


Frederico H. Sanchez1; Juliany Lima Estefan2; Lidiany Lima Estefan3
Introduction: Mohs micrographic surgery is a treatment option that increases the cure rate in various types of skin cancer, offering greater tissue preservation and lower recurrence rates. Objective: To describe clinically and histologically the tumors operated on with Mohs micrographic surgery, and to draw correlations to the number of stages and the type of surgical reconstruction performed. The operations were performed at a private clinic in the municipality of Rio de Janeiro, Brazil that is a specialist center for this technique. Methods: Retrospective, observational, cross-sectional/transversal study was carried out based on the review of medical records. Results: A study was conducted of 93 tumors in 84 patients, operated on between April 2010 and August 2012, and followed up with until August 2013 (12 to 42 months). Findings: 47.61% of patients were men and 52.38% were women, the mean age was 62.89 years; predominant phototypes: II (44%) and III (43%); 6 cases (6.45%) of squamous cell carcinoma, 87 (93.54%) of basal cell carcinoma; 74.19% were primary tumors; the nose was the most frequent site (46.24%); a single surgical stage was performed in most cases, with flaps (44%) being the more frequently performed type of closure. There was recurrence in one patient, who required reoperation in October 2012 and followed without new recurrence. Conclusions: Mohs surgery has proven effective with high cure rates and a minimal recurrence rate, especially in lesions located in the face's H area of risk.
Keywords: MOHS SURGRY, CARCINOMA, BASAL CELL, CARCINOMA, SQUAMOUS CELL.
Mohs micrographic surgery (MMS) is a therapeutic option for the treatment of various malignant neoplasms of the skin because it presents the highest cure rates combined with the lowest recurrence rates. It has the additional advantage of preserving the healthy tissue around the tumor, thus leading to less cosmetic and functional damage.1,2 MMS is the gold standard for the treatment of recurrent basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), primary tumors of aggressive histologic subtypes, tumors in embryonic clefts areas or in areas of difficult surgical reconstruction.1-3
With the micrographic technique, the tumor is removed with minimal surgical margins through a topographical mapping of the sample relative to its location on the patient. The sample is then prepared in a way that allows the histological analysis of all surgical margins (lateral and deep) in the same plane. The surgical specimen undergoes stages of tissue inclusion, freezing and preparation of histological sections, which are then stained and analyzed with a microscope. When the histological slide evidences permanence of the tumor, a new Mohs phase is required. The surgeon then, through the surgical mapping of the lesion, selectively widens the compromised surgical margin. According to some authors,1,2,4 while with the traditional freezing techniques (standardized by pathologists using the bread loaf or cut in cross techniques) the analysis covers only about 0.01% of the margins, the Mohs method allows the visualization of 100% of the surgical margins.
Although the Mohs micrographic technique was introduced in Brazil over 20 years ago and is the treatment of choice for many patients with aggressive or recurrent cutaneous tumors, it is still not widely used in the country, with only two articles found in the national literature about the use of this method in actual cases: Cernea4 (1994, São Paulo, SP, Brazil) and Chagas and Silva1 (2012, Aracaju, SE, Brazil). No articles discussing the Mohs technique in patients originating from the Brazilian state of Rio de Janeiro were found in the authors' literature search.
The purpose of the present article is to evaluate the clinical and histological profile of tumors operated through the Mohs micrographic method at a private MMS reference center in the municipality of Rio de Janeiro, studying its correlation to the number of phases and type of surgical reconstruction performed.
Ninety-three tumors were evaluated in 84 patients treated with the Mohs micrographic method in the Centro de Cirurgia Micrográfica do Rio de Janeiro (Center for Micrographic Surgery of Rio de Janeiro), from April 2010 to August 2012. A retrospective, observational, cross-sectional, descriptive study was carried out, with the data being collected through the analysis of the medical records and preoperative, intraoperative and postoperative photographs of 84 patients.
