


Bruna Souza Felix Bravo1, Maria Claudia Almeida Issa1, Raul Luiz de Souza Muniz1, Carolina Martinez Torrado1
Keywords: CELLULITIS, ULTRASONOGRAPHY,TREATMENT OUTCOME
Gynoid lipodystrophy (GL), commonly known as cellulite, is considered by many to be an aesthetic disorder. This terminology was introduced by the French medical literature more than 150 years ago.1,2 Other terms, such as dermopanniculosis deformans and adiposis edematosa, are also used.3-5
It is estimated that between 85-95% of women have some degree of GL after puberty,6 which can be located in any body site containing adipose tissue.4 However, the hip, gluteal region, and lower limbs are the most susceptible areas.
There are four main hypotheses for the origin of GL, the first being the sexually dysmorphic architecture of the skin, based on gender-related differences. According to this theory, the skin depressions common to the appearance of GL are caused by fat herniation. The fat penetrates from the subcutaneous tissue in the dermal-epidermal interface through the inferior surface of a weakened dermis. Its presence was, confirmed by ultrasound. This is a characteristic of female anatomy.7-9 Some authors have studied autopsy specimens of the thighs of healthy women between 29-39 years old who had GL, comparing them with the thighs of men and women who did not have GL. The comparison revealed important characteristic differences in the micro-architecture of the fibers of the subcutaneous connective tissue of these groups. It also showed that this alteration was immediately below the dermal-epidermal interface. The conclusion was that the permanent depressions of GL are the result of the continuous and progressive stretching of the hypodermis' collagen fibers (in the vertical direction), entailing the weakening of the connective tissue, which allows for the herniation of the fat, also giving rise to the conjunctive tissue's septa alteration theory.10
Later on, it was postulated that the origin of GL could be related to vascular alterations. It is believed that the process originates from damage that occurs in the dermal vasculature, in response to alterations in the sphincters of the precapillary arterioles of the affected areas. This occurs in association with the deposition of glycosaminoglycans (GAGs) in the walls of the dermal capillaries and within the fundamental substance between the collagen and elastin networks.4 These changes would lead to increased capillary venous permeability and to the excessive retention of fluids within the dermis, among adipocytes, and between the lobular septa. This would occur due to the hydrophilic property of GAGs, increasing the interstitial pressure. The resulting edema generates cellular alterations and entails vascular compression and vessels ectasia, in addition to decreased venous return with tissue hypoxia. This leads to the thickening of the fibrous septa in the superficial adipose tissue and deep dermis, causing the mattress aspect of GL.11-13 Finally, some authors quote inflammatory factors as key pathophysiological agents of GL. Based on the complaint of sensitivity to compression of some GL patients, 2,14 Kligman 14 reported the diffuse appearance of chronic inflammatory cells in the fibrous septum of patients with GL. This inflammation leads to dermal adipolysis and atrophy. Other authors did not find inflammation in patients with GL.2,6,10
GL occurs in all races, but is more common in Caucasian women.15 Several predisposing factors, such as female gender, advanced age, heredity, ethnicity, and obesity, have been described.16 It is important to note that in all body sites where there is deposition of fat (in the female pattern), GL is observed. Nonetheless, a patient does not need to be obese in order for GL occur.6 On the other hand, overweight-or even obese-men have little or no expression of GL, which leads to the suggestion that the hormonal factor is determinant in the pathogenesis of this condition. Another factor that reinforces the hormonal influence hypothesis is the observation of the worsening or onset of GL associated with estrogen action, such as puberty, pregnancy, menstruation, and estrogen therapy.17 Other hormones are also associated. Insulin-which in patients with unbalanced diets and excessive consumption of fat and carbohydrates causes hyperinsulinemia-increases lipogenesis and inhibits lipolysis, thus generating fat accumulation. Another associated hormone is prolactin, which increases water retention, generating edema.18 Many etiopathogenic mechanisms are involved, and in most cases it is not possible to determine a single cause.
