


Eliandre Costa Palermo1
A careful study of the anatomy of the orbit is very important for dermatologists, even for those who do not perform major surgical procedures. This is due to the high complexity of the structures involved in the dermatological procedures performed in this region. A detailed knowledge of facial anatomy is what differentiates a qualified professional-whether in performing minimally invasive procedures (such as botulinum toxin and dermal fillings) or in conducting excisions of skin lesions-thereby avoiding complications and ensuring the best results, both aesthetically and correctively. The present review article focuses on the anatomy of the orbit and palpebral region and on the important structures related to the execution of dermatological procedures.
Keywords: EYELIDS, ANATOMY, SKIN.
To have a comprehensive knowledge of palpebral and orbital anatomy may sound excessive for dermatologists, given that they do not perform procedures in the deep levels of the ocular and orbital region. However, in light of the remarkable advances in procedures that encompass the orbital region, it has become important to recognize the crucial role of anatomical knowledge in ensuring better outcomes. Following are the main structures that make up the anatomy of the orbitopalpebral region:
Structures of the orbitopalpebral anatomy:
Bone margins
Innervation
Irrigation
Skin and subcutaneous tissue
Musculature
Orbital septum
Fat pads
The main function of the orbit is to give support and protection to the eyeball and its structures.
The volume of the orbital cavity of an adult is approximately 30cc. The border of the orbit measures about 40mm horizontally and 35mm vertically.1 Due to the fact it is a compartment with a fixed cavity that cannot be widened, bleeding in the region may increase eye pressure and lead to disastrous consequences.
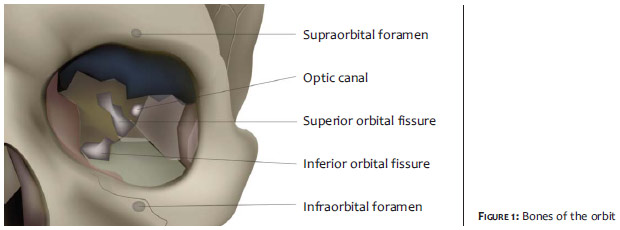
The orbit is composed of seven bones: ethmoid, sphenoid, zygomatic, frontal, maxillary, lacrimal, and palatine, which anastomose to form an osseous quadrilateral in the shape of a pyramid.1,2
The upper portion of the orbit is formed by the orbital process of the frontal bone, and the lesser wing of the sphenoid. At about 2.5 cm from the midline, a small notch in the bony edge can be felt through palpation: the supraorbital notch (supraorbital foramen in 25% of cases).3 It passes through the eyebrow arch on the midpupillary line about a third of the distance from the medial aspect of the orbital margin. The supraorbital artery and nerve pass through it. 2,3 Right above and parallel to the supraorbital margin is the superciliary arch, which sits just below the eyebrow and above the frontal sinus passage. This is more prominent in men and often absent in women, frequently contributing, in the latter, to the sagging of the eyebrows in their lateral portion.3 Subperiosteal filling with hyaluronic acid in this region can help to raise the lateral third of the eyebrow.
Medially, there is the frontal process of the maxillary, lacrimal, sphenoid bones, and a portion of the ethmoid. In the inferomedial border of this area there is a depression called the lacrimal fossa, which is formed by the maxillary and lacrimal bones and houses the nasolacrimal sac.1 At its anterior end there is the nasolacrimal groove, which is approximately 16 mm long, 4 to 9 mm wide and 2 mm deep. This groove becomes the nasolacrimal canal, which in turn flows into the nasal cavity. This fossa integrates with the nasolacrimal canal through the nasolacrimal duct.1,3 The lateral wall is formed by the greater and lesser wings of the sphenoid bone, the zygomatic bone, and the frontal portion.2
Inferiorly, there is the orbital plate of the maxilla, contiguous to the orbital plate of the zygomatic bone and the orbital plate of the palatine bones. At about 1cm from the inferior margin, on the slope of the maxilla, is the infraorbital foramen. This opening is directed from above and downwards and is located medially, approximately 2.5 cm from the midline, transmitting infraorbital nerves and vessels.3,4 (Figure 1)
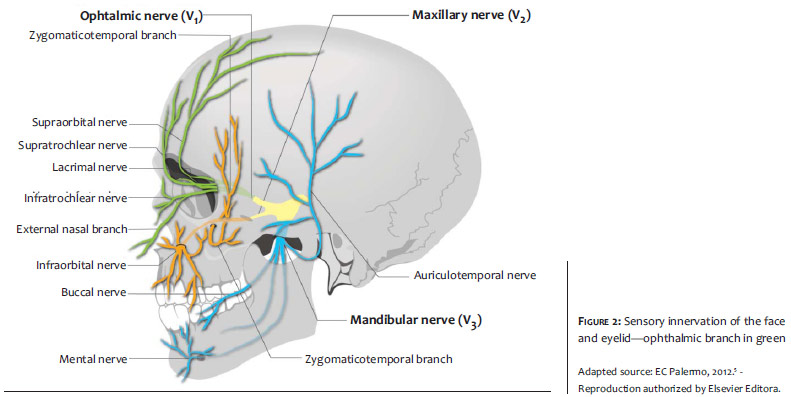
The sensory innervation of the upper and lower eyelid are respectively achieved by branches of the ophthalmic and maxillary nervesóboth are ramifications of the trigeminal nerve.5
The motor innervation is achieved with branches of the facial nerve (VII pair) that act on the orbicularis oculi, procerus, corrugator, and frontalis muscles. However, the structures responsible for the elevation of the upper eyelid are the levator palpebrae superioris (innervated by the oculomotor nerveóIII pair), and Müller muscle (innervated by the sympathetic nervous system). On the other hand, the frontalis muscle exerts only a small auxiliary lifting action on the upper eyelid. The orbicularis oculi muscle acts both in the upper as in the lower eyelids, promoting the occlusion of the palpebral fissure with the blinking and voluntary eyelid closure movements.5,6
For didactic reasons, the nerves of the eye and the orbit can be classified as the following:
Somatic motor: innervate the eye and the eyelid. The superior division of the oculomotor nerve (III) innervates the superior rectus and the levator palpebrae superioris muscle, while the inferior division innervates the inferior and medial rectus, and the inferior oblique muscles. The facial nerve (VII) innervates the facial expression muscles. Its frontal and zygomatic branches innervate the orbicularis occuli muscle, while the frontal branch innervates the muscles of the forehead.4,7
