


Luciane Francisca Fernandes Botelho1; Raquel P.R. Castro2; Juliana Casagrande Tavoloni Braga3; Sergio Henrique Hirata4; João Pedreira Duprat Neto5; Gisele Gargantini Rezze6
Introduction: In vivo confocal microscopy is an auxiliary non-invasive diagnostic method used in the diagnosis of hyperpigmented lesions in scars. Objectives: To evaluate hyperpigmentation in the scars of benign and malignant melanocytic lesions through confocal microscopy examination. Methods: Clinical, dermoscopic, and confocal microscopy images of fourteen patients with hyperpigmentation in adequately treated melanoma scars and in excised melanocytic nevi, were evaluated. Results: Among the eight patients with hyperpigmentation in melanoma scars, four showed no suspicious structures after confocal microscopy examination and four showed suspicious structures. Among the six patients with hyperpigmentation in areas where melanocytic nevi had been excised, three had atypical structures, such as dendritic cells and non demarcated papillae. Patients with suspicious structures underwent histological examination, with one case of hyperpigmentation in a lentigo maligna scar evidencing recurrence. Conclusions: The examination method allowed for the avoiding of biopsy in confirming the diagnosis in six of the fourteen patients. The finding of cells with dendritic or pagetoid pattern in the confocal microscopy examination means a diagnostic challenge, for it can indicate melanocytes or Langerhans cells in the spinous layer. Therefore, lesions that have such structures must be removed for histology and differential diagnosis.
Keywords: MELANOMA, NEVUS, DERMOSCOPY, CONFOCAL MICROSCOPY.
Hyperpigmentation in scars from melanocytic lesions constitutes a diagnostic challenge for the dermatologist, as it often presents nonspecific clinical and dermoscopic features.1 It can be classified clinically and histologically into the following categories: reactional cicatricial pigmentation, recurrent nevus, incompletely excised melanoma, or metastatic melanoma (locoregional cutaneous metastasis).2 More recently, different technologies have been developed in order to provide additional dynamic microscopic cutaneous information, without increasing morbidity.1-10 They allow both the in vivo diagnosis and real time assessment of disease progression.1-10
Confocal microscopy (CM) stands out as a new noninvasive diagnostic tool that allows for the acquisition of microscopic images and real-time in vivo visualization of cell and nuclear morphology.1-10 As a result, this technique has gained prominence as a tool in the differential diagnosis of melanocytic and non-melanocytic cutaneous tumors, and can be used in cases of hyperpigmentation in scars.1,3,9,10 CM correlates both with dermoscopy and histology.1-7 The fact that CM evaluates the tissue in the horizontal plane (like dermoscopy) and has high magnification with cellular level definition (like histology) implies that the first technique can be used as a bridge between the two latter methods and represents an important area for clinical research.1,9,10 For trained physicians, CM technology arises as a sensitive and specific tool in the early detection of melanoma and other cutaneous tumors.1,9,10 When conducted methodically and using diagnostic algorithms already described in the literature, CM allows a global architectural assessment of the epidermis, dermal-epidermal junction and upper dermis, as well as cytoarchitectural evaluation.9 Cellular atypia and pleomorphism, including certain nuclear morphologies, can be visualized in vivo, assisting in the diagnosis.1,2,9
The present study was aimed at evaluating clinical cases of hyperpigmentation scars in benign, malignant, and nonmalignant melanocytic lesions, using a non-invasive CM technique.