Among the available treatments is liposuction, a surgical method of removing fat aimed at reducing GL, which leaves unsatisfactory results in most cases-even possibly worsening the skin's appearance.11 Multiple topical treatments are used, aimed at improving the skin's appearance, such as the xanthines and retinoids. These substances are deemed effective, producing a slight change in the skin's irregularity after months of use, with continuous use being necessary to maintain its efficacy.19-21
Among the devices used, ultrasound has been developed with an aim at producing volumetric heating of the treated tissue and, secondarily, lipolysis, however more clinical studies are necessary.22 More recently, shockwave therapy, similar to that used in the treatment of nephrolithiasis,22 was described with significant improvement of GL. Two mechanisms have been described that have demonstrated the ability to perform the thermal modification of the skin's connective tissue: laser and radiofrequency (RF). RF produces heat through the action of an electric current between two dipoles, which is different from lasers, whose heat output is due to the absorption of photons (emitted by a source of light) by the tissue's chromophores.1 An advantage of RF is the possibility of using this technology in any skin phototype. RF works through two main mechanisms of action: producing dermal heating, and vasodilation. The thermal injury activates the inflammatory cascade and stimulates the synthesis of collagen by the fibroblasts (neocollagenesis), promoting the thickening of the dermis.1,23 Vasodilation leads to hyperemia and lymphatic draining in the adipose tissue.1 The association of mechanisms acting on the dermis and subcutaneous tissue provides the improvement of the skin's appearance.
RF devices produce electromagnetic currents using radiation in the 3kHz to 300 MHz frequency range. When the current is applied to the tissue, it encounters resistance due to the tissue's impedance-which is a property inherent to the type of tissue. This resistance to the passage of electric current converts the latter into thermal energy, producing heat.24,25
The energy used is computed through the formula , where:
I = current,
z = impedance,
t = time (seconds).
Therefore, the amount of energy produced depends on the current and the impedance of the target tissue. High impedance tissues, such as subcutaneous fat, generate large amounts of energy and have deeper thermal effects.25,26
Various RF delivery methods have been developed: monopolar, unipolar, bipolar, and fractional. RF devices operate in different ways according to the technique or technology. The monopolar RF system releases energy using one dipole located in the device's tip and another in contact with the patient's skin, which acts as a grounding or return electrode. The skin retraction effect is based on the principle of volumetric heating. The electrode is designed to uniformly disperse the energy through the skin surface, through a process called capacitive coupling, which creates a zone of higher temperature at a controlled depth of 3-6mm. The depth of the heat depends on the size and geometry of the tip used.25,26
The unipolar RF differs from other RF devices in that it does not produce electric current in the tissue. Rather, it produces high frequency electromagnetic radiation, resulting in a rapid alternating polarity of the electromagnetic field, inducing high frequency rotational oscillation in the wate rmolecules, which acts as the "chromophore". Such ultra-fast oscillations generate heat, which is then dissipated in the tissue. The electromagnetic wave phase produced by this device is controlled in such a way that it allows the penetration of heat in a tissue depth of up to 20mm. The heat produced by the movement of the water molecules allows the skin's surface temperature to stabilize in the range of 400ºC, while higher temperatures (50-75ºC) are obtained in the reticular dermis.1,16,25There is no return electrode in this RF modality, entailing that there is no need for the target to be static.1
The main difference between bipolar and monopolar RF is the configuration. The bipolar configuration consists of two active electrodes placed at a short distance from each other, with the current flowing between them and a penetration depth of approximately half the distance between the two electrodes. The main limitation of this configuration is the penetration,25 however it provides better control of the distribution of energy and less pain.
The fractional non-ablative RF consists of a new therapeutic approach. While some devices use electrodes, others use microneedles arranged in pairs, with bipolar energy being released between them. This energy generated by that RF produces areas of treated skin, sided by areas of untreated skin. In the treated areas, there is thermal damage of the deep dermal collagen, stimulating healing, dermal remodeling and formation of new collagen, elastin, and hyaluronic acid.26,27 The untreated areas-located between the treated areas-initially maintain the integrity of the skin, but in the long run serve as a reservoir of cells that promote and accelerate healing.28 All these RF systems generally have a cooling system to prevent epidermal heating and provide additional comfort to the patient. The most commonly reported side effects in RF-based treatments are transitional erythema, small and large blisters, echymosis, crusts, scars, and dyschromias, all resolving without complications.1,16
Despite the availability of multiple therapeutic modalities, there is little scientific evidence demonstrating the treatments' effectiveness. In fact, most of the evidence is anecdotal, subjective, or based on patients' self-evaluation.
