


Alessandra Yoradjian1; Luciana C. Maluf Azevedo1; Luciana Cattini1; Ricardo Alves Basso2; Deborah Krutman Zveibil3; Francisco Macedo Paschoal4
Keywords: PYOGENIC GRANULOMA, DERMOSCOPY, MELANOMA.
Pyogenic granuloma is a common, benign, acquired vascular proliferation that affects the skin and mucous membranes.1-4 It usually presents as a single nodule or papule of rapid growth, bleeds easily with only a minimum of trauma, and may develop into an ulcer.1-4 It occurs commonly on the hands (especially on the fingers), face, lips and feet, however it can also involve other body sites such as the trunk and perianal mucosa.1-4
It was first described by Poncet and Dor in 1897, being called botryomycose humaine. The expression pyogenic granuloma was subsequently proposed by Hartzel in 1904, however other names, such as telangiectaticum granuloma, granuloma pediculatum and lobular capillary hemangioma have emerged. The denomination pyogenic granuloma was established in the United States, for it was believed to be the term that best described the pathologic process.1 However, these lesions are neither pyogenic (for it was not possible to prove the involvement of bacterial infection) nor granulomatous. According to Zaballos et al., the best designation for these lesions would be lobular capillary hemangioma, which, however, is still subject to debate.5
The lesion seems to be reactive, but its exact mechanism of onset is uncertain. One possibility is that it might occur due to a reactional hyperproliferative vascular response to a variety of stimuli such as infectious organisms, cutaneous trauma, hormonal factors, and drug therapy such as retinoids.1,4,5
Histologically, it shows capillary proliferation close to the surface, with a radiated pattern and a loose edematous collagen matrix, with the epidermis extending down into the base of the lesion, producing an epidermal collarette and in some cases causing the formation of peduncles. Mixed inflammatory infiltrate can occur-and fibrosis with septa that intersect the lesion, producing a lobular pattern that can take place in more severe cases.1
Its diagnosis is usually facilitated by analysis of history and clinical aspects, however it may mimic benign or malignant tumors in some situations.1-4,6 The main differential diagnoses are: keratoacanthoma, squamous cell carcinoma, basal cell carcinoma, inflamed seborrheic keratosis, common warts, melanocytic nevus, Spitz nevus, metastatic carcinoma, Kaposi's sarcoma, true hemangioma, vascular tumors of intermediate malignancy, and amelanotic melanoma.1
Previous studies have found 38% of cases incorrectlydiagnosed.1-3 Some papers focusing on dermoscopy were designed to better study the characteristics of pyogenic granulomas with a view to facilitating the differentiation from similar lesions. Dermoscopy has been a useful tool in the diagnosis of not only pigmented but also nonpigmented lesions due to the capacity of recognition of vascular patterns not visible to the naked eye.7 Particularly in the case of pyogenic granulomas, dermoscopic patterns have been described.
In the present article, two cases of pyogenic granuloma with atypical clinical manifestations are presented with their dermoscopic images, followed by a review of the literature on the subject.
Patient 1: female, mulatto, 60-years-old, with a friable, asymptomatic tumor in the dorsal region of the third left finger for six months, recurring after previous treatments (surgical excision and electrocoagulation) (Figure 1).
Patient 2: female, Caucasian, 76-years-old, bearing a vegetating lesion with necrotic surface on the dorsum of the left hand, and wine colored satellite papules reaching the palm, for six months, with pain and bleeding (Figure 2).
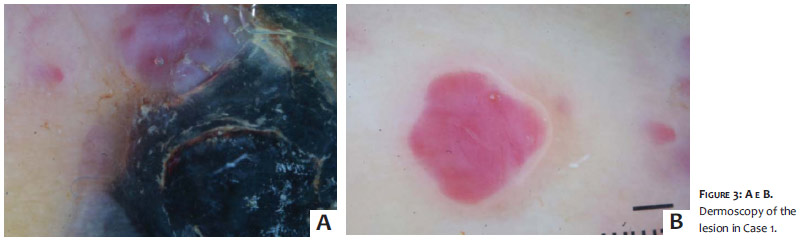
Dermoscopy of the lesions showed a well-delimited raised nodular lesion, without melanin pigment, and characteristics compatible with melanocytic lesion (Figures 3 and 4).
