


Carlos Roberto Antonio1; João Roberto Antonio2; Guilherme Bueno de Oliveira3; Lívia Arroyo Trídico4; Mariana Perez Borim5
Keywords: ACNE VULGARIS; LASERS; LASER THERAPY.
Acne is one of the most common dermatological conditions, accounting for 30% of dermatological complaints.1-3 It affects most people at some point in their life, being prevalent in adolescents and affecting 85% of individuals between 12 and 24 years old.4,5
It is an inflammatory dermatosis of the pilosebaceous unit, whose pathogenesis is multifactorial. The main contributing factors for its development include follicular hyperkeratinization, increased production of sebum by the sebaceous glands, bacterial colonization of the follicle by Propionibacterium acnes (P. acnes) and the release of inflammatory mediators in the follicle and adjacent dermis.6
Drug options can be topical or systemic. The treatment of mild acne is topical, encompassing retinoids, benzoyl peroxide, azelaic acid, and topical antibiotics, and demands frequent applications. Moderate acne requires long-term treatment with oral antibiotics, and may be associated with bacterial resistance. Severe, nodular cystic acne requires the use of oral isotretinoin, a medication associated with significant advancement in the treatment of acne, however it can present side effects such as teratogenicity, lip dryness, dry skin, epistaxis, erythema and/or dermatitis on the face, myalgia, constipation, and elevation of plasmatic lipids, in addition to the possibility of resistance to the action of active principles.2,7
Despite the availability of various treatments, there are cases of difficult management, especially the most severe, such as nodularcystic acne, where in spite of the new therapies, lesions often continue to arise.8,9 In such extreme cases, light and laser-based treatments have become an alternative to topical and oral medications in recent years, since they seem to reduce inflammatory acne lesions, acting on the major physio-pathological factors.2
Some studies have reported success in treating inflammatory acne with laser therapy such as10-12 intense pulsed light (IPL), dye lasers (PDL),13,14 diode lasers,15 KTP (potassium titanyl phosphate), erbium glass laser, radiofrequency, and photodynamic therapy1,2 being cited as examples. Positive results obtained with laser therapy can be explained by the action on the P. acnes bacteria and the inflammatory activity by the sebaceous gland.2
In light of the success of various types of lasers in treating acne16,17 the authors sought to evaluate the use of a new non-ablative fractional technology in nodularcystic acne, the 1,340nm Nd:YAP laser (Neodimiun:Ytrium Aluminum Perovskite), since itsindication in acne has up until now been restricted to the correction of scars.16 The present study was aimed at investigating the benefits of this laser in the treatment of difficult to control, oral isotretinoin treatment-resistant acne.
Patients above 14 years of age, with nodularcystic acne, treated at the Acne Ambulatory of the Dermatological Surgery and Laser Therapy Unit, Dermatology Department of the Faculdade de Medicina de São José do Rio Preto (FAMERP),São Paulo, Brazil, took part in a clinical interventionist study, from September 2012 to June 2013. Inclusion criteria included presence of nodular cystic acne active in the facial region, resistant to oral isotretinoin; absence of the use of any other treatment for acne for at least 90 days. Exclusion criteria included: pregnancy, patients under 14-years-old, patients bearing any other type of infection or skin condition or herpes active in the studied region, and those with a sensitivity to light. Those who met the selection criteria and agreed to participate in the research project signed a Free and Informed Term of Consent. The project was approved by the Ethics Committee of FAMERP.
Each patient underwent a variable number of sessions (two to six), according to clinical indication and at 28-30 day intervals. The laser device used was the 1,340nm Nd:YAP (Etherea®, Industra Technologies Indústria e Comércio Ltda, São Carlos,SP, Brazil), 100mtz (thermal microzones), energy = 100mJ, 3ms and 8mm tip. The patient received one application of this fractional laser per session. The anatomical pathological examination was performed through the incisional biopsy technique, using a 3mm punch. This procedure was carried out before the treatment and after the last laser session,at the same location. The number of sessions was determined by the patient's clinical improvement.
