


Flávia Alvim Sant’Anna Addor1, Vanessa de Melo Silva1
Keywords: DERMATITIS, ATOPIC, SKIN CARE, PRURITUS, THERAPEUTICS
Atopic dermatitis is an inflammatory dermatosis in which the skin barrier's primary defect supports the continuity of the pathophysiology, making it more susceptible to pruritus, xerosis, and secondary infections.1 If not treated, xerosis can also exacerbate atopic dermatitis, as well as other inflammatory dermatoses. The defect in the skin barrier favors the release of inflammatory cytokines, which in turn triggera dermal inflammatory process, causing or worsening dermatitis. With increased transepidermal water loss resulting from this process, and with the increased contact with irritants and allergens, there is deterioration of the skin barrier's function, perpetuating the damage.2
In this scenario, any measure that can preserve and restore the skin barrier must be taken. Appropriate cleansing combined with the use of moisturizers stabilizes the barrier's function, limiting the conditions that favor irritation and helping to reduce the use of topical steroids, which disrupt the skin barrier's function in the long run, and predisposing it to infections.3 In regards to the cleansing process, it is important to establish a balance between removal residues and impurities, keeping the skin barrier and surface pH significantly unchanged, a fundamental condition for the equilibrium of the microflora (which helps in the prevention of infections).4,5 The normal pH of untouched skin is slightly acidic, between 5.5 and 6.5.6 Maintaining the pH level in this range involves the degradation of fillagrin into amino acids, which occurs during the keratinization process. It results in the formation of urocanic acid and induces the presence of fatty acids derived from NMF (natural moisturizing factor) and sebaceous glands, which are also produced by the lipases of normal microflora.7,8
In atopic patients, there is a trend towards increased pH levels. This phenomenon is caused by the reduction of proteolysis in the filaggrin, and is associated with altered synthesis of free fatty acids by sebaceous glands and epidermal phospholipids, which entails an increase in pH, particularly in the areas with lesions.9
This increase in the pH of the cutaneous surface is an important factor inalterations to the local microflora, causing a tendency towards infection by Staphylococcus aureus.10 There is evidence that at least 30% of patients with atopic dermatitis have a genetic deficit in the synthesis of filaggrin, loricrin, and ceramide, as well as of antimicrobial peptides.11 In this context, surfactants are of paramount importance, given that they are responsible for the emulsification of lipids in the skin's surface. Syndets (synthetic detergents) have a milder degreasing action, with a neutral or slightly acidic pH, and do not promote the alcalinization of the cutaneous surface.12,13
Syndets have the least amount of surfactants (surface active agents), which are compounds responsible for the adsorption of impurities on the surface, forming micelles.14 Some studies suggest clinical improvement of eczematous lesions through continuous cleansing with the use of syndets, including in children.15,16
There is an absence of studies on the behavior of atopic skin with regard to its cleansing with the use of products specifically developed for this purpose. The present study was aimed at evaluating the tolerance and impact on the symptoms of atopic dermatitis when exposed to a skin cleanser specially developed for atopic skin, measuring its effects on hydration, pH, and the skin barrier through measurements of transepidermal water loss.
A prospective, controlled study was conducted in June and July 2011, at a private clinical research laboratory (Medcin Instituto da Pele), in the city of Osasco (SP), Brazil.
The study population consisted of 33 male and female adult patients, between the ages of 18- and 50-years-old, with a clinical diagnosis of mild atopic dermatitis (according to Hanifin and Rajka criteria) without active lesions at the time of admission, and who hadn't used medication for up to four weeks prior to inclusion.
Patients with acute eczematous dermatitis who required immediate medicament-based therapy, or who were under the use of oral or topical corticosteroids, as well as any kind of topical or systemic medication that could influence the inflammatory response, were not included.
After signing the free and informed term of consent, all participants were clinically evaluated at baseline for the parameter cutaneous xerosis, according to a five-point scale where: 1 = very xerotic skin; and 5 = hydrated skin with no sign of xerosis. Following the clinical examination, biophysical measurements were collected in order to assess the product's behavior regarding its effects on the skin barrier through hydration, transepidermal water loss, and cutaneous surface pH. The following equipment was used:
• Measurement of the stratum corneum's hydration: Corneometer® MPA 580 (Courage & Khazaka, Germany). The device gauges the electrical capacitance of the epidermis. Higher measured values indicate greater volumes of epidermal water.
• Measurement of transepidermal water loss:Tewameter® (Courage & Khazaka, Germany). It gauges the state of the barrier integrity regarding its capacity to retain water. Higher measured values indicate worse states of barrier integrity.