Sensory: trigeminal nerve or the 5 thcranial nerve (V) is the main sensory nerve of the face and of the anterior part of the scalp. Its main sensory branches are the ophthalmic, maxillary, and mandibular nerves, usually referred to as V1,V2, and V3, respectively.3,8 (Table 1)
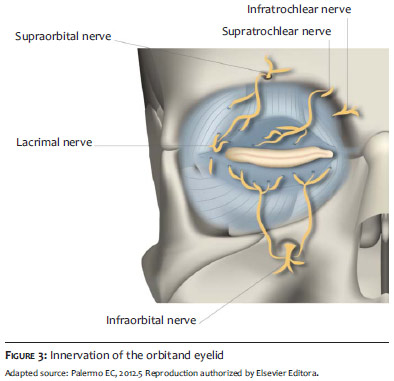
Ophthalmic branch (V1)ófrontal branch: supratrochlear and supraorbital nerves, responsible for sensory innervation of the upper eyelid, eyebrow, and forehead, and lacrimal gland (lateral orbital region). The nasociliary branch extends into long and short ciliary nerves innervating the eye and the medial region of the orbit;
Maxillary branch (V2)óinfraorbital nerve innervates the inferior eyelid.4,5 (Figures 2 and 3)
Visceral motor - autonomous - parasympathetic: oculomotor nerve (III), inferior branch for the ciliary ganglion located laterally to the posterior 1/3 of the optic nerve. The ciliary ganglion is a small ganglion located near the orbital apex, lateral to the ophthalmic artery and medial to the lateral rectus muscle, innervating the ciliary muscles and the pupil sphincter.4,9
The nerves present in the inner structure of the orbit are: oculomotor, trochlear, abducens, and the ophthalmic root of the trigeminal nerve.9 The ophthalmic nerve is one of the three branches of the trigeminal nerve and has itself three main branches in the orbit: the lacrimal nerve, the frontal nerve, and the nasociliary nerve.
The trochlear nerve enters the orbit through the superior orbital fissure, above the common tendon of the rectus muscles. It runs medially in the orbit, above the levator muscle of the upper eyelid to innervate the superior oblique muscle.9
The abducens nerve enters the orbit through the superior orbital fissure, within the Annulus of Zinn, innervating the lateral rectus muscle.2 (Table 1)
The orbital vascular irrigation system is actually very complex, with numerous interindividual variations. The blood supply of the eyelids derives primarily from the internal carotid artery via the ophthalmic artery, and secondarily from the external carotid artery, through the branches of the infraorbital, facial, and superficial temporal arteries.2,3
External and internal carotid arteries (ICA and ECA)
In general, the blood supply of the face derives primarily from the external carotid artery. Nevertheless, in the orbital regionówhere one of the points of anastomosis of the two systems occursóthe internal carotid dominates local irrigation. The internal carotid artery (ICA) provides a further arterial contribution to irrigation of the upper portion of the face and scalp.
The ICA emits numerous branches, however the present article will only cover the main branches and tributaries that irrigate the orbit. Collateral circulation does occur from the ICA to the middle meningeal artery and lacrimal and ethmoid anastomoses.10
The external carotid artery usually contributes only a small extension to the blood supply of the orbit, through the infraorbital artery and the orbital branch of the middle meningeal artery.8 The infraorbital branch is a secondary or indirect blood supply of the eyelids.3
The infraorbital arteryóa branch of the internal maxillary artery ñ passes through the inferior orbital fissure in the infraorbital groove and emits branches into the orbital fat and the orbital muscles that irrigate the inferior rectus and inferior oblique muscles.8 Laterally, the superficial temporal branch of the external carotid artery contributes to the superior and inferior palpebral arterial arch through the zygomatic-orbital and transverse facial arteries.3,8
Filling procedures in the ocular region, nasal dorsum, and glabella, with accidental intravascular injection in one of the distal branches of the ophthalmic artery, can lead to a rare, but very serious complication, with embolization of the central artery of the retina, resulting in blindness. This means that it is important to know in detail the orbital regionís irrigation and its ramifications.
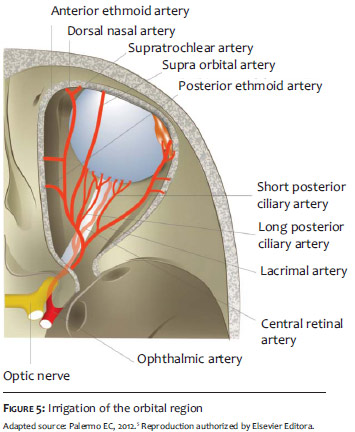
The ophthalmic artery, the first major branch of the internal carotid artery, is the main source of irrigation of the orbital region. It is responsible for the blood supply of the orbital structures, including nerves, muscles, lacrimal apparatus, the optical channel, part of the eyelid irrigation, part of the dorsum and superior region of the nose, and the frontal portion of the orbit.11,12 Several studies have shown that there is a very high rate of anatomical variability of the ophthalmic artery and its branches.11 Moreover, it is very important to bear in mind that, since the ophthalmic artery is one of the secondary axes that connect the external carotid system with the internal carotid system, some situations may predispose a retrograde flow of ocular irrigation, increasing the risk of complications, such as embolization.12,13
In 1887, Meyer carried out one of the first studies on the anatomical description of the ophthalmic artery, especially its branches and its variations. Notwithstanding the fact that his observations were based on only 20 cases, they were accepted as the norm by most anatomy books. Later on, studies have shown a wide variation regarding Meyerís initial descriptions.2
In most cases, it is a branch of the supra clinoid portion of the internal carotid artery. Approximately 8% of the ophthalmic arteries arise in the cavernous sinus, rather than in the subarachnoid space.11 The ophthalmic artery may also arise as duplicate arteries of similar size and rarely originate from the middle meningeal artery or the anterior communicating artery.8,11 The origin of the ophthalmic arteryis usually medial to the anterior clinoid process, below the optic nerve, where it runs parallel to the optic nerve, in the optic canal. The ophthalmic artery penetrates into the orbit through the optic canal, crosses from the lateral to the medial above the optic nerve in about 80% of cases and beneath that nerve in about 20% of cases.8-12 The artery runs forward horizontally, below the lower border of the superior oblique muscle, and divides into two terminal branches: the frontal and nasal dorsal.10