The present study is aimed at evaluating the efficacy and safety of a unipolar RF device in the treatment of GL in the gluteal region and thighs, not only through dermatologic examination, but also through ultrasound, in order for a less subjective assessment to be carried out. Laboratory tests for lipid profile evaluation were aimed at assessing the possible interference of deep unipolar RF action in lipid metabolism.
A prospective, comparative (before-and-after), non-randomized and without control study was carried out in female patients with GL in the gluteal region and thighs. The treatment was performed at the authors' private practice. The proposed technology for the treatment was the Accent® high energy RF (Alma Laser Ltd. , Israel), with unipolar tip. The laser-based thermometer (Center 350) was used to take temperature measurements during the treatment.
The ultrasound device with 13MHz multifrequency transducer (General Electric, GE, model Voluson 730) was used to assess the thickness of the dermis and hypodermis before and after the treatment. The ultrasound examinations were performed at the private practice of one of the authors of the study (a radiologist physician). Numeric indices were used for the objective evaluation.
A Sony DSC H9 - super steady shot 8. 1 MP camera was used in the photographic study.
Additional laboratory tests were used to assess the safety of the proposed method.
The selection of patients was carried out by the two dermatologist physicians who performed the procedures. The clinical evaluation was carried out by two dermatologist physicians who were not involved in the project, with the assistance of the sagging and morphology photographic scale.29
Side effects, such as erythema, blisters, hematomas, echymosis, crusting, scarring and dyschromias, were evaluated according to the four-point scale: 1) absent, 2) mild, 3) moderate, 4) heavy.
The statistical analysis of dermal measures obtained from ultrasound was carried out using the Wilcoxon test (SPSS software, version 13).
Inclusion Criteria
The authors selected eight female volunteer patients aged 28-45 years, Fitzpatrick phototypes II to IV, BMI between 20 and 25, and who had grades II and III GL (Nurnberger - Muller scale) in the gluteal region and thighs. After receiving an explanation about the procedure and all stages of the study, the patients signed a term of consent and authorized the publication of photographs.
Exclusion Criteria
Infections or scars in the treatment site, pregnancy, use of a pacemaker or cardioverter, autoimmune disease, epilepsy, diabetes, and prior history of surgery or liposuction on the gluteal region and/or thighs.
Unipolar RF-based procedure
Four RF sessions were carried out on predetermined sites with intervals of two weeks. Patients were instructed not to change their eating habits or use any medication aimed at improving the firmness of the skin or GL during that period. The patients received follow up from the same physicians throughout the study period. The marking of the area to be treated (a total of 20cm2 for each gluteal region and thigh) was carried out with the patient in orthostatic position. Before the application of the RF, mineral oil was applied in the area, with the aim of facilitating the sliding of the device's tip on the skin, allowing better energy transfer.
During the treatment, the unipolar tip was kept in an upright position and in full contact with the skin, and was moved constantly in circular, horizontal, and vertical strokes for 10 minutes in each of the 10cm2 areas, with 5 to10 seconds intervals, every 30 seconds (20 cycles of 30 seconds).
The initial energy used ranged from 180W x 30 seconds = 5,400 joules = 109 J/cm2 to 220W x 30 seconds = 6,600 = 133 J/cm2, with 20 consecutive passes in each gluteal region. The initial energy was chosen based on the BMI of the patients (for BMIs between 20 and 22, the initial energy was 180W), (for BMIs between 22 and 25, the initial energy was 220W), being increased or decreased depending on the tolerance of the patients. Upon reaching the a 40ºC temperature, it was decreased by 10% in every 30-second cycle, with a view to providing comfort to the patient and alleviating side effects. Nevertheless, the temperature was always kept between 39-41ºC during the 10-minute procedure (for each 10cm2). The temperature was monitored with a digital thermometer after each of the 30-second cycles.