• Measurement of the pH levels of the skin's surface: Phmeter® (Courage & Khazaka, Germany). The scale varies from 1 to 14, with lower values indicating higher acidity and higher values suggesting greater alkalinity.
After a single application of the product on the forearm-by washing the evaluated area according to the product's use instructions-new corneometric and transepidermal water loss (TEWL) measurements were taken immediately after the washing process and then every hour for four hours. The pH measures were taken just before and again 15 minutes after the cleansing process. The contralateral forearm was used as the control area for all measurements taken, being washed in the same manner, however in this case only water was used.
All measurements were taken at room temperature and controlled humidity (24+2Cº and 50 + 5%, respectively), with the average of three measurements being recorded and used for the purposes of the study. These measurements were performed in order to assess the immediate impact of a single cleansing procedure with the shower gel.
Evaluation under use conditions
At the end of the instrumental evaluation, the volunteers were given a standardized bottle containing 400ml of facial and body cleanser gel (Nutratopic® emollient shower gel, Isdin, São Paulo SP, Brazil) and instructed to apply once a day at home, during bathing, for 28 + 2 days.
At the end of the study, subjective questionnaires were distributed to the participants for the evaluation of the following items: cleansing without drying, cleansing without irritation, improvement of pruritus, improvement of dryness and smoothness. The study protocol and the free and informed term of consent were previously approved by the Independent Ethics Committee.
All patients (N = 33) reached the end of the study. No adverse reaction was mentioned or detected in the clinical examination of the group treated with the emollient shower gel.
Instrumental assessment of the skin barrier
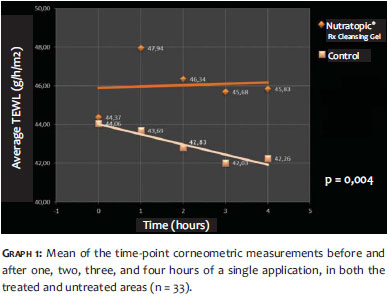
The following graphs illustrate the behavior of the mean of the instrumental measurements for the evaluated group after a single application of the emollient shower gel. (Graph 1)
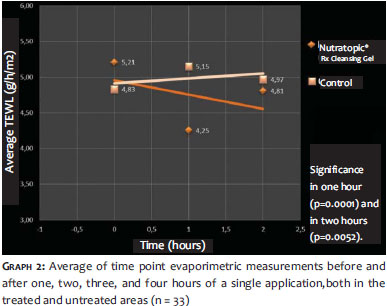
A significant improvement of corneometric levels was verified after a single cleansing procedure, within up to four hours after the application, when compared to the control (p = 0. 004). (Graph 2)
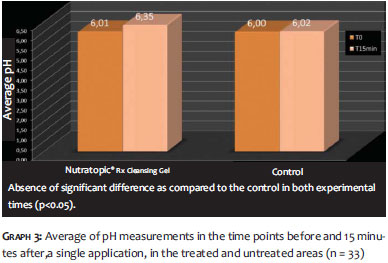
There were significant time reductions (by one hour, p = 0. 0001 and two hours, p = 0. 0052) for Nutratopic® Shower Gel as compared to the control, evidencing the cutaneous barrier's restorative effect. (Graph 3)
The variation of pH occurred within physiological parameters, with no significant difference when compared to the control (p <0. 05).
Statistical evaluation
All data were statistically analyzed through a Student's t-test, with a 5% significance level.
Clinical evaluation
Of the 33 patients evaluated in the treated group, none developed eczematous pattern lesions during the evaluation period. None of the patients presented a picture of a clinical worsening of the atopic dermatitis. Cutaneous xerosis: there was an improvement in the score used to measure xerosis. At baseline, the average scores obtained for xerosis was 2.9. Twenty-eight days after, the average of the scores rose to 4, suggesting a significant improvement in the clinical assessment (roughly 66%, p <0,01).
Subjective evaluation
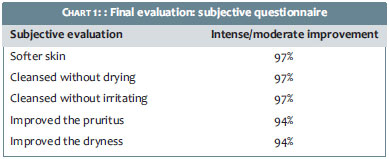
The subjective evaluation suggested significant improvement over time for all parameters assessed in the treated group, as shown in Chart 1.
Alterations in the cutaneous barrier are typical findings in atopic dermatitis, even in clinically uninjured skin.17 There is increased transepidermal water loss and lower water levels in the epidermis, which contribute to the perpetuation of the inflammatory picture, because it favors pruritus and secondary infections due to the elevation of the pH.18 The cleansing of atopic skin is a concern in the therapeutic approach. The dilapidation of the cutaneous surface during bathing increases the damage to the barrier, worsening the pruritus. Emollients often do not readily act on the recovery of the barrier and cannot completely prevent pruritus. Corticosteroids, in turn, increase the damage to the cutaneous barrier, inducing a vicious cycle.