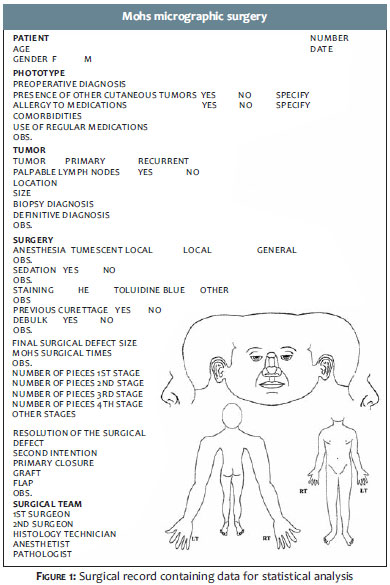
An operative record containing key patient data, that is part of the service protocol, served as the database for the study (Figure 1). The record form presented the following variables: date of surgery, patient age, gender, phototype, location of the tumor, histological type of tumor in the previous biopsy, histological type of the tumor assessed during surgery, classification in primary or recurrent tumor, number stages of Mohs surgery, type of surgical reconstruction, presence of lymph nodes, use of medication, comorbidities, dimensions of the tumor and of the resulting surgical defect after removal.
All patients signed a term of free and informed consent and a permission allowing the inclusion of personal data in the study, with guarantee of confidentiality.
All operated patients had previous biopsies, with tumors being classified according to histological type. The histological subtype was classified according to the previous biopsy or, where it was possible to detect the tumor remnant in the evaluated margins, according to the histological analysis carried out during the surgery. In case of inconsistency between histologic subtypes observed in the biopsy reports and in the blades analyzed during the surgery, the latter was chosen for assessment. Some tumors presented mixed characteristics, with more than one histological subtype in the same sample. In such cases, the most aggressive subtype was deemed the main tumor.
The tumors were further divided into categories of primary, recurrent, or incompletely excised-the latter being those with compromised surgical margins according to the histopathology carried out after conventional surgery, being then referred to Mohs micrographic surgery for the widening of margins.
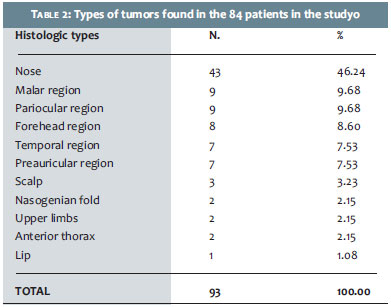
The authors classified the location of tumors as follows: trunk, upper limbs, nose, malar area, nasogenian sulcus, periauricular, periocular, scalp, temporal and forehead regions.
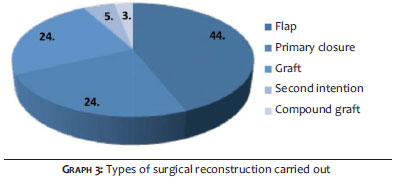
Regarding the type of surgical closure, the authors considered: primary closure, healing by secondary intention, flaps, simple grafts, and composite grafts.
Ninety-three tumors were analyzed in 84 patients-40 men (47.61%) and 44 women (52.38%), mean age of 62.89 years (SD ± 14.57), and median age of 65 years (minimum = 35 and maximum = 89 years).
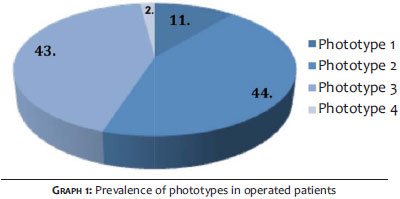
The predominant Fitzpatrick skin phototypes in the study were II (44%) and III (43%). Phototypes I and IV were also observed in 11% and 2% of cases, respectively (Graph 1).