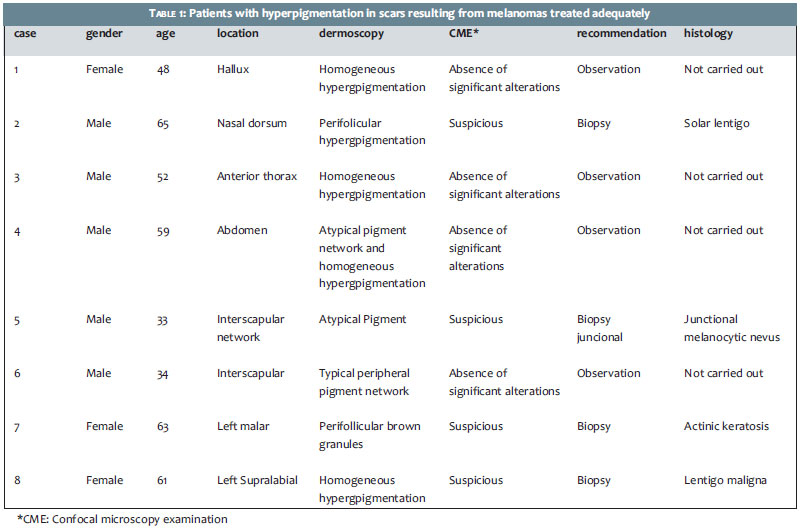
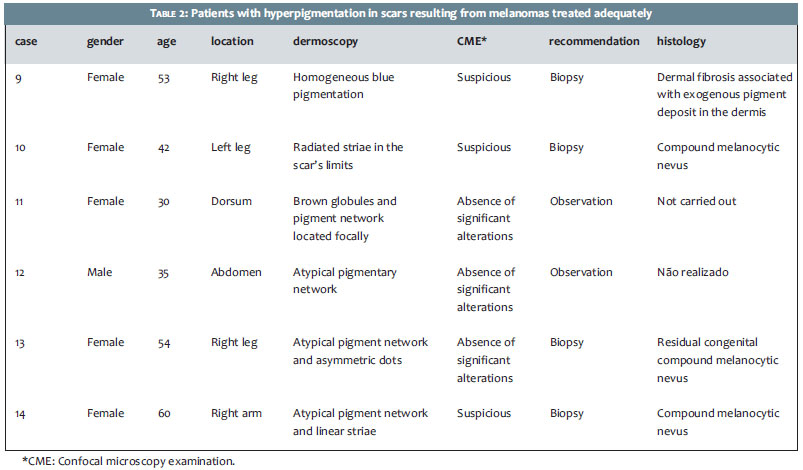
A retrospective, descriptive study, conducted at A.C. Camargo Cancer Center, in São Paulo, Brazil, included 14 patients: 8 with hyperpigmentation scars resulting from melanomas that were treated properly; and 6 with hyperpigmentation scars resulting from melanocytic nevi that had been previously excised. Dermoscopic and confocal microscopy images were evaluated by two experienced dermatologists (identified in the study as G.G.R. and J.C.T.B.).
The dermoscopic images were obtained using a Sony® Cyber Shot DSC-W290 12.1 MP digital camera, coupled to a DermLite II Pro HR (DermLite®) dermatoscope using the adapter (DermLite® II/III adapters). The confocal microscopy examination was carried out with the microscope VivaScope® 1500 and 3000 (Lucid-Tech, Rochester, New York, USA), depending on the location of the lesion to be analyzed. The confocal microscope and image acquisition methods have been described previously in the literature. 6-8 For each lesion analyzed with VivaScope® 1500, three mosaics were obtained at different skin levels (superficial epidermis, dermal-epidermal junction, and papillary dermis) based on the use of a protocol for pigmented lesions.9 In lesions examined through VivaScope® 3000, individual images (0.5 x 0.5 mm) were captured in sequence (Z stacks) from the surface (stratum corneum) to deeper levels (superficial reticular dermis), in the areas of interest.
The patients who showed suspicious structures through confocal microscopy (pagetoid cells, dendritic cells, nucleated rounded cells, not clearly demarcated papillae, and atypical nests in the dermal-epidermal junction) underwent a cutaneous biopsy of the pigmented area. After surgical exeresis, the tissue was sent to pathology, undergoing the standard routine of the Pathology Department of the A.C. Camargo Cancer Center. Patients who did not show suspicious structures remained under periodic dermatologic followup.