Neither cream, nor any type of massage or lymphatic drainage, was applied after the procedure.
The clinical analysis was carried out by comparing photographs of the morphology and the sagging of the patients' gluteal region and thighs both before, and 30 days after the treat-ment. The photonumeric scale of cellulite severity described by Dr. Doris Hexel et al.29 was used as a basis for that analysis. That scale shows photographs of different degrees of sagging and morphology of the cellulite, rating the severity from zero to three, as follows:
Morphology: 0) unaltered, 1) orange peel appearance, 2) cottage cheese appearance, 3) mattress appearance.
Sagging: 0) unaltered, 1) slightly sagging appearance, 2) moderate sagging appearance, 3) severe sagging appearance.
Before, and 30-days after, treatment photographs were compared with the photographs from the scale, and then subsequently graded. When there were changes of at least one point both in the morphology and in the sagging scales, clinical improvement was acknowledged.
Photographic evaluation
The photographs taken were standardized (same room, same professional photographer, camera fixed at the same place, patients standing up at the same distance from the camera). Pretreatment and 30-days after photographs were taken, with the patients' gluteal muscles both in the relaxed and contracted positions, from the posterior, left side, and right side views.
Complementary examinations and laboratory tests
Laboratory tests were carried out before, during, and after the treatment to evaluate possible endocrine and metabolic alterations.
Tests carried out before the treatment: blood count, erythrocyte sedimentation rate, glucose level, urea, creatinine, thyroid hormones (free T4 and TSH), lipid profile, hepatography.
In the third session, the lipid profile was carried out before the procedure and two hours after for the evaluation of possible alteration of serum lipids.
Tests carried out after the last session: blood count, lipid profile.
Ultrasonography
The ultrasound examination was always performed by the same radiologist physician, before the treatment, and 30-days after the last session.
The areas for sonographic evaluation were chosen randomly in the right thigh (supine position, with an isolation area of 10 x 10cm located 15cm below the anterior superior iliac spine) and right gluteal region (prone position, just above the gluteal line, isolating the inferomedial region).
Measurements of the thickness of the dermis and hypo-dermis were taken. In the evaluation areas, the presence of vertical septa at the superficial hypodermis were verified and counted. The evaluation area's size was defined as having the same size of the transducer, which in almost all ultrasound devices measures from 38-40mm. The transducer was positioned in a way to allow the visualization of the maximum possible number of vertical and inclined septa. The septa represent the adipose tissue's interlobular trabeculae that connect the dermis to the fascia. Orifices were observed in the posterior dermis and measured in their diameter and thickness. Aiming at lending more objectivity to the sonographic evaluation, the radiologist physician created two indices to measure these orifices: the IFD and IFO, as described below:
IFD - Dermis' Base/Dermis'Total Thickness Index (Índice Fundo da Derme/Derme integral): obtained by dividing the distance from the bottom of the fat herniation entry orifice to the surface of the dermis, by the total thickness of the dermis.
IFO - Dermis' Base/Entry Orifice (Índice Fundo da Derme/Orifício de Abertura): obtained by dividing the distance from the bottom of the fat herniation entry orifice to the surface of the dermis, by the diameter of the entry orifice of the fat herniation.
This method allowed for the evaluation of alterations that occurred in the dermis and subcutaneous tissue in the GL area before and after the proposed treatment.
Statistical Analysis
The Wilcoxon test was applied in the analysis of the dermic measures obtained through ultrasound before, and 30days after the treatment, employing the software SPSS, version 13.
Any p values < 0. 05 were considered statistically significant for two related samples.
Clinical results
The evaluations of the morphological and sagging characteristics of the patients' gluteal regions were carried out through the comparison of photographs before, and 30 days after the treatment. In these evaluations, the evaluator physicians were able to correctly identify the pre-treatment and post-treatment photographs in 100% of the cases, for the four treatment sessions with unipolar RF (which were rated using a photonumeric scale). Regarding the sagging, the evaluator physicians determined a point on the scale at which the condition was considered to have improved, using this reference point for all eight patients. Regarding the morphology, there was improvement of one point in the scale in four of the eight patients (Figures 1 and 2).