Central retinal artery: This is the firstóand one of the shortestóbranches of the ophthalmic artery. It arises near the orbital apex and enters the optic nerve about 1cm behind the eye, eventually occupying a central position within the optic nerve.8
Ciliary arteries: The long and short posterior ciliary arteries perforate the sclera to irrigate the ciliary body, the iris, and the choroid. Its branches penetrate bulbus oculi around the optic nerve.6 Two or three posterior ciliary arteries are sub-divided into about 15 short posterior ciliary arteries (that supply the optic nerve head and the choroid) and two long posterior ciliary arteries (that supply the ciliary body and iris).8
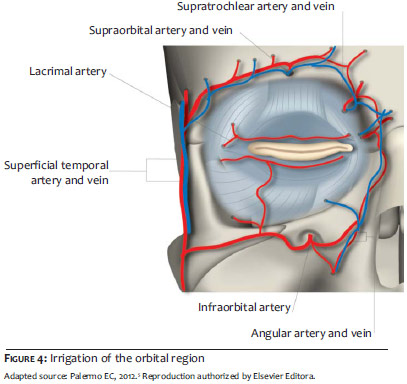
Lacrimal artery: This is one of the largest branches derived from the ophthalmic, running along the path of the lacrimal nerve. Its branches supply the lacrimal gland, the eyelids, the conjunctiva, and the superior and lateral rectus muscles. The lateral superior and inferior palpebral arteries are terminal branches of the lacrimal artery. They run from lateral to medial in the upper and lower eyelids, forming an anastomosis with the medial palpebral arteries and forming the superior and inferior arterial arch of the eyelids.8-12
The lacrimal artery also emits the zygomatic branches. One of the branches arises in the face through the zygomaticfacial foramen and through anastomoses with the transverse facial artery; the other branch passes through the zygomatictemporal foramen and irrigates the temporal fossa, where it forms an anastomosis with the deep temporal arteries.10
Medial superior and inferior palpebral arteries: The ophthalmic artery passes between the oblique superior and medial rectus muscles toward the orbit, dividing into superior medial and inferior palpebral arteries, forming a superior and an inferior irrigation arches between the orbicularis muscle of eyes and the tarsus.10
The marginal arch lies opposite the tarsus at 3mm from the palpebral margin. The peripheral arch is located between the aponeurosis of the levator palpebrae muscle and the Müllerís muscle, above the superior border of the tarsus in the upper eyelid. In the lower eyelid, its position may vary. 3,14
The superior palpebral artery passes around the medial aspect of the nasal fat into the pretarsal space, where it divides into a lesser marginal arch and a greater peripheral arch that forms an anastomosis with palpebral lateral branches of the lacrimal arteries.3 The inferior palpebral artery passes through the medial canthal tendon, superior to the fat pad of the lower eyelid, to reach the pretarsal space, where the peripheral and marginal arterial arch are also formed.3 (Figures 4 and 5)
Posterior and anterior ethmoid arteries (PEA and AEA): The PEA passes along the medial wall, between the superior oblique muscle and the medial rectus muscle, crossing the posterior ethmoid canal. In the orbit, this vessel can irrigate the superior oblique muscle, the superior and medium rectus muscles, and the superior eyelid levator muscle. The AEA, in turn, runs along the nasociliary nerve and exits the orbit through the anterior ethmoidal foramen. In the orbit, it irrigates the superior oblique muscle, the anterior and middle ethmoid portion, the frontal sinus, the lateral nasal wall, and the nasal septum.10
The cutaneous branches of the ophthalmic artery are:
Supraorbital artery: This artery route supwards medially to the superior rectus and the superior eyelid levator muscles, irrigating them and following the path along the supraorbital nerve. As the artery passes through the supraorbital foramen, it divides into a superficial and a deep branch, which supply the integument, muscles, and pericranial tissues of the eyebrows and forehead. It forms an anastomosis with the supratrochlear artery and the frontal branch of the superficial temporal artery, and with thesupraorbital artery of the opposite side.
Supratrochlear artery10: One of the terminal branches of the ophthalmic artery, the supratrochlear artery or frontal artery, leaves the orbit in its medial angle above the trochlea with the supratrochlear nerve, going upward into the forehead, and irrigating the lower forehead and scalp. The supratrochlear artery forms an anastomosis with the supraorbital artery and contralateral vessels. 10,12
Dorsal nasal artery: This artery emerges from the orbit above the medial palpebral ligament, irrigates the root and dorsum of the nose, crosses the nasal root and extends into two branches. One of these anastomosizes with the contralateral artery and with the lateral nasal artery. The other anastomosizes with the angular artery, which is the terminal branch of the facial artery.10,12
Below are the different points of anastomosis in the orbital region:
Anastomosis between the ECAand ICA systems
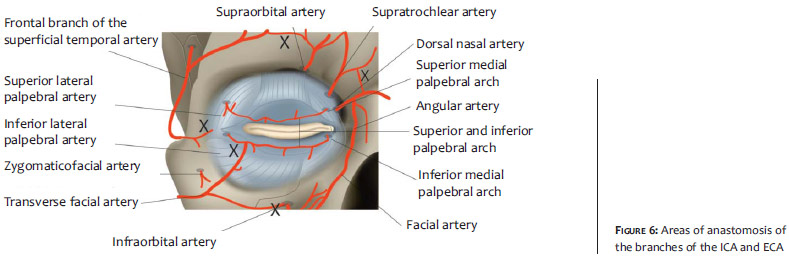
The periorbital region has a huge network of arterial anastomoses, and numerous anatomical variations that make it impossible to predict with certainty the exact locations of their occurrence. Nevertheless, with prior knowledge of the location of the main connection points between the systems, it is possible to minimize the risks of applications in those locationsóusing cannulas to perform fillings, for instance.
