oral Maxillofac Surg. 2008;66(9):1826-32.
5. Stein JD, Antonyshyn OM. Aesthetic eyelid reconstruction. Clin Plast Surg. 2009;36(3):379-97.
6. Jewett BS, Shocley WW. Reconstructive options for periocular defects. Otolaryngol Clin North Am. 2001;34(3):601-25.
7. Miyamoto J, Nakajima T, Nagasao T, Konno E, Okabe K, Tanaka T, et. al. Full-thickness reconstruction of the eyelid with rotation flap based on orbicularis oculi muscle and palatal mucosal graft: long-term results in 12 cases. J Plast Reconstr Aesthet Surg. 2009;62(11):1389-94.
8. Moesen I, Paridaens D. A technique for the reconstruction of lower eyelid marginal defects.Br J Ophthalmol. 2007;91(12):1695-7.
9. Özkaya Ö, Karşidag S, Egemen O, Akçal AÖ, Şirvan S, Kabukçuoglu F. Comparative analysis of the nail xenografts with cartilage autografts in eyelid reconstruction. J Craniofac Surg. 2012;23(4):1028-31.
10. Nigro MV, et. al.Comparative analysis of the influence of perichondrium on conjunctival epithelialization on conchal cartilage grafts in eyelid reconstruction: experimental study in rabbits. Plast Reconstr Surg. 2009 Jan;123(1):55-63
11. Knop E, Korb DR, Blackie CA, Knop N. The lid margin is an underestimated structure for preservation of ocular surface health and development of dry eye disease. Dev Ophthalmol. 2010;45:108-22.
Study performed at the Centro de Cirurgia Micrográfica do Rio de Janeiro-Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}