The present study evaluated 14 cases of hyperpigmentation scars in benign and malignant melanocytic lesions. Of the 8 patients with hyperpigmentation in melanoma scars, 4 had suspicious structures under confocal microscopy and underwent cutaneous biopsy with histological results of solar lentigo, junctional melanocytic nevus, actinic keratosis, and lentigo maligna (Table 1). Patients who did not show suspicious structures remained under periodic followup.
Of the 6 patients with hyperpigmentation scars in excised melanocytic nevus, 3 presented suspicious structures under confocal microscopy: intraepidermal dendritic cells and poorly demarcated papillae. These three patients underwent cutaneous biopsy, with the histology evidencing dermal fibrosis associated with exogenous pigment deposit in the superficial and deep dermis in one patient, and compound melanocytic nevus in two patients (Table 2). Despite not presenting suspicious structures in the confocal microscopy, patient number 13 requested that the recurrent nevus be excised.
Figure 1 illustrates a case of hyperpigmentation in an area where a melanocytic nevus (recurrent nevus) had been previously excised. The dermoscopic examination revealed the presence of radiated striae limiting the scar. Under confocal microscopy, the presence of great amounts of dendritic cells in the superficial epidermis could be observed. Although those suspicious structures could be visualized under confocal microscopy, the histological examination confirmed the diagnosis of compound melanocytic nevus.
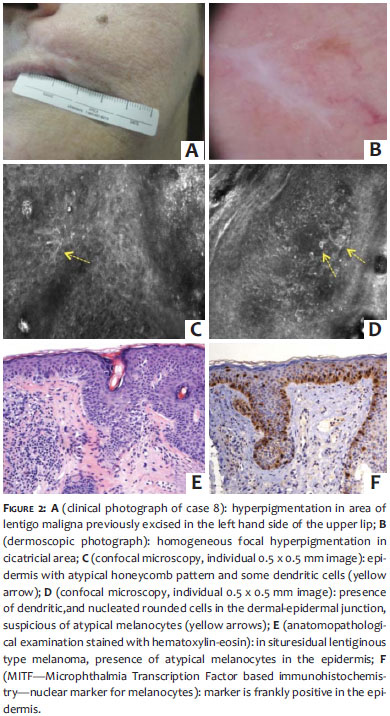
Figure 2 illustrates a case of recurrent lentigo maligna in the upper lip, previously treated with adequate surgical margins. Under dermoscopy, the presence of homogeneous focal hyperpigmentation in pericicatricial area can be observed. Under confocal microscopy examination, epidermis with atypical honeycomb pattern and some dendritic cells could be observed, with the presence of nucleated rounded dendritic cells, suspicious of atypical melanocytes, in the dermal-epidermal junction. The histological examination confirmed the diagnosis of recurrent lentigo maligna.
Pigmentation in scars of melanocytic lesions can be secondary to reactive phenomena linked to the healing process or can result from a recurrence of an excised melanocytic lesion.1,2 Recurrent nevi are benign, however they can present morphological characteristics that simulate melanoma.1,2 The appearance of pigmentation in melanoma scars is not uncommon and may raise doubts about the persistence of the tumor.1,2 CM is a noninvasive and reliable method that can assist in that differentiation. 2,4
Intraepidermal Langerhans cells are visualized in CM examination as dendritic cells, with long and thin dendrites. These cells are often difficult to differentiate from atypical melanocytes present in the suspicious melanocytic lesions, which are also visualized as dendritic cells or rounded and nucleated with pagetoid dissemination in the epidermis.5 Therefore, the presence of those dendritic cells in scars of melanocytic lesions may indicate a reactional inflammatory phenomenon or proliferation of atypicalmelanocytes.1,2 The cells of the recurrent nevus viewed through confocal microscopy examination (as illustrated in Figure 1) are probably intraepidermal Langerhans cells secondary to the healing process. One opportunity to document the presence of these cells in future studies would be through the use of immunohistochemistry with the marker CD1a, the main marker for Langerhans cells.