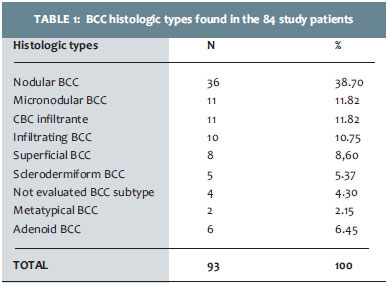
Regarding the histologic types, the study observed 6 (6.45%) SCC cases and 87 (93.54%) BCC cases, the latter being subdivided into 36 nodular BCC (one over a sebaceous nevus), 11 micronodular BCCs, 11 infiltrating BCCs, 10 superficial BCCs, 8 sclerodermiform BCCs,4 metatypical BCCs, 2 adenoid BCCs, and in five cases the subtype has not been evaluated. (Table 1)
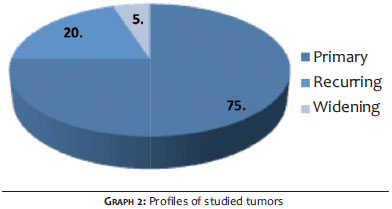
Of the 93 tumors operated through MMS, 69 (74.19%) were primary and 18 (19.35%)recurrent. In 6 cases (6.45%) there were no clinical recurrences of the lesions, nevertheless these cases were referred for expansion of surgical margins, due to the histopathologic diagnosis of BCC with compromised surgical margins after being operated with conventional techniques (Graph 2). Of these, in 5 cases (5.37%)it was not possible to identify the histological subtype, for the tumor was not observed during MMS, with previous reports showing no specification of the histological subtype. It was assumed that a tumor was not identified during Mohs surgery given that it is a peripheral technique, and surgical margins free of neoplasia were obtained in the initial stage of MMS.
Regarding the location of tumors, the majority (43/93, 46.24%) were located in the nose. Other locations were: 9 (9.68%) in the malar region, 9 (9.68%) in the periocular region, 8 (8.60%) in the frontal region, 7 (7.53%) in the temporal region, 7 (7.53%) in the periauricular region, 3(3.23%) in the scalp, 2 (2.15%) in the nasolabial folds, 2 (2.15%) in the upper limbs, 2 (2.15%) in the anterior thorax and 1 (1.08%) in the lip (Table 2).
Regarding the number of stages of the MMS, only one was observed in the majority (46/93, 49.46%) of cases. Two stages were observed in 25 (26.88%) cases, 3 in 17 (18.27%) cases, 4 in 2(2.15%) cases, 5 in 2 (2.15%) cases and 6 in 1(1.07%) case.
Of the examined cases, surgical margins free of neoplasia were not obtained in 2 patients. One of those patients had a BCC in the nasal wing area that recurred four times on the prior cutaneous flap, with an infiltrative pattern, that invaded the nasal septum and bone up until the right choana. The other patient had a poorly differentiated SCC in the pre-auricular region. Extensive invasion of the parotid gland was verified during the Mohs surgery. These patients were referred to the head and neck surgery and oncology services for radical surgery and radiotherapy.
To date (August 2013), the postoperative follow-up of these patients ranged from 12 to 42 months. In 47 (50.53%) patients, the follow-up period was of one to two years, and in 46 (49.46%), it was more than two years.
Recurrence was observed in only one patient during this period, 16 months after the first Mohs micrographic surgery was performed. It was a predominantly micronodular BCC casein the ear pinna that had recurred several times after cryosurgery and conventional surgery. The patient was re-operated using the Mohs method in October 2012 and to date has had no recurrence.
Regarding the surgical closure, 41 flaps, 22 simple grafts, 22 primary closures, and 3 compound grafts were performed. Five surgical defects were left to heal by secondary intention (Graph 3).
The mean age of patients was 62.89 years (SD±14.57), with a predominance of Fitzpatrick's skin phototypes II and III-findings that coincide with data found in the literature.
The literature describes male patients as the most affected by skin neoplasia.5,6 In the present study there was a predominance of female patients, with 52.38% (44/84) of cases, while male patients accounted for 47.61% (40/84) of cases. This difference was not significant and can be justified by the small size of the sample and by the fact that it focused only on cases referred for Mohs surgery.
Regarding the histological type, SCCs accounted for 6.45% and BCCs accounted for 93.54%, with the nodular subtype being found in 38.7% of cases. This finding was consistent with the literature, which describes BCC as the most frequent malignant neoplasm.3,5 Considering that the most aggressive histologic subtypes of BCC are the sclerodermiform, the infiltrative micronodular, and the metatypical, the present study included a large number of aggressive tumors (36.54%).