Side-effects
The only side effect observed was moderate to intense transient erythema, with resolution within one to two hours after the treatment for all eight patients.
Laboratory tests
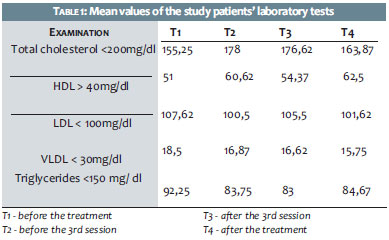
There werealterations in the pre-treatment exams. There was no pattern of alteration or increase comparatively significant in serum levels of cholesterol, HDL, LDL,VLDL or triglyceride in any of the evaluation phases (Table 1).
Ultrasonography
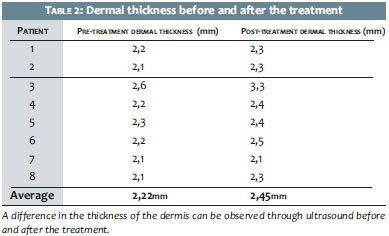
The measurement of the dermis showed increased thickness 30 days after the treatment-corresponding to three months after the first session-in seven of the eight patients treated. The greatest increase was 0. 6 mm after four sessions, and the smallest increase was 0. 1mm, with a total mean initial thickness of 2. 22 mm and total mean final thickness of 2. 45 mm (Table 2). The entry orifice for the herniated fat was found in three patients before the treatment. These orifices were not detected in the post-treatment examination, indicating the therapeutic efficacy of the therapy.
Statistics
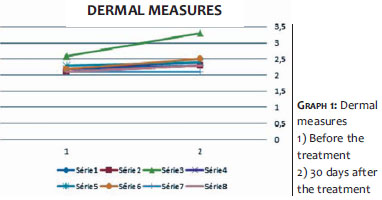
The statistical analysis based on the Wilcoxon test suggested a positive effect in the dermal measures with statistical significance p < 0. 05, showing an increase in the dermal thickness after four unipolar RF sessions (Graph 1).
Armenakas et al. 30 evaluated the efficacy and safety of unipolar RF in the improvement of the appearance of GL through a randomized, blind, and controlled study of 10 patients with cellulite grades II to IV on the thighs. The patients received up to six sessions of unipolar RF unilaterally (number of sessions at the discretion of the investigator), with fortnightly intervals. The thigh to be treated was chosen randomly, and the results were evaluated through questionnaires administered to the participants and to two blind evaluators, using photographs and a new quantitative classification system for GL. Patients were evaluated at one and three months after the treatment. All patients responded to the treatment, suggesting that favorable results that were clinically visible and measurable through a scale, were maintained three months after the treatment. That study-as well as the present study-has indicated unipolar RF's efficacy in the treatment of GL, despite the lack of an evaluation based on an imaging method.
Goldberg et al.16 evaluated the efficacy of the unipolar device (Accent RF System, Alma Lasers, Buffalo Grove, IL) in 30 patients with cellulite grades III and IV in the upper thigh. All were treated with a total of six sessions, applied in intervals of 15 days, and were evaluated before, and six months after the treatment through clinical photographs, clinical measurements, biopsies, MRI, and blood lipid tests. Twenty-seven patients had clinical improvement. The average reduction in the circumference of the leg was 2. 45cm. Histological alterations were reported, evidencing dermal fibrosis, however no alterations were observed in the treated patient's MRI or lipid levels. That study confirms the results obtained in the present study, showing efficacy in the treatment of GL with unipolar RF, with an absence of undesired effects on lipid metabolism. Nonetheless, the MRI's results recorded neither alteration in the adipose tissue nor in skin layers, a diverse result from that obtained in the present study. In the present study, the ultrasound evidenced a significant increase in the dermal thickness in most patients and the disappearance of the orifices generated by the herniation of dermal fat, which would translate into a dermal strengthening that would avoid the herniation of that layer, in turn suggesting the effectiveness of the treatment used in the present study.