The orbital region has some points of anastomosis of the external carotid system with the internal carotid system. One of the most important is the anastomosis of the dorsal nasal artery with the angular artery. The facial artery, a branch of the external carotid artery, leads into the angular artery after superficially crossing the medial canthal tendon, where it anastomosizes with the dorsal nasal branch of the ophthalmic artery, which in turn is a branch of the internal carotid artery. One of its branches joins the angular artery at the root of the nose, and the other runs downward, anastomosizing with the external nasal artery, which is a branch of the infraorbital artery. 10,15
Another point is the anastomosis of the superficial temporal artery with branches of the supraorbital artery. From the external carotid artery, there is the superficial temporal artery, which anastomosizes medially with branches of the supraorbital artery, which in turn is a branch of the ophthalmic artery that derives from the internal carotid artery. 3,10
The zygomatic artery that derives from the lacrimal artery anastomosizes with the transverse facial artery, a branch of the superficial temporal artery. 10
The lacrimal artery gives rise to a recurrent meningeal branch that anastomosizes with the middle meningeal artery, forming another communication axis between the internal and external carotid arteries.10,13
The lateral and medial palpebral arteries anastomosize with each other, forming two sets: the marginal and peripheral arch. The superior medial palpebral artery anastomosizes with the zygomatic-orbital branch of the temporal artery in the lateral angle of the orbit. That artery also anastomosizes with the superior portion of the two lateral branches of the lacrimal artery.13 (Figure 6)
The venous system of the orbital regionis highly variable and complex. Unlike in other sites of the body, there is no correspondence between arteries and veins, except for the superior ophthalmic vein, which has correspondence with the ophthalmic artery.12
Venous drainage of the orbit is performed by the inferior and superior ophthalmic veins, which are located within the connective septum of the orbit. The superior ophthalmic vein is formed near the root of the nose with the union of angular, supratrochlear, and supraorbital veins. Divided into three sections, the vein runs along the path of the ophthalmic artery, passes through the superior orbital fissure and ends in the cavernous sinus. The first section passes along the medial border of the superior rectus muscle, the second section passes near the superior rectus muscle and the third section passes posteriorly along the lateral border of the superior rectus muscle to enter the superficial orbital fissure, outside the annulus of Zinn, draining into the cavernous sinus.8 The inferior ophthalmic vein is more variable, and usually is formed anteriorly as a plexus in the inferomedial orbital fat. The four vorticose veins pierce the sclera obliquely and end in the ophthalmic veins. The central retinal vein is identified contiguous to the central retinal artery, often entering the cavernous sinus directly, and may join one of the ophthalmic veins.8,13
The drainage of the eyelids is carried out by the pre-tarsal and post-tarsal veins. The pre-tarsal veins are more superficial and connect latero-superiorly with the superficial temporal and lacrimal veins, and medially with the angular vein. The post-tarsal section connects the orbital veins with the deep branches of the anterior facial vein and the pterygoid plexus. The main venous drainage of the eyelids flows into the superficial temporal, angular, and facial veins, connecting superiorly with the supraorbital frontal system, and with the facial vein inferiorly. As in the arterial system, there are venous arch that drain into the main venous drainage systems.3
Lymphatic drainage
The lymphatic vessels of the eyelids have systems similar to those of the veins, being divided into pre-tarsal and post-tar-sal. The pre-tarsal vessels provide lymphatic drainage of the eyelidís skin and of the orbicularis oculi muscle. The post-tarsal deep plexus provides lymphatic drainage of the tarsal plates, glands and other structures of the palpebral margins, including the conjunctiva and lacrimal glands.3 The palpebral lymphatic vessels drain two main areas. The lateral lymphatic drainage group provides drainage of the lateral aspect of both eyelids, as well as of the deep vessels that drain the conjunctiva and lacrimal glands of the upper eyelids. They drain into the superficial and deep parotid lymph nodes (pre-auricular). The medial aspects of both eyelids and lacrimal sac run parallel to the lacrimal vein into the submandibular lymph nodes.3
The eyelids are specialized structures with unique anatomical components. The skin of the eyelid is the thinneston the human body, with a thickness of 700º to 800º. 6 The stratigraphiesof the eyelids can differ according to the section assessed, with 4 layers in the tarsal portion and 7 layers in the tarsal region, above the orbital septum. In the tarsal portion there are: (1) skin and subcutaneous tissue, (2) orbicularis oculi muscle, (3) tarsus, and (4) and conjunctiva. In the proximal portion there are: (1) skin and subcutaneous tissue, (2) orbicularis oculi muscle, (3) orbital septum, (4) post-septal or orbital fat, (5) aponeurosis of the levator muscleof the superior eyelid, (6) Müller muscle, and (7) conjunctiva. 3
The upper eyelid extends superiorly to the eyebrow, which separates it from the forehead. The lower eyelid extends below the inferior orbital border, forming folds where the eyelidís loose conjunctive tissue is juxtaposed to the thicker tissue of the cheek. 5
The palpebral skin is still divided into two parts: the orbital portion (between the tarsal portion and the orbital border), and the tarsal portion (between the free border and the orbito-palpebral sulcus). The subcutaneous tissue is composed of loose conjunctive tissue, which is very scarce in the skin of the eyelid. The tarsal portion is very thin and vascularized, with an absence of subcutaneous tissue. The transition from that portion of the tarsal skin to the orbital portion is clinically evident in thickness and color, being delimited by the superiorpalpebralsulcus. The eyelids are the protective covering of the ocular globe. The palpebral borders enter in contact during the closure and the blinking movement of the eyelids. The eyelids help in creating and maintaining the lacrimal film, the mucus and the oil that are necessary for the corneaís survival.5
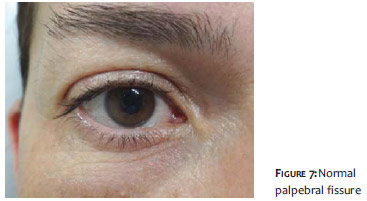
With an elliptical shape, they measure between 28mm and 30mm in width, and from 7mm to 12mm in height in men (from 8mm to 12mm in women). The space between the superior and inferior eyelids is called palpebral fissure. When opened, the superior eyelid should usually cover about 1mm to 2mm of the iris, with the inferior edge of the lower eyelid slightly brushing the inferior limbus.16 (Figure 7)
In the case of a decrease of that distance due to the lowering of the upper eyelid, palpebral ptosis is configured. The socalled scleral show occurs when the palpebral fissure is enlarged due to malocclusion of the lower eyelid.5,16
Although similar, the upper and lower eyelids have different characteristics.