The evaluation of outcomes was performed through comparison of photographs taken before and after the treatment with fractional laser for each patient. The images were analyzed by two dermatologist physicians not related to the study and who were responsible for assigning scores from 0 to 3 (0 = worsening, 1 = absence of improvement, 2 = moderate improvement, 3 = significant improvement), after comparing the two photographs. The patients also provided information on their degree of satisfaction with the treatment (0 = dissatisfied, 1 = somewhat satisfied, 2 = satisfied, 3 = very satisfied). In addition, the lesions were counted on day zero and after the last session.
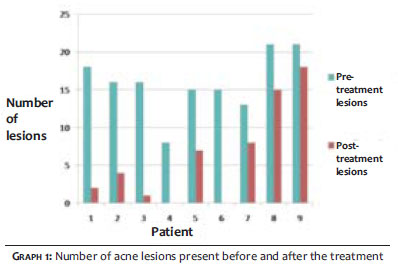
Nine male patients underwent laser treatment for nodular cystic acne resistant to isotretinoin. The mean value of the patients' age was 20 (range = 16 to 27). The patients had an average of 16 lesions in the face before the treatment (range = 8 to 21), with standard deviation.3,7,8
The number of laser sessions performed on the patients ranged from 2 to 6 (2 sessions in one patient, 3 sessions in three patients, 4 sessions in four patients and 6 sessions in one patient), according to clinical indication. As a result, after the treatment, six acne lesions lingered on average, ranging from 0 to 18, with a standard deviation of 6. 20 (Graph 1).
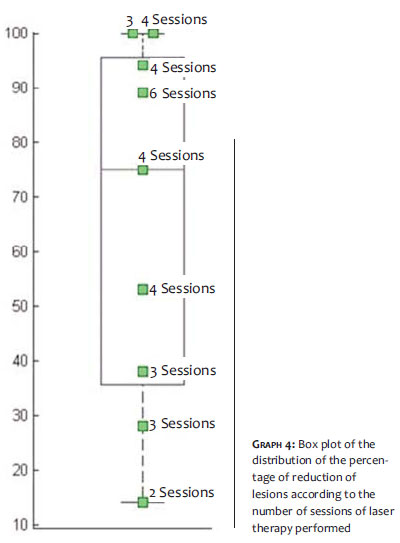
Considering the average number of lesions existing before the treatment (16 lesions) and comparingit to the average number of lesions after the treatment (6 lesions), it was observed that there was an average decrease of 65% of lesions. The highest percentage of lesion reduction was found in patients who had at least 4 laser sessions, with an average reduction of 82%, while in those who underwent a maximum of 3 sessions, lesions reduced on average 45%.
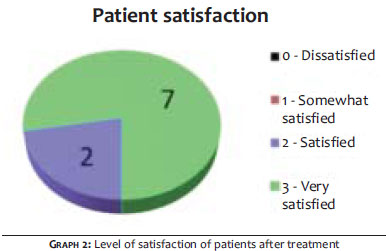
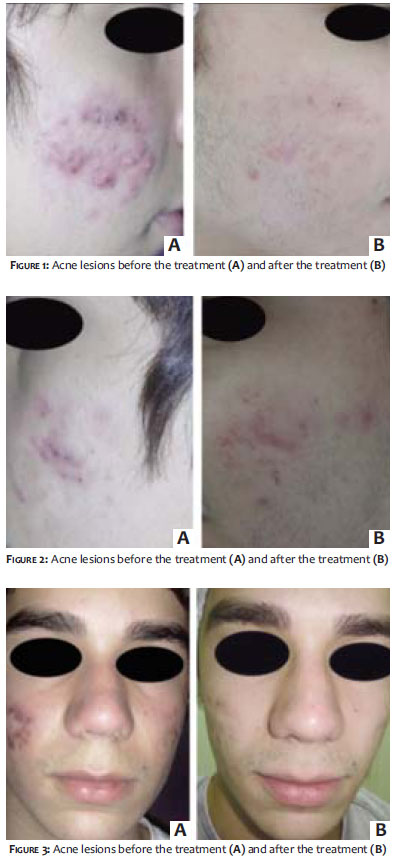
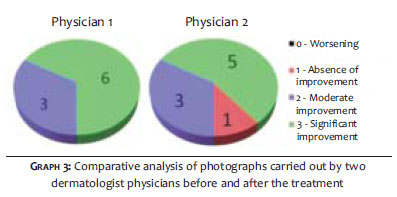
The degree of satisfaction assessed subjectively by the patients was as follows: 7 patients reported being very satisfied (degree of satisfaction 3), 2 patients reported being satisfied (degree of satisfaction 2) and no patient was somewhat satisfied or dissatisfied (degrees of satisfaction 1 and 0, respectively) (Graph 2). The objective analysis of photographs (Figures 1 to 3) carried out by the two dermatologist physicians not related to the study was rated as follows: Physician 1 rated 6 patients with significant improvement and 3 patients with moderate improvement. Physician 2 rated 5 patients with significant improvement, 3 patients with moderate improvement and 1 patient with absence of improvement. (Graph 3) The physicians had differing opinions only regarding 2 patients, with one of them being rated with significant improvement by Physician 1 and moderate improvement by Physician 2,while the other was rated with moderate improvement by Physician 1 and absence of improvement by Physician 2. In aggregate terms, the physicians had the same opinion in 78% of patients, with Physician 2 rating photographs of two patients with a lesser degree of improvement when compared tothe rating attributed by Physician1 to the same patients.