For ethical reasons, the study was conducted on patients with mild atopic dermatitis without active lesions. Such patients many times do not use emollients routinely, which often undermines the prevention of recurrences.19 Patients in the present study had xerotic skin, with levels of around 44 corneometric units, as compared to eudermic skin, which often has above 55 corneometric units.20 The use of the studied syndet-based cleanser allowed the maintenance of previous hydration levels. With statistical significance, the data demonstrates that such a preservation level is not observed when the cleansing procedure is carried out with pure water. The same finding is observed in the main parameter that evaluates the cutaneous barrier (the transepidermal water loss), where there is no significant alteration-and even the presence of a slight improvement-a fact that is not observed when cleansing without any type of soap. This parameter is an important indicator of the integrity of the barrier.21 This data was clinically translated into the relief of typical symptoms of atopic dermatitis, such as pruritus and dryness. Even without the concomitant use of emollients, no discomfort was reported in any of the patients after continued use, with the majority considering its use as a factor of relief of symptoms. During the clinical examinations, the significant improvement in xerosis confirmed the impact of an adequate cleansing process for reducing the damage to the barrier. The cleansing action of soaps is effected by the detergent agents. In daily practice, only substances such as soaps and similar products are considered detergents. This is because of the fact that their molecules have a hydrophilic part (that attracts water molecules) and a lipophilic part (which is hydrophobic), and therefore emulsify fats or organic materials.
Surfactants are molecules that have detergent action. The spatial chemical structure of the molecules has two areas: polar (water soluble, hydrophilic) and nonpolar (not water soluble, hydrophobic).12 This chemical structure, which has dual polarity, interacts favorably with molecules-both water and non-water soluble molecules, such as oils and non-soluble silicones- and is responsible for the detergent action.
Soaps with synthetic surfactants (syndets) are composed of lipids that have undergone reactions such as ethoxylation, esterification, and others, but have not been saponified, and are milder than the classical surfactants. They lend a more acidic pH to the cleansing agent, with greater tolerability and lower reactivity with salts present in the water, in addition to imparting a softer feeling to the skin after its use.22 Many body care products contain surfactants for cleaning without irritation, nevertheless tolerance is higher only in those in which syndet surfactants predominate. Adding emollients in the formulation also lend softness to the cleansing process, particularly when the cleanser is specifically directed to xerotic skin, such as in the case of the product evaluated in the present study.
In a recent study, Cheong demonstrated that patients with alterations in the skin barrier benefit from gentle cleansing, which acts synergistically to hydration.23 Continued use of products with a slightly acid pH (physiological) helps to preserve the skin's natural pH and therefore reduces the risk of staphylococcal infections.24, 25 In addition, they do not cause a risk of sensitization and are more effective at removing impurities and bacteria.26 Currently, syndet based cleansers are the safest option for the treatment of the skin with alterations in the cutaneous barrier, such as atopic dermatitis.
The preservation of the cutaneous barrier is a fundamental requisite in the treatment of atopic skin, in which xerosis may worsen with the use of common soaps. Cleansing with a syndet product, such as the shower gel analyzed in the present study, demonstrates that not only is there preservation of the integrity of parameters inherent to the cutaneous barrier, but there is also improvement in clinical signs and symptoms linked to xerosis, such as dryness and pruritus.
1. Elias PM, Wood LC, Feingold KR. Epidermal pathogenesis of inflammatory dermatoses. Am J Contact Derm. 1999;10(3):119-26.
2. Loden M. Role of topical emollients and moisturizers in the treatment of dry skin barrier disorders. Am J Clin Dermatol. 2003;4(11):771-88.
3. Simpson EL, Hanifin JM. Atopic dermatitis. J Am Acad Dermatol. 2005;53(1):115-28.
4. Bikowski J. The use of cleansers as therapeutic concomitants in various dermatologic disorders. 2001;68(5 suppl):12-9.
5. Schmid-Wendtner MH, Korting HC. The pH of the skin surface and its impact on the barrier function. Skin Pharmacol Physiol. 2006;19(6):296-302.
6. Hachem JP, Man MQ, Crumrine D, Uchida Y, Brown BE, Rogiers V, et al. Sustained serine protease activity by prolonged increase in pH leads to degradation of lipid processing enzymes and profound alterations of barrier function and stratum corneum integrity. J Invest Dermatol. 2005;125(3):510-20.