Of the 93 tumors studied, 74.19% were of the primary type and 19.35% were recurrent. This profile differs from the trend described by the Brazilian articles found in the authors' research. Chagas and Silva (2012)1 reported 62.7% recurrent tumors, and Cernea (1994)4 showed 56.1% recurrent tumors operated on using the Mohs technique. This misalignment may be due to socio-economic and regional factors, considering that this study was carried out in a private practice in the city of Rio de Janeiro, which may explain the fact that most of the operated tumors were primary. The smaller number of recurrent tumors in the present study is reflected in the number of stages required to achieve free surgical margins,2,7 even though as many as 50.54% of the analyzed tumors have required two or more stages.
Regarding the recurrence, although the follow-up time was still limited at the time the present article was written (12-42 months), recovery rates obtained were high, and when compared to those reported in the international literature corroborate the efficiency of the method in selected cases. Only one case of recurrence was detected, in an aggressive histological subtype tumor that had already recurred several times. Studies conducted with fewer than five years of followup demonstrated that recurring BCC lesions, when treated with traditional surgical techniques, achieved cure rates of roughly 82% after excision, while MMS increased that rate to 94.4%. 7
The most common locations of the tumors analyzed in the present study were: nose, malar, and periocular regions, coinciding with the "H zone of the face" area of risk, known by the presence of embryonic clefts that result in lower resistance to tumor infiltration, providing greater subclinical extension of lesions. 8,9 There is a formal indication of MMS in those cases, for it allows precise histological control, achieving high cure rates with low tumor recurrence rates.10
The present study has some limitations, such as the relatively small size of the sample and the limited follow-up time with the patients (1 to 3.5 years). This is justified by the facts that the MMS technique is still not widespread in Brazil and that the study has been conducted at a relatively new private practice (operations commenced in February 2010).
Despite the limitations, the Mohs surgical technique has proven its efficacy by achieving high cure rates with minimal recurrence rates. It was especially helpful in lesions located in the "H zone of the face" risk area-the majority in the present study-and in tumors of the aggressive histological subtype.
The authors suggest that further papers should be written describing studies with larger sample sizes and longer followup times, since there are few Brazilian articles on the subject.
2. Daniëlle IM. Kuijpers, Monique R.T.M. Thissenand Martino H.A. Neumann Basal Cell Carcinoma: Treatment Options and Prognosis, a Scientific Approach to a Common Malignancy. Am J Clin Dermatol 2002;3(4):247-59.
3. Ceilley RI, Del Rosso JQ. Current modalities and new advances in the treatment of basal cell carcinoma.InternationalJournalof. Int J Dermatol. 2006;45(5):489-98.
4. Cernea SS. Experiência do grupo de cirurgia micrográfica de Mohs do HCFMUSP: dezembro/1989 a abril/1993. An Bras Dermatol. 1994;69(5):365-73.
5. Leffell DJ, Fitzgerald DA. Basal cell carcinoma. In: Freedberg IM, Eisen AZ, Wolff K, Austin KF, Goldsmith LA, Katz SL, editors. Fitzpatrick's Dermatology in general medicine. 5th ed. New York: McGraw-Hill; 1999. p. 857-64.
6. Salasche SJ, Amonette R. Morpheaform basal cell epitheliomas: study of subclinical extensions in a series of 51 cases. J Dermatol Surg Oncol. 1981;7(5):387-94.
7. Maia M, Proença NG, Moraes JC. Risk factors for basal cell carcinoma: a case control study. Rev Saúde Pública.1995;29(1):27-37.
8. Kopke LFF. Cirurgia micrográfica. In: Fonseca FP, Rocha PRS. Cirurgia ambulatorial. 3. ed. Rio de Janeiro: Editora Guanabara Koogan S.A.;1999. p.230-8.
9. Vuyk HD, Lohuis PJ. Mohs micrographic surgery for facial skin cancer. Clin Otolaryngol Allied Sci. 2001;26(4):265-73.
10. Nouri K, Ballard CJ, Patel AR, Brasie RA. Basal cell carcinoma. In: Skin Cancer. Nouri K. New York: Mc Graw Hill ; 2007.p. 61-85.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}