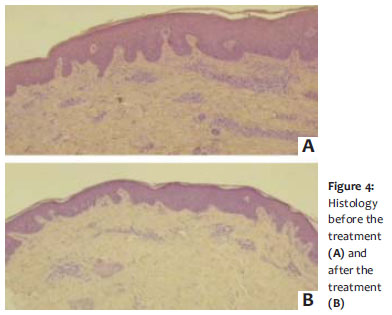
Before the treatment, the anatomical pathological examination revealed lymphocytic inflammatory infiltrate and thick and disorganized collagen fibers. After the last session, it showed a significant reduction in the inflammatory infiltrate and that collagen fibers were organized (Figure 4).
As an adverse reaction to the treatment, the 9 patients presented only pain and mild erythema after the application of non-ablative fractional laser. No severe, adverse effects were observed in any of the patients.
Laser therapy for inflammatory acne is an alternative treatment mainly for patients who do not respond to conventional treatment. It is associated with minimal side effects, and is therefore an option for patients who have moderate and severe acne.18 According to Rai and Natarajan, advances in laser therapy for inflammatory acne have been reported. Notwithstanding, the development of clinical studies is necessary in order to determine its effectiveness in the different types of laser therapy.18
The present study demonstrated that there was a significant reduction in the number of acne lesions after treatment with 1,340nm Nd:YAP laser. The reduction in the number of lesions was on average 65%. In addition, the greater the number of sessions performed, the higher the percentage of reduction, since the patients who underwent more than four sessions showed an 82% reduction in the number of lesions on average, evidencing an important response to the therapy (Graph 4). It was also possible to observe that two patients had 100% improvement in the number of lesions, meaning that it was not possible to observe nodular cystic acne lesions in those patients after the laser treatment.
Due to the psychosocial impact caused by acne,19,20 the present study showed the relevance in asking about the degree of patient satisfaction, for the majority reported great satisfaction with the treatment, and no patient was somewhat satisfied or unsatisfied. It was possible to note that, in addition to the reduction in the number of lesions, the use of fractional laser also provided physical and psychological well-being.
From a medical standpoint, the therapy with fractional laser proved effective in treating acne, for in the evaluation performed by dermatologist physicians not related to the study, very close and positive opinions were obtained. Another factor contributing to the efficacy was an important histological improvement after the laser therapy, with the decrease of inflammatory infiltrate and the reorganization of collagen fibers. Furthermore, no significant adverse effects were observed, ensuring the method's safety.
Nodular cystic acne resistant to isotretinoin is a condition capable of having psychosocial impacts on patients, requiring effective methods for its management. The authors concluded that the treatment with non-ablative fractional 1,340nm Nd:YAP laser was effective and safe for that indication and can be a good option. Further studies are necessary in order to consolidate the authors' conclusion.