One criterion that can assist in the diagnosis of recurrence of melanocytic lesions in scar is the fact that dendritic cells (in cases of recurrent nevi) do not extend beyond the scar-unlike with cases of recurrent melanoma. 1 In figure 2,a CM examination of the pericicatricial area of hyperpigmentation evidenced intraepidermal pagetoid cells and nucleated rounded dendritic cells in the dermal-epidermal junction that extended beyond the scar, suggesting the diagnosis of lentigo maligna, which was confirmed by the anatomopathologic examination.
Other authors who assessed hyperpigmentation areas in scars from melanocytic lesions, carried out cutaneous biopsies in all cases examined-even when the confocal microscopy findings did not evidence suspicious structures.1 In contrast, in the present study, only the lesions with intraepidermal dendritic cells were removed, for as discussed above, the presence of those cells may suggest both atypical melanocytes and Langerhans cells. The CM avoided the need for cutaneous biopsies in 6 of the 14 patients evaluated, who remain under periodic dermatologic follow up. The limitation of the present study was linked to the small number of patients included in the sample.
CM is a useful auxiliary tool in the evaluation of hyperpigmentation in scars resulting from melanomas and melanocytic nevi, avoiding unnecessary excision of benign lesions and providing a good degree of safety to the dermatologist in the follow-up of those cases.
1. Longo C, Moscarella E, Pepe P, Cesinaro AM, Casari A, Manfredini M, et al. Confocal microscopy of recurrent naevi and recurrent melanomas: a retrospective morphological study. Br J Dermatol.2011;165(1):61-8.
2. Botella-Estrada R, Nagore E, Sopena J, Cremades A, Alfaro A, Sanmartin O, et al. Clinical, dermoscopy and histological correlation study of melanotic pigmentations in excision scars of melanocytic tumours. Br J Dermatol. 2006;154(3):478-84.
3. Rito C, Pineiro-Maceira J. Reflectance confocal microscopy in the diagnosis of cutaneous melanoma. An Bras Dermatol. 2009;84(6):636-42.
4. Erfan N, Kang HY, Cardot-Leccia N, Chignon-Sicard B, Passeron T, Ortonne JP, et al. Reflectance confocal microscopy for recurrent lentigo maligna. Dermatol Surg. 2011;37(10):1519-24.
5. Hashemi P, Pulitzer MP, Scope A, Kovalyshyn I, Halpern AC, Marghoob AA. Langerhans cells and melanocytes share similar morphologic features under in vivo reflectance confocal microscopy: a challenge for melanoma diagnosis. J Am Acad Dermatol. 2012;66(3):452-62.
6. Rajadhyaksha M, Grossman M, Esterowitz D, Webb RH, Anderson RR. In vivo confocal scanning laser microscopy of human skin: melanin provides strong contrast. J Invest Dermatol. 1995;104(6):946-52.
7. Rajadhyaksha M, Gonzalez S, Zavislan JM, Anderson RR, Webb R H . In vivo confocal laser microscopy of human skin II: advances in instrumentation and comparison with histology. J Invest Dermatol. 1999;113(3):293-303.
8. Rajadhyaksha M. Confocal microscopy of skin cancers: Translational advances toward clinical utility. Conf Proc IEEE Eng Med Biol Soc. 2009;2009:3231-3.
9. Pellacani G, Guitera P, Longo C, Avramidis M, Seidenari S, Menzies S.The impact of in vivo reflectance confocal microscopy for the diagnostic accuracy of melanoma and equivocal melanocytic lesions.J Invest Dermatol. 2007;127(12):2759-65.
10. Gareau DS, Li Y, Huang B, Eastman Z, Nehal KS, Rajadhyaksha M. Confocal mosaicing microscopy in Mohs skin excisions: feasibility of rapid surgical pathology. J Biomed Opt. 2008;13(5):054001.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}