7. Kezic S, Kemperman PM, Koster ES, de Jongh CM, Thio HB, Campbell LE, et al. Loss-of-function mutationsin the filaggrin gene lead to reduced level of natural moisturizing factor in the stratum corneum. J Invest Dermatol. 2008;128(8):2117-9.
8. Fluhr JW, Darlenski R. Skin barrier. In: Revuz J, et al, editors. LifeThreatening Dermatoses and Emergencies in Dermatology. Heidelberg, Germany: Springer-Verlag; 2009. p. 3-18.
9. Knor T, Meholjic-Fetahovic A, Mehmedagic A. Stratum corneum hydration and skin surface pH in patients with atopic dermatitis. Acta Dermatovenerol Croat. 2011;19(4):242-7.
10. Rippke F, Schreiner V, Doering T, Maibach HI. Stratum corneum pH in atopic dermatitis: impact on skin barrier function andcolonization with Staphylococcus Aureus. Am J Clin Dermatol. 2004;5(4):217-23.
11. Boniface K, Bernard FX, Garcia M, Gurney AL, Lecron JC, Morel F. IL-22 inhibits epidermal differentiation and induces proinflammatory gene expression and migration of human keratinocytes. J Immunol. 2005;174(6):3695-702.
12. Abbas S, Goldberg JW, Massaro M. Personal cleanser technology and clinical performance. Dermatol Ther. 2004;17(Suppl 1):35-42.
13. Korting HC, Hübner K, Greiner K, Hamm G, Braun-Falco O. Differences in the skin surface pH and bacterial microflora due to the long-term application of synthetic detergent preparations of pH 5.5 and pH 7.0. Results of a crossover trial in healthy volunteers. Acta Derm Venereol. 1990;70(5):429-31.
14. Del Rosso JQ. Understanding skin cleansers and moisturizers: the correlation of formulation science with the art of clinical use. Cosmet Dermatol. 2003;16:19-31.
15. Solodkin G, Chaudhari U, Subramanyan K, Johnson AW,Yan X, Gottlieb A. Benefits of mild cleansing: synthetic surfactant based (syndet) bars for patients with atopic dermatitis. Cutis. 2006;77(5):317-24.
16. Lavender T, Bedwell C, O'Brien E, Cork MJ, Turner M, Hart A. Infant skin-cleansing product versus water: a pilot randomized, assessor-blinded controlled trial. BMC Pediatr. 2011;11:35.
17. Addor FAS, Aoki V. Barreira cutânea na dermatite atópica. An Bras Dermatol. 2010;85(2):184-94.
18. Proksch E, Jensen JM, Elias PM. Skin lipids and epidermal differentiation in atopic dermatitis. Clin Dermatol. 2003;21(2):134-44.
19. Lebwohl M, Herrmann LG. Impaired skin barrier function in dermatologic disease and repair with moisturization. Cutis. 2005;76(6 Suppl):7-12.
20. Elkhyat A, Agache P, Zahouani H, Humbert P. A new method to measure in vivo human skin hydrophobia. Int J Cosm Sci. 2001;23(6):347-52.
21. Holm EA, Wulf HC, Thomassen L, Jemec GB. Instrumental assessment of atopic eczema: validation of transepidermal water loss, stratum corneum hydration, erythema, scaling, and edema. J Am Acad Dermatol. 2006;55(5):772-80.
22. Solodkin G, Chaudhari U, Subramanyan K, Johnson AW,Yan X, Gottlieb A. Benefits of mild cleansing: Synthetic surfactant based bars for patients with atopic dermatitis. Cutis. 2006;77(5):317-24.
23. Cheong WK. Gentle cleansing and moisturizing for patients with atopic dermatitis and sensitive skin. Am J Clin Dermatol. 2009; 10(Suppl 1):13-7.
24. Korting HC, Hübner K, Greiner H, Hamm G, Braun-Falco O (1990) Differences in skin surface pH and bacterial microflora due to the long-term application of synthetic detergent preparations of pH 5.5 and pH 7.0. Results of a crossover trial in healthy volunteers. Acta Derm Venereol. 70(5):429-31.
25. Fadel APC, Almeida T, Fujita EM, Auada MP, Marinoni LP. Variações do pH dos sabonetes e indicações para sua utilização na pele normal e na pele doente. An Bras Dermatol. 2000;75(6):697-703.
26. Braun-Falco O, Korting HC. Syndets in the treatment of atopic eczema. In: Ring J, Przibilla B, Ruzicka T, editors. Handbook of atopic eczema. New York: Springer-Verlag; 2006.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}