1. Kim RH, Armstrong AW. Current state of acne treatment: highlighting lasers, photodynamic therapy, and chemical peels. Dermatol Online J. 2011;17(3):2.
2. Jih MH, Kimyai-Asadi A. Laser treatment of acne vulgaris. Semin Plast Surg.2007;21(3):167-74.
3. Gold MH. Efficacy of lasers and PDT for the treatment of acne vulgaris. Skin Therapy Lett. 2008 Jan;12(10):1-6,9.
4. Leyden JJ. A review of the use of combination therapies for the treatment of acne vulgaris. J Am Acad Dermatol. 2003;49(3 Suppl):S200-10.
5. Oberemok SS, Shalita AR. Acne vulgaris, I: pathogenesis and diagnosis. Cutis. 2002;70(2):101-5.
6. Gollnick H. Current concepts of the pathogenesis of acne: implications for drug treatment. Drugs. 2003;63(15):1579-96.
7. Montagner S, Costa A. Diretrizes modernas no tratamento da acne vulgar: da abordagem inicial à manutenção dos benefícios clínicos. Surg Cosmet Dermatol. 2010;2(3):205-13.
8. Ramos e Silva M, Costantini SE. Clasificación, formas clínicas y variantes. In: Kaminsky A. Acné. Un enfoque global. Buenos Aires: Pinter; 2007.
9. Seaton ED, Charakida A, Mouser PE, Grace I, Clement RM, Chu AC. Pulseddye laser treatment for inflammatory acne vulgaris: randomised controlled trial. Lancet. 2003;362(9393):1347-52.
10. Elman M, Lask G. The role of pulsed light and heat energy (LHE) in acne clearance. J Cosmet Laser Ther. 2004;6(2):91-5.
11. Morton CA, Scholefield RD, Whitehurst C, Birch J. An open study to determine the efficacy of blue light in the treatment of mild to moderate acne. J Dermatolog Treat. 2005;16(4):219-23.
12. Lee M C. Aura 532 nm laser for acne vulgaris-3-year experience. New Orleans, LA: Presented at: 2003 ASDS-ACMMSCO Combined Annual Meeting; October 9-12,2003.
13. Orringer JS, Kang S, Hamilton T, Schumacher W, Cho S, Hammerberg C, Fisher GJ,Karimipour DJ, Johnson TM, Voorhees JJ. Treatment of acne vulgaris with a pulsed dye laser: a randomized controlled trial. JAMA. 2004;291(23):2834-9.
14. Glaich AS, Friedman PM, Jih MH, Goldberg LH. Treatment of inflammatory facial acne vulgaris with combination 595-nm pulsed-dye laser with dynamic-cooling-device and 1,450-nm diode laser. Lasers Surg Med. 2006;38(3):177-80.
15. Jih MH, Friedman PM, Goldberg LH, Robles M, Glaich AS, Kimyai-Asadi A. The 1450-nm diode laser for facial inflammatory acne vulgaris: dose-response and 12-month follow-up study. J Am Acad Dermatol. 2006;55(1):80-7.
16. Hasegawa T, Matsukura T, Hirasawa Y, Otsuki A, Tsuchihashi H, Niwa Y, Okuma K,Ogawa H, Ikeda S. Acne conglobata successfully treated by fractional laser after CO laser abrasion of cysts combined with topical tretinoin. J Dermatol. 2009;36(2):118-9.
17. Paschoal FM, Ismael APPB. A ação da luz no tratamento da acne vulgar. Surg Cosmet Dermatol. 2010;2(2)117-23.
18. Rai R, Natarajan K. Laser and light based treatments of acne. Indian J Dermatol Venereol Leprol. 2013;79(3):300-9.
19. Al Robaee, AA., Assessment of general health of life in patients with acne using a validated generic questionnaire. Acta Dermatovenerol Alp Panonica Adriat, 2009;18(4):157-64.
20. Clark SM, Goulden V, Finlay AY, Cunliffe WJ. The psychological and social impact of acne: a comparison study using three acne disability questionnaires. Br J Dermatol. 1997;137(Supplement 50):41.
Study performed at the Faculdade de Medicina de São José do Rio Preto (FAMERP)-São José do Rio Preto (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}