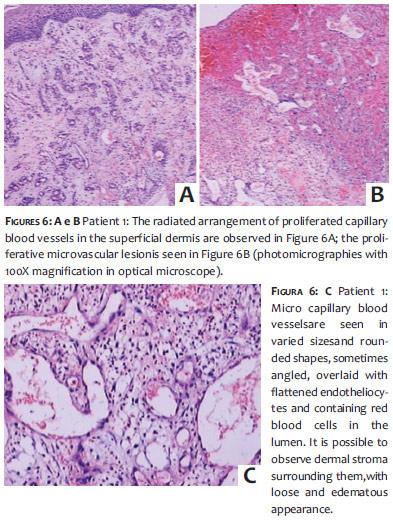
Histological examination of Patient 1 revealed a raised, well-defined nodular lesion with conservation of epidermal areas and others with epidermal ulceration, inflammatory mononuclear cells, lymphocytes, intact and lysed polymorphonuclear neutrophils, with recent hemorrhage in the papillary dermis just beneath the ulcerated areas. In the deep and superficial papillary dermis, various capillary blood vessels were identified, proliferating in lobular arrangement, with thin walls overlaid by flattened endotheliocytes without atypia and containing red blood cells in the lumen.Capillaries had a radiated layout with some elongated vessels and others displaying obtuse angles (Figures 5 and 6).
A histopathological examination of Patient 2 revealed a lesion similar to that of Patient 1, in its nodular and lobulated arrangement, formed by a microvascular blood proliferative lesion with capillaries in a radiated disposition, and endothelial overlay without atypia. In deeper planes, however, an increase of endothelial cellularity showing elongated nuclei with fusiform aspect and mild nuclear atypia, such as hyperchromatism, was verified, without necrosis or mitosis. Despite the existence of other smaller satellite lesions (similar to the latter) on the hand of the patient, the final diagnosis was that of pyogenic granuloma (Figure 7).
The photograph not featuring a magnified view of the biopsy taken during the histological examination of Patient 2's cutaneous lesion, shows a full view of the lesion with nodular area. In the photomicrography, the images show the lesion just beneath the epidermis. These areas show less cellularity and contain a more recent hemorrhage, with the most differentiated area exhibiting froth with small blood capillaries, an aspect of lobular capillary hemangioma. The deepest areas of the lesion, in the subcutaneous tissue region, are hypercellular areas composed of fusiform cells with mild to moderate atypia, rose-colored cytoplasm, and elongated and hyperchromatic nuclei. This means that these are differentiated areas-characteristic of hemangioendotheliomas-allowing a differential diagnosis with the low-grade angiosarcoma. The less cellular, more differentiated area is observed with greater magnification. (Figure 7)
The cases described in the present article show pyogenic granuloma lesions with atypical and exuberant clinical presentation. Due to the fact that it was not possible to clinically exclude malignancy, patients underwent biopsy for histological analysis. First, however, a dermoscopic examination without criteria for melanocytic lesions was carried out. Homogeneous red areas, white rail lines intersecting the lesion, white collarette, ulceration, hemorrhage crusting, and isolated lesions showing pinpoint vessels, were observed. Finally, the histological examination demonstrated the presence of benign lesions.
Pyogenic granulomas are benign acquired capillary lesions that affect the skin and mucous membranes, and whose pathogenesis is not yet explained. It is suggested that it might result from mechanical trauma, however the participation of hormonal factors, medications (retinoids), arteriovenous malformations, viral oncogenes and other microorganisms, as well as of angiogenic growth factors have also been proposed.
Usually solitary, painless, pyogenic granulomas may have different diameters-from a few millimeters to centimeters-and can ulcerate and bleed.1-5
Due to the fact that some nodular melanomas mimic pyogenic granulomas, biopsy is always required for anatomopathological analyses, with an aim at avoiding the delay of diagnosis and improving the prognosis.1,7
Dermoscopy is an in vivo, noninvasive technique, used for pigmented and vascular lesions that can help when there is suspicion of pyogenic granuloma, increasing diagnostic accuracy even in cases that are clinically atypical.1-3,5,7 More recently, studies on dermoscopic patterns of pyogenic granuloma have been carried out in order to assist in the differential diagnosis with amelanotic melanoma.3
Dermoscopy should be conducted without pressure to avoid compromising vascular visualization. In the absence of criteria for melanocytic lesions, it can evidence from homogeneous red areas to well-defined vascular structures.3,5,8 The main characteristics are homogeneous red areas (observed in more than 90% of cases), white collarette (80% of cases), white rail lines that intersect the lesion (30-45% of cases), ulceration (46% of cases) and vascular structures (45% of cases).1-6,8 No isolated characteristic was 100% specific.3 As a consequence, through observations of dermoscopic findings in pyogenic granulomas, Zaballos et al. recently defined 7 dermoscopic patterns for those lesions.1-3 According to the combination of these characteristics present in the lesion, the patterns are: 1-3 (Figure 8):
P1: homogeneous red area + white collarette
P2: homogeneous red area + white rail lines
P3: homogeneous red area + vascular structures
P4: homogeneous red area + white rail lines + white collarette
P5: homogeneous red area + white collarette + vascular structures
P6: homogeneous red area + white rail lines + vascular structures
P7: homogeneous red area + white collarette + white rail lines + vascular structures
The patients studied had had multiple lesions grouped in a single body segment. In those cases, the presence of a combination of the patterns described abovecould be observed, due to the presence of multiple lesions, each with a specific pattern.
