


Geraldo Magela Magalhães1; Maria de Fátima Melo Borges2; Amanda Gomes Dell'Horto3; Denise de Borba Carvalho3; Marcela Mattos Simões Mendonça3; Marcos Alvarenga de Souza Júnior3
Introduction: For some patients, pain during the injection of botulinum toxin can represent a limitation for performing the procedure. There are doubts about whether the use of topical anesthetic decreases pain or interferes with the treatment's efficacy and duration of effect. Objectives: To study the effect of 4% lidocaine cream in controlling pain during BoNT-A - Speywood Unit botulinum toxin application, comparing it to the vehicle. In addition, the study was aimed at verifying whether the cream influences the treatment's outcome and duration. Methods: An experimental, prospective, double-blind, randomized study was carried out. The pain was assessed through a compartmentalized numerical rating scale (CNRS). The effect was assessed through a four-point contraction qualitative scale. Results: After evaluating the pain scale, higher values were observed in the placebo group when compared to the group that used anesthetic, with statistical significance. Furthermore, there was no statistical difference in the efficacy and duration of effect over weeks 4, 8, 12, and 16. Conclusions: BoNT-A - Speywood Unit toxin was effective and safe for the treatment of glabellar and frontal wrinkles. The use of topical anesthetics (4% lidocaine cream) reduced the pain during the procedure. In addition, there was no interference in the toxin's efficacy and effect duration.
Keywords: BOTULINUM TOXIN TYPE A, LIDOCAINE, PAIN, THERAPY.
In 1817, Justinus Kerner first described the symptoms of a highly lethal, progressive paralysis associated with the ingestion of sausages, later known as botulism (from the Latin botulus, meaning sausage). 1 In 1895, Emile van Ermengen described the bacterial agent responsible for the disease and the agent's mechanism of toxic action.1
Botulinum toxin is one of the most potent bacterial toxins known to date. It is produced by the Clostridium botulinum, a gram-positive anaerobic bacteria in the form of a spore, commonly found in the soil and in marine environments. Eight immunologically distinct serotypes have been identified, of which seven (A, B, C1, D, E, F, and G) are neurotoxins. Although all neurotoxins are able to reduce the release of acetylcholine by the motor plate, they vary in size, cellular biosynthesis, and mechanism of action. Serotype A has the greatest neuromuscular blocking potency, with rare systemic effects, and has been used for several years with various therapeutic objectives, and is the first to be manufactured for clinical use.2 In 1980, the serotype described was introduced in medical practice for the treatment of strabismus.3
In 1982, after a multicentric study on the use of botulinum toxin type A for correcting strabismus and other facial muscle problems, one patient reported a reduction of glabellar wrinkles. This was the landmark case for the treatment of glabellar wrinkles with this product, with its results being published in 1988.4 Since then, botulinum toxin has seen increasing use, in isolation or associated with other facial rejuvenation techniques, and is currently one of the main procedures performed in dermatology practices.2
Several botulinum toxins are available in the market for clinical use: abobotulinumtoxinA (Dysport®, Ipsen Biopharm Limited-UK), onabotulinumtoxinA (Botox®, Allergan, Inc., Irvine, CA-USA), incobotulinumtoxinA (Xeomin® Merz Pharma, Frankfurt-Germany),5 Lanzhou type A-LBTXA (Prosigne, Cristália, China), among others.6 Botulinum toxin is manufactured from different strains of bacteria, undergoing various purification and stabilization processes, resulting in different chemical and biological properties. 7 Abobotulinumtoxina (Dysport-Ipsen Biopharm Limited-UK), a derivative of botulinum toxin A, has been used in Europe for the correction or mitigation of facial wrinkles for over two decades, and in April 2009 its use was approved by the U.S. FDA. It is measured in Speywood Units (s.U.), and collectively referred to as BoNT-A (Speywood Unit). 8 The product is sold in 300 s.U. and 500 s.U. vials. 8,9
Neuromuscular diseases, the use of aminoglycosides and anticholinergic drugs, pregnancy and lactation, and allergy to cow's milk are reported as contraindications. Unrealistic expectations area relative contraindication and must be thoroughly evaluated by the physician.10
Some adverse effects associated with the use of botulinum toxin type A in the treatment of dynamic wrinkles in the upper third of the face have been reported: headache, facial edema, sensation of facial swelling, palpebral ptosis, eyebrow ptosis, local pain and bruising, mild pruritus, and nausea. 6 Local pain during the procedure is one of the most important and limiting side effects of the technique. 6,10
For some patients, pain during the injection of the toxin may represent a limitation for undergoing the procedure. Topical anesthetic in the form of a dermatological cream offers a noninvasive and relatively safe analgesia in various dermatologic procedures, such as cutaneous fillings, curettage, electrocauterization, laser, and botulinum toxin application, among others. 11,12 The standard drug used is 4% lidocaine cream.12
The present study is aimed at determining whether the use of 4% lidocaine cream modifies pain during the application of botulinum toxin. In addition, it is intended to study whether the cream described affects the outcome and duration of treatment. The scarcity of scientific reports on the influence of the use of anesthetic cream and the effect of treatment justifies the study.