The lower eyelid has three sulci: inferior palpebral, malar, and nasojugal. The inferior palpebral sulcus begins at the medial canthus, bends down and passes over the inferior border of the tarsus, ending in the lateral canthus. The nasojugal sulcus begins below the medial canthus, and runs downward and laterally at an angle of 45º. The malar sulcus begins laterally at the malar prominence and curves medially and downwardly until it intersects the nasojugal sulcus. The nasojugal and malar sulcus attach to the periosteum through a fascia.3,17
The upper eyelid has an orbito-palpebral sulcus or superior palpebral sulcus. It divides the eyelid into two parts: the palpebral and tarsal portion below and the orbital portion above. The sulcus is formed by the insertion of the levator muscleís aponeurosis in the upper eyelid, in the orbicularis septum. The sulcus begins medially at 3mm from the ciliary border (measuring, on average, from 6mm to 8mm in its central portion in women and from 7mm to 10mm in men) and ends in the lateral portion, at 4 to 5mm from the ciliary border.5,17 (Figure 8)
In people of East Asian heritage, it is located lower, at about 2 to 4mm from the tarsus. That palpebral sulcus is very important for it is used as reference in the marking and removal of skin in the superior blepharoplasty. The blepharoplasty technique with Westernization consists of building this sulcusówhich is absent in this caseócarrying out a plication in the muscle. 3,14
It is important to bear in mind these measurements as well as some pre-existing conditions before carrying out procedures that can lead to changes in the ocular closure. Below are some of the common problems related to eyelids:
Palpebral ptosis: Decrease of the palpebral fissure due to lowering of the upper eyelid.
Apparent sclera: Occurs when the palpebral fissure is increased due to malocclusion of the lower eyelid.
Lagophthalmos: Excessive exposure of the eye, with inability to close it.
Dermatochalasis: Excess of skin in the upper, lower, or both eyelids, associated with the aging of the eyelid and eyebrow.
The palpebral borders are 2mm thick and are the junction between the skin and the mucous membraneof the eyelidsóthe conjunctiva. They are located in the gray line, near each palpebral borderís posterior border, and can be readily identified through a change in the color of the skin. The so-called gray line is the line of union between the skin and orbicularis muscle (anteriorly) and between the tarsus and the conjunctiva (posteriorly). The gray line is also an anatomical structure that identifies the junction of the eyelidsí anterior and posterior lamellas.3,17 The caruncle and the semilunar fold are located in the medial region, where there is an elevation called lacrimal papilla, whose central orifice presents the lacrimal punctum. The Meibomian glandsí orifices are located behind the gray line.17 There are approximately 40 Meibomian glands in the upper eyelid and 20 to 30 in the lower eyelid.3
The eyelashes form two or three layers anteriorly to the gray line, being more numerous and thick in the upper eyelid. There are approximately 100 to 150 eyelashes in the upper eyelid and half that number in the lower eyelid.
Orbicularis oculi muscle
The second palpebral layer is the orbicularis oculi muscle, a striated muscle formed by the palpebral and orbital portions. The orbital portion has voluntary contraction, while the palpebral portion can have voluntary and involuntary movements. Innervation of the upper portion of the orbit occurs throughthe temporal branch of the facial nerve, while in the lower portion it occurs through the zygomatic branch of the facial nerve. The orbital portion covers the orbital border and its fibers are intermingled medially with the procerus muscle and superiorly with the frontal muscle. The central portion of the orbicularis oculi muscle covers the eyelid and is referred to as the palpebral portion. 3,14
The palpebral portion of the orbicularis muscle is divided into two parts:
 Pre-tarsal portion:It is located over the tarsal plate of the orbicularis muscleand is tightly adhered to the tarsus. It begins in the lateral canthus and inserts in the medial canthus. Its superficial portion forms the anterior part of the medial canthal tendon. Its deep portion inserts into the bone of the posterior lacrimal crest, forming the posterior medial canthal tendon. When contracted, the eyelid closes, bringing the lacrimal punctum close to the lacrimal sac.7,17
Pre-tarsal portion:It is located over the tarsal plate of the orbicularis muscleand is tightly adhered to the tarsus. It begins in the lateral canthus and inserts in the medial canthus. Its superficial portion forms the anterior part of the medial canthal tendon. Its deep portion inserts into the bone of the posterior lacrimal crest, forming the posterior medial canthal tendon. When contracted, the eyelid closes, bringing the lacrimal punctum close to the lacrimal sac.7,17
Pre-septal portion:It is loosely attached to skin and covers the orbital septum of theupper and lower eyelids, with its fibers bundling laterally to form the lateral palpebral raphe. The preseptal portion inserts in the lacrimal fascia, on the lateral part of the lacrimal sac, and when contracted, produces a tear in the lacrimal sac. When the muscles relax, the lacrimal fascia returns to its normal position and the tear drains directly into the nasolacrimal duct.14,17
The superior and inferior medial canthal tendons originate in the medial aspect of the tarsal plates, which coincides with the location of the papill and the lacrimal punctum. The superior and inferior medial canthal tendons, as well as the common medial canthal tendon, can be seen through thin eyelids as white, firm structures that extend from the medial canthus up to the medial aspect of the orbit.3
The lacrimal canaliculus lies deep to the common medial canthal tendon, and is therefore protected from traumas in that locationóif the tendon is not sectioned. The angular artery and vein cross the tendon at its medial aspect and anastomosize with branches of the ophthalmic vessels above the superior border of the tendon.3,17
Extraocular muscles
The main extraocular muscles are the superior eyelid levator muscle, the four rectus muscles (superior, inferior, lateral, and medial) and the two oblique muscles (superior and inferior).5
Superior eyelid retractor muscle
The superior eyelid retractor muscles consist of the frontal muscles, superior eyelid levator muscle, superior tarsal muscle (or muscle of Müller), and also the Whitnall ligament. The superior eyelid levator muscle originates from the lesser wing of the sphenoid bone and, later on, dividing into aponeurosis and the superior tarsal muscle. The aponeurosis inserts and overlaps with the fibers of the orbicularis muscle to form the palpebral sulcus.5
Superior eyelid levator muscle and muscle of Müller
The fourth layer of the upper eyelid is formed by the superior eyelid levator muscle and aponeurosis. It is innervated by the oculomotor nerve (3rd cranial pair). When it shifts into a diagonal-vertical direction, it divides into anterior aponeurosis and posterior tarsal muscle of Müller. It is responsible for lifting the upper eyelid and therefore opening the eye. The aponeurosis merges with the superior transverse ligament in the superior orbit, which acts as a restraint ligament that provides additional support for the aponeurosis.3 The aponeurosis merges with the orbital septum and then inserts in the anterior surface of the tarsus. It is firmly attached to the orbicularis oculi muscle and to the skin by fibrous bands. The superior borderof this insertion is marked by the lower crease of the upper eyelid (superior eyelid sulcus). During blepharoplasty, when operating in the postseptal space, it is necessary to take care in order to avoid trauma of the aponeurosis and the resulting ptosis.
