


Milena Cordeiro Afradique1, Danielle de Paula Aguiar1, Maluf Marcos Gabbay Belicha1, Dina Zylberztejn1, Bruna Souza Félix Bravo1
Keywords: NEVUS OF OTA, TREATMENT OUTCOME, LASERS
The Nevus of Ota was initially described as Nevus fuscocaeruleus ophthalmomaxillaris, by Ota and Tanino in Japan in 1939.1 It is a dermal melanocytic nevus with low malignization potential, clinically characterized by a blue-grayish macula interspersed with smaller brownish macules located in the skin. It is innervated by the second and third branches of the facial nerve, and is often associated with ocular pigmentation and can occur in the nasal, palate, pharyngeal, or tympanic mucosa. It is usually unilateral, nevertheless 5-15% of cases can be bilateral.2
It occurs mainly in women of Asian origin, with a prevalence of 0.4-0.8% in the Japanese population, being rare in Caucasians. It has two peaks of onset: the first in the first two months of life (50-60% of cases), with most present at birth; and the second in adolescence (40-50% of cases). The onset between the ages of 1 to 11 years and after 20 years of age is unusual. The literature describes rare cases of familial Nevus of Ota, however no hereditary factor has been characterized.1-3
The Nevus of Ota may grow over time and persists throughout life, causing damage to the interpersonal relations of affected individuals.3
Its histology evidences normal epidermis and dermal dendritic fusiform melanocytes associated with abundant fine granules of melanin. In general, there is an absence of melanophages.4
Several treatments, such as surgery, electrosurgery, dermabrasion, cryotherapy, and chemical peels were described with minor responses or complications such as scarring and dyschromias.5-7 The best results were achieved with Q-switched lasers (QS lasers), which is the best laser to treat benign melanocytic pigmented lesions.3,7-10 QS laser types that stand out are the QS neodymium doped yttrium aluminum garnet (QS Nd:YAG) that operates at 1,064nm and 532nm (infrared and green light); the QS Ruby laser that operates at 694nm; and the QS Alexandrite that operates at 755nm.11-13
The introduction of laser therapy has emerged as a new tool for the therapeutic approach to various unaesthetic lesions. The principle of selective photothermolysis-which allows for acting on specific chromophores-lent objectivity to laser-based treatment, which uses prevailing parameters in each lesion (such as color variation, applicability, and relief) for the purpose of evaluation.3,7-19
The target-chromophore to be reached is melanin, and QS lasers' mechanism of action occurs through a photomechanical effect based on the generation of photoacoustic waves produced by the emitted photons, which heat the small particles of pigment and melanosomes, resulting in the formation of cavities within the cells, with subsequent rupture.3
The Alexandrite and Ruby lasers have shorter wavelengths, resulting in greater absorption by melanin, which increases the risk of dyschromias and epidermal damage. 17 The most severe side effects were rarely observed in studies-the majority of which were carried out in patients of Asian background-focused on QS lasers.
The present study was aimed at presenting the experience of the Cosmiatry Department of the Instituto de Dermatologia Professor Rubem David Azulay of the Santa Casa de Misericórdia do Rio de Janeiro (RJ), Brazil, in the treatment of the Nevus of Ota with 1,064/532nm QS Nd:YAG laser, in patients of western background with high skin phototypes.
A retrospective analysis was carried out based on medical records and on the active search for patients with Nevus of Ota who had been treated with the 1,064/532nm QS Nd:YAG laser, at the Cosmiatry Department of the Instituto de Dermatologia Professor Rubem David Azulay of the Santa Casa de Misericórdia do Rio de Janeiro. The equipment used in those treatments was the Victory Tattoo Removal Laser® (Beijing, China), with 1,064nm wavelength and converter to 532nm, with 10ns pulse duration, 3mm spot size, 5Hz frequency and 2 to 12J/cm2 fluence. All participant patients read and signed a Free and Informed Term of Consent before undergoing the treatment. An active search was carried out aimed at selecting patients for photographic reassessment and application of a questionnaire to analyze individual profiles, satisfaction, and effectiveness of the treatment. The assessment of the response to the treatment was carried out by both the patients and the physician researchers.