An experimental, prospective, double-blind, randomized study was conducted at the Cosmetic Dermatology Ambulatory of the Dermatology Clinic of the Santa Casa de Belo Horizonte, Minas Gerais-Brazil, in ambulatorial patients bearing glabellar and frontal hyperfunctional facial lines, from April 20-August 24, 2012.
Fifteen patients were included in the study, which was submitted to the Ethics Committee in Research, and all participants signed a Free and Informed Term of Consent.
The patients were randomized: half the glabellar and frontal region received topical anesthetic cream (4% lidocaine cream) applied to the injection points, and the other half received a pure cream vehicle (Figure 1).
Each vial containing 500s.U. of abobotulinumtoxinA (Dysport® Ipsen Biopharm Limited-UK) was diluted in 2 ml of 0.9% saline solution without preservatives, resulting in a concentration of 250 s.U./ml. The syringe used in the dilution process was the BD ultrafine II 100UI, with all vials used being from the same batch (D31307 exp. date 05/2013). The application was performed immediately after dilution.
Each patient received 100 s.U. of BoNT-A treatment, as follows: eight points in the frontal muscle, each with 5 s.U. (0.02 ml of the dilution), totaling 40 s.U., and five glabellar points, totaling 60 s.U. (one point in the procerus muscle-20 s.U., 0.08 ml of the dilution and four points in the corrugator muscles-10 s.U., 0.04 ml each point). BD ultrafine II 30 UI syringes were used for injection.
The study was double-blind and the applications of the topical anesthetic and the vehicle were carried out by a research assistant. The injection of botulinum toxin was performed by the main investigator physician, who was also responsible for assessing the effectiveness and duration of effect of the botulinum toxin, and was unaware of which area was treated with topical anesthetic or placebo.
The patients were assessed immediately after the procedure for the verification of pain, through the compartmentalized numerical grading scale (EGNC) 13 and in weeks 4, 8,12, and 16, for the verification of efficacy and duration of treatment effect through photographic analysis and qualitative scale of four-point contraction. 14,15
The photographic analysis was carried out at each visit, with patients being photographed at rest and at maximal contraction of muscles. All photographs were taken with the same digital camera respecting parameters regarding body site, background, and distance.
The following inclusion criteria were observed: women with hyperfunctional glabellar and frontal lines, age over 18, and signature on a Free and Informed Term of Consent.
The following exclusion criteria were observed: pregnant and lactating women, patients with infection in the application site, patients with a known hypersensitivity to one of the contents of the anesthetic cream or botulinum toxin, patients with psychological instability and unrealistic desires regarding the treatment, patients who rely on facial mimicry for their work, patients bearing neuromuscular diseases such as myasthenia gravis or Eaton-Lambert syndrome, patients taking drugs such as aminoglycosides, penicillamine, kinins, or calcium channel inhibitors.
The studied variables-pain and degree of paralysis-were analyzed according to the presence or absence of anesthetic. Initially, a characterization of the sample by means of frequency distribution tables, and central tendency and variability measures, was performed. To check for differences between groups-control (placebo) and experimental (anesthetic)-the Pearson's Chi-square test or Fisher's exact test were employed for comparing proportions. To compare continuous variables, the nonparametric test of Mann-Whitney, suitable for comparing two groups, was used. The intraclass correlation coefficient was used to assess the correlation between the physician's and the patient's assessments. In all analyses a 5% significance level was adopted. The software SPSS 15.0 was used.