The Müller muscle (controlled by the sympathetic nervous system), inserts in the superior margin of the tarsal plate. It contributes to the tonic elevation of the eyelid by2 to 3mm.17 The innervation of the superior tarsal muscle (Müller) is achieved by the sympathetic nervous system.14
Lower eyelid retractor muscles
The lower eyelid retractor muscles are composed of a layer of fibrous tissue originating from the sheath of the inferior rectus muscle that attaches to the inferior border of the tarsus. In both morphology and function this tissue resembles the aponeurosis of the upper eyelid levator muscle. It extends along the inferior rectus muscle, intertwines with the inferior suspensory ligament (of Lockwood) of the bulbus oculi and runs toward the inferior border of the tarsus, accompanied by fibers of the inferior tarsal muscle. The retractor muscles are responsible for lowering the lower eyelid when looking downward. The same similarity exists between the lower tarsal and upper tarsal muscles. The tarsal plate is a dense conjunctive tissue that provides structure to the eyelid, stabilizing the palpebral border. As the superior tarsal plate measures approximately 11mm, it can be used as a donor source for tarsal-conjunctival graft. On the other hand, the inferior tarsal plate, measuring about 4mm, does not offer that possibility. The medial canthal tendon is formed by the insertion of pre-tarsal and pre-septal muscles. Its superficial portion inserts in the anterior lacrimal crest, while its deep portion inserts in the posterior lacrimal crest. The lateral canal tendon is a tendon that gives rise to the pre-tarsal muscles.3,5
The third layer of the eyelids in their upper portion is the orbital septum. It is a fibrous conjunctive tissue membrane that separates the orbital fat pads and deep orbital structures from the eyelid itself. It originates from the orbital marginal insertions of the thick fibrous band (arcus marginalis), which is formed by the junction of the orbital and periorbital periosteum with the insertion of the deep layer of the aponeurotic galea.3 The septum merges laterally with the lateral canthal tendon and medially with the aponeurosis of the upper eyelid levator muscle. In the upper eyelid, the orbicularis septum inserts in the levator muscle, however, in the lower eyelid, the septum and the aponeurosis of the retractor muscle insert in the inferior border of the tarsus and of the inferior fornix.14 Behind the septum are the fat pads. In blepharoplasty it is necessary to make small incisions in this septum in order to remove the fat pads. With aging, both the septum and the orbicularis muscle and skin become looser and thinner, causing orbital fat prolapse, making it prominent. Blepharoplasty is usually performed to correct that defect, however filler injections in the nasojugal sulcus region can alleviate the problem and delay the necessity of surgery.
Fat pads
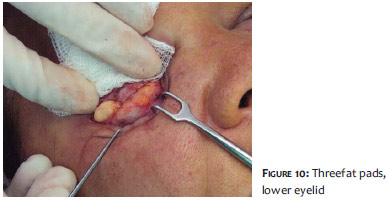
The palpebral fat pads are located behind the orbital septum and in front of the palpebral retractor muscles. There are three compartments in the lower eyelid: nasal, central, and lateral. The nasal fat pads are more whitish in appearance than the others. These fat pads are surrounded by a thin fibrous fascia, which separates them intodistinct compartments. There are two compartments in the upper eyelid: the pre-aponeurotic fat pad and the nasal fat pad. The lacrimal gland lies laterally, and may be mistaken with the adipose body. Therefore, one should be careful not to inadvertently injure the gland during surgical procedures.3-14
The large superior and inferior medial palpebral vessels run on the surface of the respective nasal fat pads and can be carefully dissected or clamped when the fat pad is excised during blepharoplasty. Although the vessels of pre-septal and muscle areas are well supported by connective tissue and muscle, the orbital vessels are virtually unsupported. As a result, despite the fact that they can withstand some tension, orbital vessels can be easily traumatized and even suffer severe strain during blepharoplasty.14 Bleeding in these vessels can lead to increased intraocular pressure and even blindness. The inferior oblique muscle is also vulnerable to trauma during suchprocedures, during the removal of the inferior medial fat pad. 17 (Figs. 9 and 10)
Tarsal blade
Tarsus are structural elements of the eyelids composed of dense fibrous tissue, and measuring approximately 29mm in width, 10-12mm in height at its medial point, and 1mm in thickness. The inferior tarsus has the same width and thickness, but is 5-6mm high. The tarsus begins medially in the lacrimal punctum, extending up to the lateral commissures. The Meibomian sebaceous glands are embedded vertically in the tarsal plate and extend toward their marginal aspects. Thirty to 40 glands are present in the upper eyelids, and 20 to 30 are present in the lower eyelid.3
The glabella and nasal root region is a location of major risk in the face when performing cutaneous filler injections. Despite being highly vascularized, this region differs from other areas of the face for presenting two separate events. Although it contains a rich vascular network, many of the vessels in the region are superficial and some have terminal branches. This leads to a higher risk of necrosisódue to both ascending embolization in the forehead and ischemia by external compression.
The supraorbital arteryówhich leaves the orbit through the supraorbital foramenóand the supratrochlear arteryówhich surfaces through the superior and medial portion of the orbitóemerge in the glabella anteriorly to the corrugator supercilii muscle, and posteriorly to the orbicularis oculi muscle. Subsequently, both arteries cover a short path towards the frontal muscle and become superficial.
Another important event concerns the anastomoses network present in the glabellar region and across the periorbital regionóespecially in the medial portionóthat ultimately increases the risk of embolism of the central retinal artery. Cutaneous filling applications in this region might reach vessels that have anastomosis with the internal carotid system, reaching the ophthalmic artery in retrograde and then to the central retinal artery.