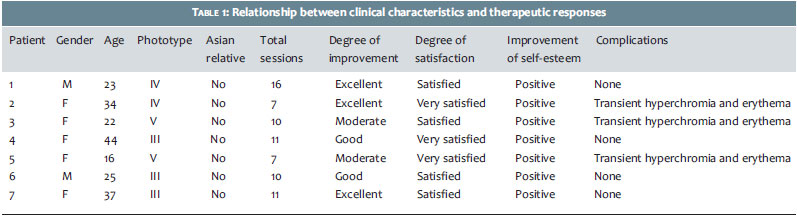
Inclusion criteria were: all patients with Nevus of Ota who had been treated with 1,064/532nm QS Nd:YAG laser at the Cosmiatry Department of the Instituto de Dermatologia Professor Rubem David Azulay of the Santa Casa de Misericórdia do Rio de Janeiro, from May 2007 to July 2011, independently of age, gender, or skin phototype, and who had no history of previous treatment. Exclusion criteria were: not being able to contact the patient, and patient attendance at fewer than five sessions. Fourteen patients were initially selected, with seven being withdrawn from the study for failing to meet the inclusion criteria specified above. The age range of patients was 16-44 years. Altogether, five female patients and two male patients-with phototypes III to V-were included. Only one patient had bilateral lesions (Table 1). The number of sessions varied from 7 to 16 (average = 10. 2), with an interval between sessions of 1 to 4 months, depending on the post-inflammatory hyperpigmentation degree and availability of the patient.
All patients underwent pre-procedure preparation and care for at least 15 days with the Kligman's modified formula and topical anesthetics under occlusion for 30 minutes before each session. Antibiotics and topical corticosteroids were prescribed during the post-procedure period for seven days, with patients being instructed about the necessary use of sunscreen. In adherence to the Cosmiatry Department's protocol, only the 1,064nm tip was used in the first session, with an absence of adverse effects, such as dyschromia and scars. The remaining sessions were carried out with the combination of 1,064nm and 532nm tips, in that order. Patients were photographed before each session. The period of re-evaluation of the response after the completion of the treatment ranged from 2 to 50 months.
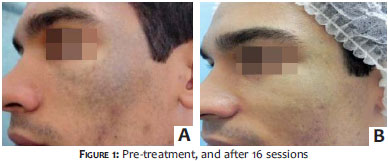
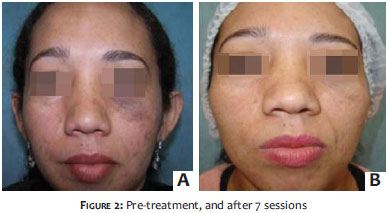
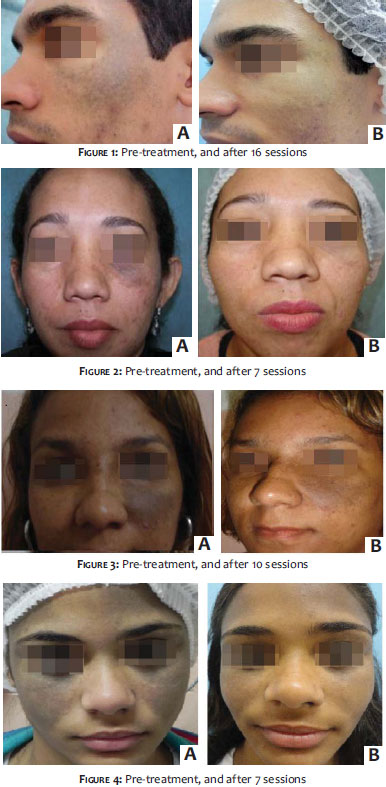
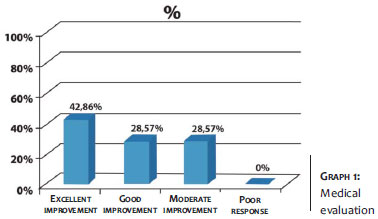
The relationship between the clinical characteristics and therapeutic response is shown in Table 1. Of the 14 patients with Nevus of Ota, 7 met the inclusion criteria previously established. There was no correlation between the degree of clinical improvement and the interval between sessions. Of the 7 patients, 3 had excellent improvement (greater than 75%), 2 had good response (improvement between 51-75%), two had moderate response (improvement between 25-50%). There was no poor response (Figure 1). The degree of patient satisfaction assessed through the questionnaire showed that 4 patients reported being very satisfied and 3 satisfied (Figure 2). Better results were observed in patients with phototypes up to IV, after seven treatment sessions. Hyperpigmentation, erythema, edema, and a burning sensation were reported in the immediate post-procedure in all patients, in addition to crusts 5-7 days after the start of the treatment. Three patients developed transient hyperchromia and erythema, which receded with the use of topical whiteners and sunscreen. There were no reports of hypopigmentation, scarring, secondary infection, or persistent complications. (Figures 1 to 4)
The pathogenesis of Nevus of Ota is still the subject of discussion. In the literature, 80% of cases are seen in women, which coincides with our study. The lesions occur mainly in patients of Asian origin, however none of the patients in the present study were of Asian origin. Most lesions can be identified from birth and are usually unilateral, however in 15% of cases they may be bilateral. In the present study, all patients had a lesion since birth, and one of the seven patients had a bilateral lesion, which also coincides with the literature's data.