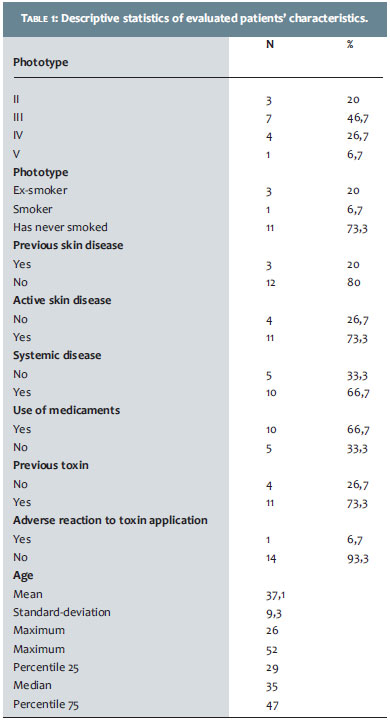
Fifteen patients 26- to 52-years-old (mean = 37-years-old) (Table 1) were evaluated. All were originally from urban regions (information not shown in the table). Most had phototype III (46.7%) and 73.3% had never smoked. The prevalence of prior skin disease was 20% (73.3% of active disease and 66.7% of systemic disease). It is worth noting that the prior skin disease reported was acne, and the active disease was melasma. Arterial hypertension, asthma, lupus syndrome NEM-2 A were informed as systemic diseases. Pharmaceutical use was reported in 66.7% of cases, with contraceptives being the most frequently declared. The majority of respondents reported previous use of botulinum toxin (73.3%), and only one patient (6.7%) mentioned adverse reaction.
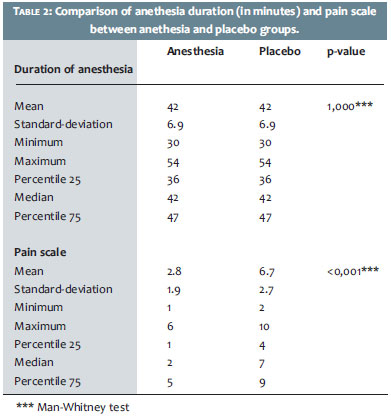
According to the results presented in Table 2, the values for the anesthesia duration were similar in both groups, with an average of 42 minutes (min = 30' and max = 54'). On the pain scale, higher mean and median values were observed in the placebo group when compared to the anesthetic group, with a statistically significant difference (p-value < 0.05).
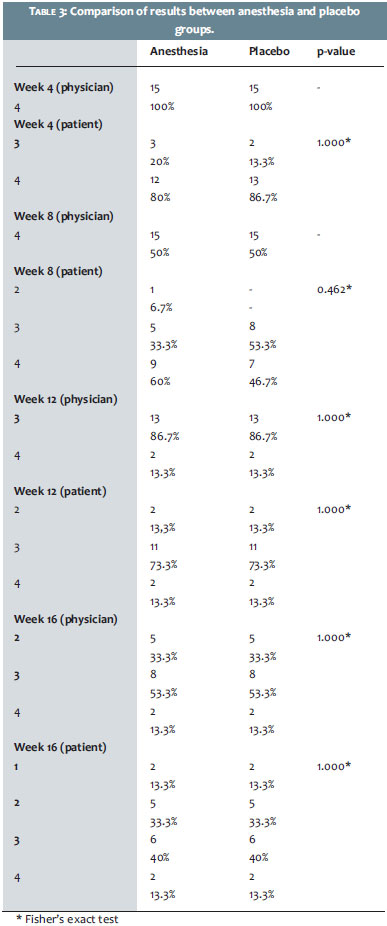
According to the results shown in Table 3, the physician's assessment in week 4 attributed a score of 4to both the anesthetic and the placebo group. In that same week, according to the patients' evaluation, 80% of the anesthetic group and 86.7% of the placebo group received a score of 4. In week 8, in the physician assessment, both groups had a score of 4. In the evaluation of patients, 60% of the anesthetic group and 46.7% in the placebo group received that score. In weeks 12 and 16 an identical percentage was observed in the comparison between the two groups. The prevalence of a score of 4 was 13.3% in both weeks, both in the physician's and the patients' evaluations. There were no significant differences between groups in any of the evaluations (p-values > 0.05).
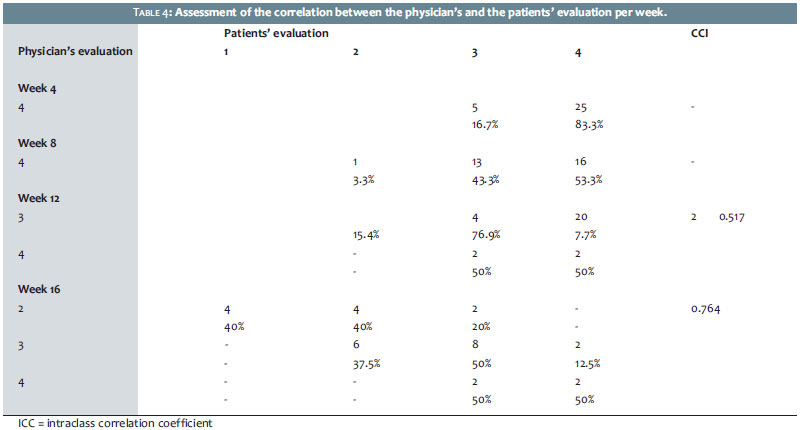
Table 4 shows the correlation between the assessments carried out by the physician and the patient. Due to the fact that it is a case of correlation between two ordinal variables (physician's assessment x patient's assessment) the intraclass correlation coefficient was used. For weeks 4 and 8 it was not possible to carry out an estimate due to the lack of variability in the physician's assessment (which attributed a score of 4 for all patients).