Although MRI is the gold standard for the assessment of improvement in GL, 16 it is an expensive and difficult to access method. As evidenced by the present study, the ultrasound can be considered a good alternative method for the diagnosis and evaluation of the therapeutic response to unipolar RF treatment, for it allows the measurement of the dermis, the assessment of the septa, and fat herniation into the dermis.
Del Pino et al.1 conducted a study with 26 healthy women bearing visible bilateral GL grades I to III in both the gluteal regions and/or thighs, who underwent two RF unipolar sessions, with15-day intervals. The initial parameter was 150W x 30sec = 4,500 joules = 91 J/cm2, with three consecutive passes in each area during each session. This energy level was increased or decreased depending on the patient's tolerance or up until a temperature between 39º- 41ºC was reached in each treated zone. The evaluation of the subcutaneous tissue's thickness in the thigh and gluteal region took place prior to the first and second treatments, and 15 days after the second treatment through ultrasound examination, with photographs being taken to record the contour and superficial alterations. Measurements of the distance between the stratum corneum and the Camper's fascia, and from the stratum corneum to the muscle were taken. The authors evidenced that 68% of patients showed contraction of approximately 20% in the volume. The study shows that the use of ultrasound in the evaluation of results is a good, uncomplicated, and easy to access method, corroborating the present study's results.
Most studies use the measuring of the treated area's circumference and the photographic evaluation as a method to assess the response to proposed treatments.16,31 In the present study, not only the morphology and sagging of the skin were evaluated through a standardized clinical-photographic scale, but also the alterations detected in the dermis and hypodermis induced by the treatment with unipolar RF, contributing to an advanced understanding of the mechanism of action of the technique. Moreover, it was possible to assess the method's safety through laboratory tests.
The authors of the present study believe that the treatment with unipolar RF was effective for clinically improving the appearance of the GL in the gluteal region and thighs, while providing increased firmness and decreasing the skin's wavy appearance.
The increase in the dermal thickness and the reduced number of herniations of the subcutaneous tissue into the dermis-observed in the ultrasound evaluation-contribute to the understanding of the possible mechanisms of action of the unipolar RF, and corroborate the clinical effects observed.
The present study's results lead to the conclusion that the high-energy unipolar RF is an effective and safe method for the treatment of GL in the gluteal region and thighs, with clinically visible results just one month after treatment, with few local side effects, and an absence of serum alterations.
We would like to thank technician Ricardo Granato, who performed additional laboratory tests.
1. Emilia del Pino M, Rosado RH, Azuela A, Graciela Guzmán M, Argüelles D, Rodríguez C. Effect of controlled volumetric tissue heating with radiofrequency on cellulite an the subcutaneous tissue of the buttocks and thighs. J Drugs Dermatol. 2006;5(8):714-22.
2. Scherwitz C, Braun-Falco O. So-called cellulite. J Dermatol Surg Oncol. 1979;4(3):230-4.
3. Rossi AB, Vergnanini AL. Cellulite: a review. J Eur Acad Dermatol Venereol. 2000;14(4):251-62.
4. Lotti T, Ghersetich I, Grappone C, Dini G. Proteoglycans in So-called Cellulite. Int J Dermatol. 1990;29(4):272- 4.
5. Dahl PR, Zalla MJ, Winkelmann RK. Localized involutional lipoatrophy: a clinicopathologic study of 16 patients. J Am Acad Dermatol. 1996;35(4):523-8.
6. Nürnberger F, Müller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol. 1978;4(3):221-9.
7. Rosenbaum M, Prieto V, Hellmer J, Boschmann M, Krueger J, Leibel RL, et al. An exploratory investigation of the morphology and biochemistry of cellulite. Plast Reconstr Surg. 1998;101(7):1934-9.
8. Querleux B, Cornillon C, Jolivet O, Bittoun J. Anatomy and physiology of subcutaneous adipose tissue by in vivo magnetic resonance imaging and spectroscopy: relationships with sex and presence of cellulite. Skin Res Technol. 2002;8(2):118-24.