The control of the flow of the ophthalmic artery depends on the autonomic nervous system. In cases of stimulus of the cervical sympathetic receptors, the flow in the ophthalmic artery is reduced, while in sympathectomy an increase in the flow occurs. In contrast, the central retinal artery is a terminal vessel that has a characteristic mechanism of self-regulation and is not subject to the action of the autonomic nervous system. Thus, alterations in the flow of the ophthalmic artery directly affect the central retinal artery. The anastomoses between the systems help to regulate and maintain the blood support to the central nervous system.13 Nevertheless, in situations where the flow is reduced, the secondary vascular axis is activated. In the presence of internal carotid artery stenosis, for example, reversal of the flow occurs and, hence, the patient in this situation, even if asymptomatic, has a greater chance of an embolization that might reach the central retinal artery.13
Risks of cutaneous filling techniques in the orbital region.
The most common complications regarding cutaneous fillings are related to circulatory issues. The more frequently affected sites, and those of greater risk of ischemia or embolization in the orbito-palpebral region concerning blindness are:
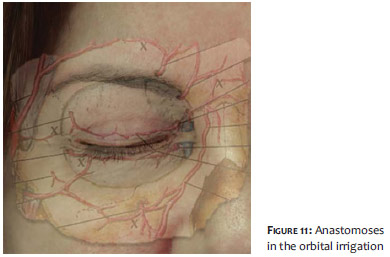
Nasojugal sulcus: as seen earlier, blood circulationin the eyelid happens through an anastomosis of the branches of the ophthalmic artery, laterally through the lacrimal artery (originating from the lateral palpebral branches) and medially through the branches of the medial palpebral artery (originating from the upper and lower eyelid artery). The medial and lateral palpebral arteries anastomosize with each other, forming two sets of marginal and peripheral arches. (Figure 11) The marginal arch lies opposite to the tarsus at 3mm from the palpebral margin. The peripheral arch lies between the aponeurosis of the eyelid levator muscle and the Müller muscle, above the superior border of the tarsus, in the upper eyelid. In the lower eyelid, its position may vary. This inferior and medial region is therefore one of the areas of risk regarding embolization during application of cutaneous filling in the nasojugal sulcus.
Glabella: The supraorbital and the supratrochlear arteries are superficial in this region. Moreover, vascularization in the glabellar region is poor because it is predominantly a terminal circulation. Thus, obstruction of these small arteries can easily occur with injections of materials used for both external and internal filling. This superficial pathway is the most vulnerable point of these arteries, and is where there is a high risk of intravascular injection (Figure 12).
Medial portion of the orbit: In this specific region of the orbit, more precisely contiguous with the final and superior part of the nasojugal sulcus and the lateral portion of the nasal root, passes the angular arteryóthe final branch of the facial artery (a branch of the external carotid artery), which anastomosizes with the dorsal nasal artery (the final branch of the ophthalmic artery). At this point, in patients who have thin skin, it is possible to visualize the angular vein, which runs slightly more centrally than the angular artery. The angular artery and vein cross the medial canthal tendon and anastomosize with branches of the ophthalmic vessels above the superior border of the tendon. These sites contain one of the carotid systemís anastomoses, a fact that also enables clots to access the central artery of the retina in retrograde.
Since the palpebral artery is a branch of the ophthalmic artery, in the case of intravascular injection withthe release of clots of the filling product, there is a chance for those clots to move and reach the central retinal artery in retrograde, causing counter flow in the circulation of the ophthalmic artery.
Some studies demonstrate that this secondary vascular axis of anastomosis between the ICA and ECA (that reverse the flow of the ophthalmic artery) is activated when there is hemodynamically significant stenosis of the ICA, as evidenced by Doppler records of retrograde flow in the ophthalmic arteries. 13
As a result, this calls into question whether some patients, even asymptomatic ones, might have a retrograde flow permanently activated and thus have an increased risk of complications related to cutaneous fillings in this region, affecting the central retinal artery.
Therefore, it is of paramount importance to be aware of the early signs of embolic or ischemic complications, including pain, local whitening, followed by hyperemia or blueness, visual blurring, and loss of vision.
As previously seen, the thickness of the palpebral skin and its correlation with the orbicularis muscle and the quasiabsence of subcutaneous tissue, also make the site risky for less seriousóyet undesirableócomplications, such as the implant being visibly apparent in the palpebral region.
In order to avoid this problem, it is important to assess the site thoroughly before application and, where possible, work at deep and intermediate planes, preferably with the use of cannulas or micro-cannulas.
Botulinum toxin risks in the orbital region
Rare complications, however related to ocular anatomy, are diplopia and strabismus after botulinum toxin injection, with the probable cause being the toxinís affect on the extrinsic muscles of the eye, such as the inferior oblique and the lateral rectus.18
The paresis of the inferior oblique muscle is caused by the migration of the toxin applied to the glabella and nasal region to the muscle, since the insertion of the inferior oblique muscle occurs in a small depression just behind the orbital boder lateral to the lacrimal duct. As for the paresis of the lateral rectus muscle, the explanation would be the migration of the toxin applied in periorbital wrinkles (crow's feet), due to the anatomical proximity of that muscle to the region treated with the toxin.
The feared post-botulinum toxin ptosis, in turn, relates to the toxinís affecton the upper eyelid levator muscle, while the fall of the brow or pseudo ptosis relates to its action in the frontal muscle.
Due to the great local vascularization of the eyelids, there is a high risk of bleeding and echymosis. Furthermore, the lymphatic drainage system is very fragile, leading to the very common emergence of edema in this region after the application of cutaneous fillers and botulinum toxin. In the case of toxin applied to the glabella, some patients frequently complain of ìswellingî in the eyes, especially in the morning, with edema in the upper eyelid that may be related to excessive relaxation of the superficial musculature that aids in local drainage. The same can occur in cases where cutaneous fillers are applied in the orbital region, due to the hydrophilic nature of the products, with edema that can be intermittent and prolonged, worsening after exposure to heat. In general, this problem resolves spontaneously, however it can be aided by manual drainage. In the specific case of cutaneous filling, the recommendation is to evaluate whether only edema occurred or if there was indeed superficialization of the filleróa situation where it can then be treated with applications of hyaluronidase.
Care in anesthesia and orbital surgery
Regarding anesthesia in dermatological procedures, given that multiple cutaneous sensory nerves assist in the innervation of the orbit and eyelid, local infiltration or nerve blocks are good methods for anesthesia of the region. Local infiltration must be initiated by the lateral canthus, in the subdermal plane, with thin needles in order to avoid hematoma. Since the skin above the tarsus is loose, the needle can be advanced smoothly in the medial direction, as the injection of anesthetic elevates the epidermis and separates it from the dermis and from the orbicularis muscle.