As for week 12, the correlation between the two assessments can be classified as moderate (0.517) and in week 16, the correlation was good (0.764).
The mean age of the treated group was 37 years (range = 26-52 years). This finding reinforces the use of botulinum toxin for the correction of hyperfunctional wrinkles of the facial muscles, which was more frequent in that age group. Only one patient (6.7%) reported adverse reaction to the treatment: local pain for three days in the points of application and a sensation that the eyebrow had "sunk", a fact that was not confirmed by the dermatological clinical examination.
The visual analogue scale (VAS) and the compartmentalized numeric graded scale (EGNC) are commonly used to evaluate the intensity and severity of pain. Its use is justified by the reproducibility, and can be used both clinically and in research. The VAS consists of a straight, not numbered, ten-centimeter line, presented on a blank sheet, where the left end means an absence of pain and the right end, the greatest level of pain perceived by the patient. It is one of the most-used scales for measuring pathological pain for scientific purposes, since it allows for the minimizing of the subjective factor. Another variation of thistype of scale would be the EGNC, which is numbered from 0 to10, in ascending order, from the left to right within a frame. The minimum value measured means absence of pain, and the maximum value, a greater intensity of pain; the patient chooses the number that best represents his or her perception of pain. 13
In developing countries, the best option is the EGNC scale, which presents greater ease of interpretation and makes it therefore more accessible to patients with a low level of education. In EGNC pain is expressed in numbers and patients tend to prefer it to quantify their pain; 13 in this study, it was the chosen scale for the assessment of pain.
There was a significant reduction in pain in the group treated with a topical anesthetic versus the one treated with the placebo: in the first, the average pain was 2.8 and in the second 6.7 (p < 0.001 %). The placebo group felt 2.4 times more pain than the anesthetic group. Anesthesia time ranged from 30 to 54 minutes (mean = 42 minutes).
Some studies tested the efficacy and safety of using topical lidocaine in botulinum toxin application. In 2010, Baumann et al. evaluated 26 patients regarding pain during botulinum toxin application, concluding that there is a statistically significant reduction in pain, with proven efficacy when applying 4% lidocaine before theprocedure. 12 In 2005, Carruthers A. et al. also found similar effectiveness in a randomized double-blind study involving 24 patients. 16 These observations were confirmed by the present study.
In addition, it aimed at studying the interference of the use of a topical anesthetic in the effectiveness and duration of the effect of the treatment with BoNT-A (Speywood Unit). There is anatomical variability of the muscles in the frontal and glabellar regions, a fact that has generated interest and stimulated the realization of recent studies describing different patterns of contraction in these areas. These studies have reinforced the need for individualization of the points of application of botulinum toxin, based on those anatomical variations. 17,18 For standardization, conventional doses and points of application for the treatment of glabellar and frontal regions were used, following the literature data. 1,8 In a recent study about the international consensus for the use of botulinum toxin type A (BoNT-A, Speywood Unit), the recommended dose for the frontal region ranged from 20 to 60 s.U., and for the glabellar region the recommendation was 50 s.U. 8 In the present study, we used doses of 40 s.U. for the frontal region and 60 s.U. for the glabellar region.
The muscular mobility was evaluated both by the physician and the patient at each visit using a qualitative four-point scale (1 = unaltered, 2 = slightly reduced, 3 = moderately reduced, 4 = considerably reduced).14,15 The physician assessed the patients directly, and the volunteers observed themselves in mirrors.
There was no statistical difference in efficacy and duration of effect when the anesthetic and placebo groups were compared, over weeks 4, 8, 12, and 16, as can be seen in Table 3. The same table provides important information about the duration of the muscle paralysis throughout the study. It is possible to observe that in week 16, 66.6% of patients had moderately reduced muscle contraction (value = 3) or considerably reduced (value = 4), regardless of the side (anesthetic or pure vehicle), according to the physician's evaluation. In the patients' assessment, that ratio stood at 53.3%.