9. Avram MM. Cellulite: a review of its physiology and treatment. J Cosmet Laser Ther. 2004;6(4):181-5.
10. Piérard GE, Nizet JL, Piérard-Franchimont C. Cellulite: from standing fat herniation to hypodermal stretch marks. Am J Dermatopathol. 2000;22(1):34-7.
11. Draelos ZD, Marenus KD. Cellulite. Etiology and purported treatment. Dermatol Surg. 1997;23(12):1177-81.
12. Curri SB. Cellulite and fatty tissue microcirculation. Cosmet Toilet. 1993;108:51-8.
13. Curri SB, Bombardelli E. Local lipodystrophy and districtual micro-circulation. Cosmet Toilet. 1994;109:51-65.
14. Kligman AM. Cellulite: facts and fiction. J Geriatric Dermatol. 1997;5:136-9.
15. Draelos ZD. In serch of answers regarding cellulite. Cosmet Dermatol. 2001;14(1):55-8.
16. Goldberg DJ, Fazeli A, Berlin AL. Clinical, laboratory, and MRI analysis of cellulite treatment with a unipolar radiofrequency device. Dermatol Surg. 2008;34(2):204-9.
17. Ciporkin H, Paschoal LH. Atualizaçao terapéutica e fisiopatogenica da lipodistrofia ginoide "celilute". São Paulo: Editora Santos; 1992.
18. Isidori A. Fattori Predisponenti. In: Ribuffo A, Bartoletti CA, Editors. La celulite. Rome: Sallus; 1983. p. 49-59.
19. Jackson EM. Substantiating the efficacy of thigh creams. Cosmet Dermatol. 1995;8:31-41.
20. Piérard-Franchimont C, Piérard GE, Henry F, Vroome V, Cauwenbergh G. A randomized, placebo-controlled trial of topical retinol in the treatment of cellulite. Am J Clin Dermatol. 2000;1(6):369-74.
21. Goldman MP. Cellulite: a review of current treatments. Cosmet Dermatol. 2002;15:17-20.
22. Costa A, Pereira ESP, Alves CRT, Cruz FAM, Frigerio RM, Fidelis MC. Lipodistrofia ginoide e terapêutica clínica: análise crítica das publicações científicas disponíveis Surg Cosmet Dermatol. 2012;4(1):64-75.
23. Belenky I, Margulis A, Elman M, Bar-Yosef U, Paun SD. Exploring Channeling Optimized Radiofrequency Energy: a Review of Radiofrequency History and Applications in Esthetic Fields. Adv Ther. 2012;29(3):249-66.
24. Alster RS, Lupton JR. Nonablative cutaneus remodeling using radiofrequency devices. Clin Dermatol. 2007;25(5):487-91.
25. Elsaie ML. Cutaneus remodeling and photorejuvenation using radio-frequency devices. Indian J Dermatol. 2009;54(3):201-5.
26. Lolis MS, Goldberg DJ. Radiofrequency in cosmetic dermatology: a review. Dermatol Surg. 2012;38(11):1765-76.
27. Alexiades-Armenakas M, Rosenberg D, Renton B, Dover J, Arndt K. Blinded, randomized, quantitative grading comparison of minimally invasive, fractional radiofrequency and surgical face-lift to treat skin laxity. Arch Dermatol. 2010;146(4):396-405.
28. Hruza G, Taub AF, Collier SL, Mulholland SR. Skin rejuvenation and wrinkle reduction using a fractional radiofrequency system. J Drugs Dermatol. 2009;8(3):259-65.
29. Hexsel DM, Dal'forno T, Hexsel CL. A validated photonumeric cellulite severity scale. J Eur Acad Dermatol Venereol. 2009;23(5):523-8.
30. Alexiades-Armenakas M, Dover JS, Arndt KA. Unipolar radiofrequency treatment to improve the appearance of cellulite. J Cosmet Laser Ther. 2008;10(3):148-53.
31. Manuskiatti W, Wachirakaphan C, Lektrakul N, Varothai S. Circumference reduction and cellulite treatment with a TriPollar radio-frequency device: a pilot study. J Eur Acad Dermatol Venereol. 2009;23(7):820-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}