If the surgery comes in contact with the tarsus or a chalazion forceps is used, the cornea must first be anesthetized with a topical ophthalmic solution. The patient should be warned and the surgical team must be constantly aware of the fact that there is no corneal reflex, resulting therefore in the possibility of a significant lesion of the eye during the effective period of the local anesthesia. In the case of nerve blocks, the indication is to follow the midpupillary line as a reference, for it is the exit site of the supra and infraorbital nerves. Alternatively, intraoral nerve block can be carried out in the case of the lower eyelid. There is a risk of intravascular injection, however cases of serious complications are rare.
The lower eyelid has less redundant skin and is less tolerant to excessive tissue removal than the upper eyelid.Vertically oriented defects may result in ectropion if the tarsus is not well evaluated prior to the procedure. If located in the medial region of the palpebral margin, minor lesions can heal well by secondary intention, avoiding retraction of the tarsus. It is always crucial to evaluate in advance the local laxity.
The potential for development of ectropion can be estimated by pulling the defect with skin hooks or toothed forcepswhile instructing the patient to look up with his or her mouth open. This maneuver exerts maximum tension on the lower eyelid. If an impending ectropion is evident, an alternative such as a skin graft or flap should be considered. Pre-operative laxity of the lower eyelid can be estimated through the ìsnaptestî, in which a seated patient has their lower eyelid seized and moved away from the eyeball.
In the same way, the skin laxity of the proximal tarsal eyelid allows the (generally important) accumulation of fluid and edema, so blood or pus may also accumulate. Patients should be warned about the possibility of significant edema or echymosis after eyelid, forehead, or scalp surgery.
There are several studies and publications demonstrating serious complications in the use of cutaneous fillers in the orbital region, glabella, nasal dorsum, and ala and even in the nasogenian sulcus and lips. Precisely because of the vast network of anastomoses between the superficial and deep carotid system, there is a risk of embolization even during application of products in seemingly safe areas.
The existence of this vascular complex helps to maintain an adequate blood flow to the central nervous system in case of any failure in the circulatory supply. Notwithstanding, this same system may be the cause of serious complications such as clots reaching the central retinal artery, leading to blindness, large edema, and ecchymosis.
The orbital region has a challenging and delicate anatomy, where even procedures that seemingly do not present risks (such as dermatological procedures), may suffer complications. Many cases of blindness and necrosis after filling applications are unfortunately irreversible. Therefore, only prevention and knowledge of risk areas can provide good results and low complication rates.
1. Thiagarajan B. Anatomy of Orbit: Otolaryngologist's perspective. ENT SCHOLAR. 2013;1:1-33.
2. Petruzzelli GJ, Hampson CM, Meyers AD, Kokoska MS, Kellman RM, Slack CL, et al. Orbit Anatomy.[Internet]. New York: Medscape; 2011 [cited 2013 Sept 9]. Available from: http://emedicine.medscape.com/article/835021-overview
3. Salasche SJ, Bernstein G, Senkarik M. Surgical anatomy of the skin. Appleton& Lange, 1988. p. 183-197.
4. Smith RL. Anatomia da órbita: introdução. [Internet]. São Paulo: Unifesp. [citado 9 Set 2013]. Disponível em: www.oftalmo.epm.br/aluno/disciplina_eletiva/anatomia_olho/anatomia_olho.pdf.
5. Palermo EC. Rejuvenescimento da região palpebral. In: Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. p. 455-87.
6. Palermo EC. Cirurgia da região periorbitária. In: LupiO, Belo J, Cunha PR, orgs. Rotinas de diagnóstico e tratamento da Sociedade Brasileira de Dermatologia. 2º ed. São Paulo: AC Farmacêutica, 2010. p. 69-77
7. Patel B, Taylor SF, Gupta R, Kokoska MS, Talavera F, LaFerriere KA, et al. Eyelid Anatomy. [Internet]. New York: Medscape; 2013 [cited 2013 Sept 9]. Available from: http://emedicine.medscape.com/article/834932-overview
8. René C. Update on orbital anatomy. Eye (Lond). 2006;20(10):1119-29. doi:10.1038/sj.eye.6702376
9. Ferreira RGF, dos Santos MLB. Estudo morfológico e neurofuncional da cavidade orbital. Acta Sci Med. 2012 [citado 9 Set 2013];5(1):2-8. Disponível em: http://www.actascientiaemedica.com/Artigos/PDF/1-2012/Ciencias_Basicas_Ferreira_et_al.pdf
10. Duong HVQ, Copeland RA Jr, Wilson JL, Windle ML, Duffy MT, Garzia R, et al. Orbit Arterial Supply. [Internet]. New York: Medscape; 2013 [cited 2013 Sept 9]. Available from: http://emedicine.medscape.com/article/1189696
11. Martins C, Costa e Silva IE, Campero A, Yasuda A, Aguiar LR, Tatagiba M, et al. Microsurgical anatomy of the orbit: the rule of seven. Anat Res Int. 2011;2011:458727.
12. Hayreh SS. Orbital vascular anatomy. Eye (Lond). 2006 [cited 2013 Sept 9];20(10):1130-44. Available from: http://www.nature.com/eye/journal/v20/n10/full/6702377a.html
13. Diniz ALD, Moron AF, Santos MC. Sass N. Dopplervelocimetria colorida dos vasos orbitais: técnica de exame e anatomia vascular normal. Radiol Bras 2004;37(4):287-290.
14. Kaminer MS, Dover JS, Arndt kA. Atlas of Cosmetic Surgery. Saunders, 2002,351-384.
15. Tamura B. Anatomia da face aplicada aos preenchedores e à toxina botulínica - Parte II. Surg Cosmet Dermatol. 2010;2(4):291-303.
16. Schellini SA, PretiRC,Yamamoto RK, Padovani CR, Padovan CRP. Dimensões palpebrais antes e após blefaroplastia superior - Avaliação quantitativa. Arq Bras Oftalmol. 2005;68(1):85-8.
17. Pitangy I, Sbrissa RA. Atlas de cirurgia palpebral.Rio de Janeiro:ColinaLivr. Ed.; 1994. p.21-252.
18. Lacordia MHFA, Januario FSM, Pereira JCC. Estrabismo após toxina botulínica para fins estéticos. Rev Bras Oftalmol. 2011;70(3):179-81.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}