In week 16, the correlation between the observations relating to decreased muscle contraction assessed by the physician and the patients was good (intraclass correlation coefficient = 0.764). This demonstrates that at the end of four months there were no significant differences between doctor and patient in the evaluation of the BoNT-A, Speywood Unit's effect.
The BoNT-A, Speywood Unit toxin was effective and safe for the treatment of glabellar and frontal wrinkles. The application of topical anesthetic (4% lidocaine cream) reduced pain during the procedure. Furthermore, there was no interference in the efficacy and duration of the toxin's effect.
The authors would like to thank Galderma for supplyingthe BoNT-A, Speywood Unit botulinum toxin, and Amphora Farmácia de Manipulação, in particular Mrs. Karina de Sá Pedras, for dispensing the cream vehicle.
1. Carruthers A. Botulinum toxin type A: history and current cosmetic use in the upper face. Dis Mon. 2002;48(5):299-322.
2. Sattler G. Current and future botulinum neurotoxin type A preparations in aesthetics: a literature review. J Drugs Dermatol. 2010;9(9):1065-71.
3. Scott AB. Botulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology. 1980;87(10):1044-9.
4. Jankovic J. Botulinum A toxin in the treatment of blepharospasm. Adv Neurol. 1988;49:467-72.
5. Cymbalista NC. Resultados da aplicação de incobotulinumtoxinA em pacientes para correção de rugas dinâmicas. Surg Cosmet Dermatol. 2011;3(4):288-95.
6. Ferreira LM, Talarico S, Costa RO, Godoy A, Steiner D, Fleissig L, et al. Eficácia e tolerabilidade de uma nova toxina botulínica tipo a para tratamento estético de rugas faciais dinâmicas: estudo multicêntrico prospectivo de fase III. Surg Cosmet Dermatol. 2009;1(2):58-63.
7. Huang W, Foster JÁ, Rogachefsky AS. Pharmacology of botulinum toxin. J Am Acad Dermatol. 2000;43(2 pt 1):249-59.
8. Ascher B, Talarico S, Cassuto D, Escobar S, Hexsel D, Jaén P, et al. International consensus recomendations on the aesthetic usage of botulinum toxin type A (Speywood unit) - part I: upper facial wrinkles. J Eur Acad Dermatol Venereol. 2010:24(11):1278-84.
9. Kane M, Donofrio L, Ascher B, Hexsel D, Monheit G, Rzany B, et al. Expanding the use of neurotoxins in facial aesthetics: a consensus panel's assessmentand recommendations. J Drugs Dermatol. 2010:9(1 Suppl):s7-22.
10. Matarasso A, Shafer D. Botulinum neurotoxin type A-ABO (Dysport): clinical indications and practice guide. Aesthet Surg J. 2009:29(6 Suppl):S72-9.
11. Froes GC, Ottoni FA, Gontijo G. Anestésicos tópicos. Surg Cosmet Dermatol. 2010;2(2)111-16.
12. Baumann LS, Grunebaum L, Elsaie ML, Murdock J, Jablonka E, Figueras K, et al. Safety and efficacy of a rapid-acting topical 4% lidocaine gel in a unique drug delivery system. J Drugs Dermatol. 2010;9(12):1500-4.
13. Andrella GQ, Araújo PMP, Lima SMPF. Estudo comparativo entre duas escalas de dor e a aplicação em doentes. Estudos (Goiânia). 2007;34(1-2):21-34.
14. Hexsel DM, De Almeida AT, Rutowitsch M, De Castro IA, Silveira VL, Gobatto DO, et al. Multicenter, double-blind study of the efficacy of injections with botulinum toxin type A reconstituted up to six consecutive weeks before application. Dermatol Surg. 2003;29(5):523-9.
15. Hexsel D, Rutowitsch MS, De Castro LC, Do Prado DZ, Lima MM. Blind multicenter study of the efficacy and safety of injections of a commercial preparation of botulinum toxin type A reconstituted up to 15 days before injection. Dermatol Surg. 2009;35(6):933-40.
16. Carruthers A, Caruthers J. Single-center, double-blind, randomized study to evaluate the efficacy of 4% lidocaine cream versus vehicle cream during botulinum toxin Type A treatments. Dermatol Surg. 2005;31(12):1655-9.
17. Almeida ART, Marques ERMC, Kadunc BV. Rugas glabelares: estudo piloto dos padrões de contração. Surg Cosmet Dermatol. 2010;2(1):23-8.
18. Braz AV, Sakuma TH. Estudo piloto dos padrões de contração do músculo frontal. Surg Cosmet Dermatol. 2010;2(3):191-4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}