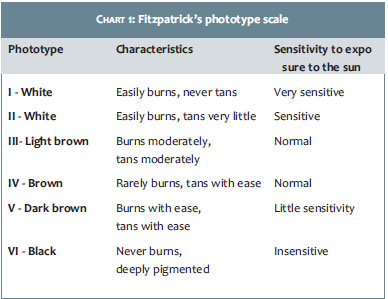
In the literature, studies are aimed at assessing the therapeutic response of Nevus of Ota in the Asian population, which typically has high skin phototypes according to the Fitzpatrick's classification (Chart 1). Nevertheless, Asian populations have distinct skin characteristics and colorations from that of this study (a Brazilian population), which due to miscegenation has numerous skin tones and different responses to light stimuli, creating a challenge in treating these patients.3,6-20
Geronemus RG 6 reported success with QS Nd:YAG laser and preference for using it in high phototypes, due to the longer wavelength and less epidermal damage, therefore minimizing complications. The 1,064nm wavelength was safer, for it reaches deeper levels of the dermis, sparing the epidermis. Thus, for being shallower, the 532nm tip presents a higher risk of dyschromia. 19 However, some authors suggest the concomitant use of the two tips for greater whitening of the lesions, a fact that was also observed in the present study.19
Few side effects were observed in studies with QS lasers, the main being: discomfort, edema, and erythema up until 48 hours after the application. A study with two patients of African origin with Nevus of Ota, treated with the 1,064nm tip of the QS Nd:YAG laser, concluded that the probability of dischromia depends more on the laser parameters than on the patient's phototype or number of sessions.8 The present study recommends the use of low fluences.
Regarding the side effects, the authors of the present study have the impression that the combined use of the two tips showed greater chance of post-inflammatory hyperchromia, which, however, was transient in all cases, with resolution after the use of whiteners and sunscreens. In the present study, the best results were obtained after the seventh session. It is worth noting that due to the fact that the group of patients in the present study presented higher phototypes (from III to V), a greater number of sessions were performed due to the higher risk of complications. However, no significant complications, such as permanent scarring or dyschromias, were observed.
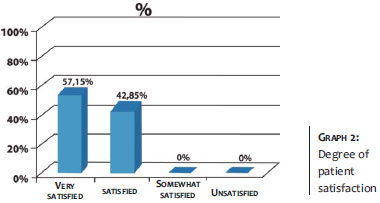
Hague JS et al.17 evaluated the degree of satisfaction of 67 patients bearing pigmented lesions treated with Nd:YAG and erbium:YAG, with a 21-month follow-up (27% had phototypes varying from IV to VI, average = 5. 4 completed sessions). Approximately 30% of patients reported excellent results. The most common injuries treated were congenital nevi and the Nevus of Ota. In the present study, the degree of patient satisfaction was measured through a questionnaire that showed that 57. 15% were very satisfied and 42. 85% were satisfied (Graph 2). The best results were observed in patients with Phototype IV, after seven treatment sessions.
Due to the fact that the present analysis was a retrospective study, the resulting analysis was of a clinical nature, based on the physician's evaluation (Graph 1) and on the degree of patient satisfaction (Graph 2). The QS Nd:YAG laser has proven useful and safe, even in a location subject to high ultraviolet radiation and with high patient skin phototypes. Although the present study was carried out in a western, miscigenated population, where no individual was of Asian descent, and clinical characteristics were distinct from those found in the literature, the epidemiological data and therapeutic responses were satisfactory and similar to those already described.