The homogeneous red area corresponds to the area with absence of structure, whose color varies from red to whitish-red. It is attributed to the presence of numerous small capillaries or proliferative vessels arranged in a myxoid stroma.3,5 It is quite common in pyogenic granulomas, however it is not a finding specific only to this type, for it is also common in amelanotic melanomas.
In histology, the white collarette corresponds to the attached hyperplastic epithelium that fully or partially embraces the lesion in theperiphery.3,5 It is the most specific structure of pyogenic granulomas. The white rail lines correspond to fibrous septa that surround the capillary tufts or lobules in the older lesions.3,5 In Patient 1, on whom both conventional dermoscopy and polarized light had been performed, it could be observed that the white rail lines became more apparent with the use of polarization (Figures 4B and 4C).
Regarding the vessels that can be observed, the following arrangements have been described: pinpoint, irregular linear, polymorphic/atypical, telangiectasia, and hair-pin-like. In the cases described in the present study, the vessels were minimally evident, not constituting a relevant finding despite the exuberance of the lesions.
Ulcerations were found to be common to many other skin lesions and were not included in the criteria.
In the study carried out by Zaballos et al., the pattern most frequently associated with pyogenic granuloma was the P4. Fifty-two percent of pyogenic granulomas showed one of three patterns: P1, P4, and P7, with no amelanotic melanoma having presented in any of them.3
In addition to atypical vessels, other findings, such as the whitish-blue veil, blotches, and hematic crusts-all of which are common characteristics of melanomas-were also found in some cases of pyogenic granuloma. For that reason, there is the possibility they can simulate a nodular amelanotic melanoma. As a result, surgical excision and pathological examination of pyogenic granulomas are mandatory. 1-3,6,7
More recently, with the advent of new technologies such as confocal microscopy, advances in differential diagnosis have emerged. With this technique it is possible to evaluate the vascularization regarding dilatation, elongation, tortuosity, flow rate, and neovascularization. In addition, pagetoid cells and atypical melanocytes are not visualized in pyogenic granulomas. Studies are still preliminary, nevertheless there seems to be good histologic correlation. 9
Due to the diversity in clinical presentations of benign tumor lesions, such as pyogenic granuloma, imaging studies linking dermoscopy and confocal microscopy, especially in atypical cases, may be useful for defining the characteristics of these tumors and their histopathologic correlation.
1. Zaballos P, Llambrich Á, Cuéllar F, Puig S, Malvehy J. Dermoscopic findings in pyogenic granuloma. Br J Dermatol. 2006;154(6):1108-11.
2. Zaballos P, Rodero J, Serrano P, Cuellar F, Guionnet N, Vives JM. Pyogenic granuloma clinically and dermoscopically mimicking pigmented melanoma. Dermatol Online J. 2009;15(10):10.
3. Zaballos P, Carulla M, Ozdemir F, Zalaudek I, Bañuls J, Llambrich Á, et al. Dermoscopy of pyogenic granuloma: a morphological study. Br J Dermatol. 2010;163(6):1229-37.
4. Junck M, Huerter CJ, Sarma DP. Unknown: Rapidly growing hemorrhagic papule on the cheek of a 54-year-old man. Dermatol Online J. 2011;17(1):11.
5. Zaballos P, Salsench E, Puig S, Malvehy J. Dermoscopy of Pyogenic Granulomas. Arch Dermatol. 2007;143(6):824.
6. Zalaudek I, Kreusch J, Giacomel J, Ferrara G, Catricalà C, Argenziano G. How to diagnose non pigmented skin tumors: a review of vascular structures seen with dermoscopy. Part II: Nonmelanocytic skin tumors. J Am Acad Dermatol. 2010;63(3):377-86.
7. Zalaudek I, Argenziano G, Kerl H, Soyer HP, Hofmann-Wellenhof R. Amelanotic/Hypomelanotic Melanoma - Is Dermatoscopy Useful for Diagnosis?. J Dtsch Dermatol Ges. 2003;1(8):369-73.
8. Oiso N, Kawada A. Dermoscopy of pyogenic granuloma on the lip: the differing appearances of vascular structures with and without pressure. Eur J Dermatol. 2011;21(3):441.
9. Astner S, González S, Cuevas J, Röwert-Huber J, Sterry W, Stockfleth E, et al. Preliminary Evaluation of Benign Vascular Lesions Using in Vivo Reflectance Confocal Microscopy. Dermatol Surg. 2010;36(7):1099-1110.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}