


Rubens Pontello Júnior1; Rogério Nabor Kondo2; Ricardo Pontello3
The dorsum of the hand is home to tumors that often require a surgical approach. Due to limited cutaneous mobility, wide surgical wounds become a challenge to dermatologic surgeons. The authors report the case of a patient with a tumor in the dorsal region of the left hand that, after removal with a safety margin, resulted in a wide surgical wound, and in the choice of reconstruction with an A-T flap. Six months later, the patient was cured, with total preservation of the hand's mobility and excellent aesthetic results. The concept of using flaps for closing wide surgical wounds, whenever possible, is reinforced.
Keywords: HAND, NEOPLASMS, SURGICAL FLAPS.
The dorsum of the hands often house tumors that require a surgical approach. Due to limited cutaneous mobility, wide surgical wounds become a challenge to dermatological surgeons. The present article describes the use of the A-T flap, performed in a single surgical event by a single surgeon, as an option for closing surgical wounds on the dorsum of the hand.
A 54-year-old male patient presented a three-month history of progressive growth of a lesion on the dorsum of the left hand. Clinical examination showed hardened tumoration with central corneum plug, 3.6 cm in diameter, suggestive of keratoacanthoma. (Figure 1)
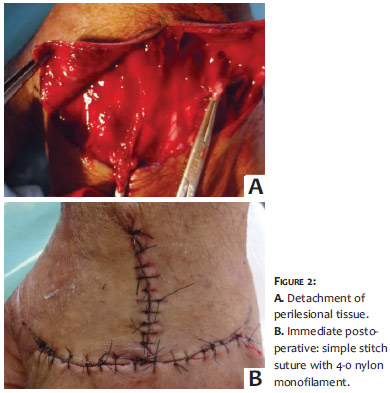
After demarcating the tumor with a 3.0 mm safety margin, plans were made for reconstruction with the A-T advancement flap (Figure 1). After local infiltrative anesthesia of 2% lidocaine with vasoconstrictor, the total excision of the lesion was carried out with a minimum margin of 3.0 mm. It was followed by perilesional cutaneous divulsion, avoiding accidental cut nerves or tendons, and the preparation of the flap, with an approximation of the borders and suture with 4-0 nylon monofilament (Figure 2).
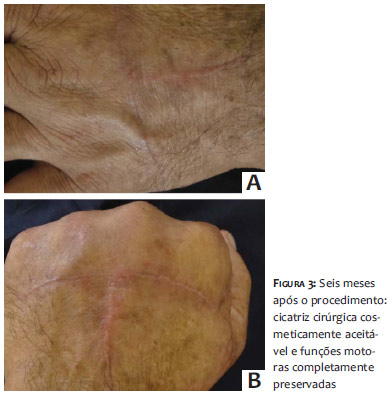
The patient returned two weeks after, showing adequate healing, which allowed for the removal of all stitches. Despite this, some limitation in the flexion of the fingers was verified. The patient was then referred for motor physical therapy, having been instructed to frequently and gradually flex and extend the fingers, immersed in water, in addition to taking oral prednisone in an anti-inflammatory dose (equivalent to 0.5 mg/kg*day, for seven days). The one-week re-assessment of the patient showed that the movement had been completely restored. After six months, the patient showed excellent aesthetic and functional recovery, with complete patient satisfaction and no signs of tumor recurrence (Figure 3).
The histologic examination of the specimen removed surgically confirmed the initial hypothesis of keratoacanthoma.
Extensive surgical wounds on the dorsum of the hand often create a challenge for dermatologic surgeons. When primary closure is not feasible, flaps or skin grafts are alternative techniques. Even though free grafts provide good results on the dorsum of the hands, this technique has the disadvantage of requiring a distant donor area.1, 2 Whenever possible, a decision is made for the use of flaps-which use adjacent tissue, following the "like-forlike" rule, leading to better esthetic results 2-or the confection of rotation flaps for surgical wounds on the dorsum of the hands, recently introduced by Cardoso et al., a method that preserves functional capabilities and aesthetics.3
The A-T flap is classified as an advancement flap, and is chosen when the greater degree of sagging is located along the defect's shorter axis (as in the present case) or when the distortion of structures adjacent to the borders of the defect is undesirable (as in the case of lesions above the eyebrow). It is worth noting that extensive undermining is not recommended, for despite providing a greater amount of tissue without tension, it can give rise to the interruption of blood supply to the vertical component arising from the deep plexus, thus compromising the perfusion of the flap's distal rim.4 The use of simple divulsion for detaching the surgical margins has preserved axial vascularization, avoiding areas of necrosis in the flap even in the most distal region.
The technique has proved useful for the reconstruction of surgical wounds in the central region of the dorsum of the hands, where the flap's borders advance naturally.
The procedure described in this paper was performed in a straightforward manner, requiring only the use of a local anesthetic. Based on the authors' literature search, it is the first report of an A-T advancement flap being used for the closure of a surgical wound on the dorsum of the hands. The conclusion is that the described technique allows for rapid reconstruction, distributing the tension of the closure over a larger surface area while preserving the functionality and aesthetic. The technique is therefore identified as a good option for large wounds that have their longest vertical axis located in the central region of the dorsum of the hand.
1. Chao JD, Huang JM, Wiedrich TA. Local hand flaps. J Am Soc Surg. 2001;1(1):25-44.
2. Hurren JS, Cormack GC. The application of the rotation flap to the dorsum of the hand. Br J Plast Surg. 2000;53(6):491-4.
3. Cardoso PM, Santos P, Azevedo F. Retalho de rotação para fechamento de defeitos cirúrgicos nos dorsos das mãos. Surg Cosmet Dermatol. 2011;3(4):348-9.
4. Khouri RK; Nouri K; Khouri SL Retalhos cutâneos. In: Khouri S.L; Nouri K. Técnicas em cirurgia dermatológica. Rio de Janeiro: DiLivros Editora. 2005 p. 141.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}