1. Ota M. Nevus fusco-caeruleus ophthalmic-maxillaris. Jap J Dermatol. 1939;46:369.
2. Mosher DB, Fitzpatrick TB, Ortonne JP, Hori Y. Disorders of pigmentation. In: Fitzpatrick TB, Eisen AZ, Wolff K et al. , eds. Dermatology in general Medicine, 4 th ed. New York: Mc Graw-Hill; 1993. p. 979.
3. Lowe NJ, Wieder JM, Sawcer D, Burrows P, Chalet Ml. Nevus of Ota: Treatment with high energy fluences of the Q-switched ruby laser. J Am Acad Dermatol. 1993;29(6):997-1001.
4. Lever WF, Schaumburg-Lever G. Histopathology of the skin. 7th ed. Philadelphia: JB Lippincott; 1990. p. 776-7.
5. Fujimori Y. Treatment of nevus of Ota and nevus spillus. Tokyo: Kokuseido;1990. p. 181-8.
6. Kobayashi T. Microsurgical treatment of nevus of Ota. J Dermatol Surg Oncol. 1991;17(12):936-1.
7. Cosman B, Apfellberg DB, Druker D. An effective cosmetic treatment for Ota's nevus. Ann Plast Surg. 1992;18:817-21.
8. Polnikorn N, Tanrattanakom S, Goldberg D. Treatment of Hori's Nevus with the Q-switched Nd:YAG laser. Dermatol Surg. 2000;26(5):477-80.
9. Suh D, Hwang J, Lee H, Youn J, Kim P. Clinical features of Ota's naevus in Koreans and its treatment with Q-switched alexandrite laser. Clin Exp Dermatol. 2000;25(4):269-273.
10. Ueda S, Isoda M, Imayama S. Response of naevus of Ota to Q-switched ruby laser treatment according to lesion colour. Br J Dermatol. 2000;142(1):77-83.
11. Lam A, Wong D, Lam L, Ho W, Chan H. A Retrospective Study on the Efficacy and Complications of Q-Switched Alexandrite Laser in the Treatment of Acquired Bilateral Nevus of Ota-Like Macules. Dermatol Surg. 2001;27(11):937-42.
12. Chan HH, King WW, Chan ES, Mok CO, Ho WS, Van Krevel C, et al. In vivo trial comparing pacients tolerance of Q-switched neodymium:yttriumaluminum-garnet (QS Nd:YAG) lasers in the treatment of nevus of Ota. Lasers Surg Med. 1999;24(1):819-24.
13. Tse Y, Levine VJ, McClain SA, Ashinoff R. The removal of cutaneous pigmented lesions with the Q-switched neodymium:yttrium-aluminiumgarnet laser. J Dermatol Surg Oncol. 1994;20(12):795-800.
14. Moody MN, Landau JM, Vergilis-Kalner IJ, Goldberg LH, Marquez D, Friedman PM. 1,064-nm Q-Switched Neodymium-Doped Yttrium Aluminum Garnet Laser and 1,550-nm Fractionated Erbium-Doped Fiber Laser for the Treatment of Nevus of Ota in Fitzpatrick Skin Type IV. Dermatol Surg. 2011;37(8):1163-7.
15. Geronemus RG. Q-switched ruby laser therapy of nevus of Ota. Arch Dermatol. 1992;128(12):1618-22.
16. Chan HH, Kono T. Nevus of Ota: clinical aspects and management. Skinmed. 2003;2(2):89-96.
17. Hague JS, Lanigan SW. Laser treatment of pigmented lesions in clinical practice: a retrospective case series and patient satisfaction survey. Clin Exp Dermatol. 2008; 33(2):139-41.
18. Landau JM. Treatment of Nevus of Ota in Fitzpatrick Skin Type VI With the 1064 nm QS Nd:Yag Laser. Lasers Surg Med. 2011;43(2):65-7.
19. Ee HL, Goh CL, Khoo LS, Chan ES, Ang P. Treatment of Acquired Bilateral Nevus of Ota-Like Macules (Hori's Nevus) with a Combination of the 532 nm Q-Switched Nd:YAG Laser Followed by the 1,064 nm Q-Switched Nd:YAG Is More Effective: Prospective Study. Dermatol Surg. 2006;32(1):34-40.
20. Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, et al. Editors. Fitzpatrick's tratado de dermatologia. 5 ed. Rio de Janeiro: Revinter; 2005.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}