


Elisete Isabel Crocco1; Nicole Matos Costa2
Fractional photothermolysis was developed as an alternative to ablative lasers (which are effective but pose a high risk of complications) and non-ablative lasers (which have limited effectiveness). Fractional photothermolysis has been successfully used in diverse dermatological conditions. This study describes the case of an Asian male patient with atrophic scarring secondary to trauma in the left paranasal region, who underwent treatment with 1,550 nm non-ablative fractional Erbium Glass laser, which led to a significant improvement in the lesion. This case corroborates the use of less-invasive procedures in difficult-to-treat dermatoses and in treating Asian skin types safely and effectively.
Keywords: LASERS; THERAPEUTICS; CICATRIX; ATROPHY.
Fractional photothermolysis was introduced in 2003 as an alternative to ablative laser treatments (which are effective but have a high risk of complications) and non-ablative lasers treatments (which have limited effectiveness).1
Erbium fractional lasers target the water and emit beams that cause small tri- dimensional areas of thermal damage, called thermal microzones (TMZ). The surrounding tissue is not involved, enabling migration of viable keratinocytes and faster healing of coagulated tissue, with the homogenization of the dermal matrix and extrusion of microscopic epidermal necrotic debris. The stratum corneum remains functionally intact above the lesion column. This tissular repair mechanism decreases discomfort, the risk of infection, and patient recovery time. 2,3
The Erbium fractional laser has been used safely and effectively in various dermatological conditions including dyschromia, poikiloderma of Civatte, rhytids, photoaging, acne scars and surgical scars. 4
Atrophic scars are dermal depressions most commonly caused by collagen destruction that occurs with inflammatory skin diseases, such as cystic nodular acne or chickenpox, or after trauma, burns, and surgery. Scars of this type are difficult to treat, and usually require corrective surgery. Recently, less-invasive treatments have been used with relative success.5
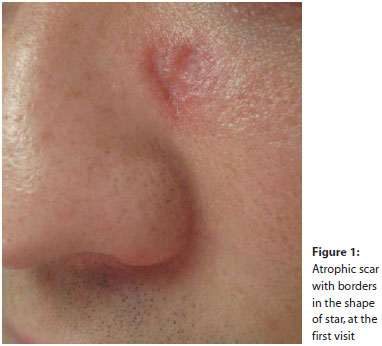
A 33-year-old businessman of Asian origin, with Fitzpatrick skin type IV, had developed a scar in the left paranasal region following an insect bite a month-and-a-half prior. Initially, there was local pruritus and exulceration, when Trofodermin® was used until the wound healed. The patient denied previous treatments. Physical examination revealed skin lesion located in the left paranasal region, characterized by an erythematous depressed area of approximately 0.6 cm in diameter, and surrounded by slightly elevated borders in the shape of a star (Figure 1).
The diagnostic hypothesis of atrophic scarring secondary to trauma was chosen, and a biopsy of the lesion was carried out in order to exclude other diagnoses. Histopathological examination evidenced chronic perivascular and periannexal dermatitis, without signs of malignancy. Fungi research came out negative. The result was consistent with the initial diagnosis, and the treatment with non-ablative fractional 1,550nm Erbium Glass laser (Mosaic of HP Lutronic®) was proposed.
Before each laser session, topical anesthesia (4% lidocaine cream, Dermomax®) was used at the site to be treated. Four laser sessions were carried out (at 30-day intervals) with the following parameters: 6x10mm tip, Static mode, 40J/cm2fluence, 100TMZ/cm2 density in the first session (and 200MTZ/cm2 in the others), with eight passes at each session. The patient used Skimatix® and 50 SPF sunscreen during the intervals between visits.
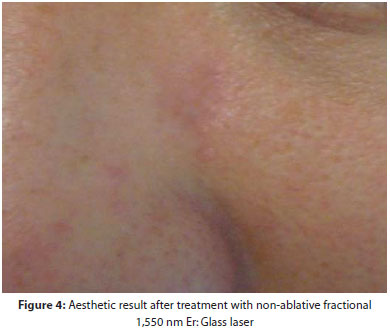
At the end of the four sessions, the patient experienced significant improvement of the lesion, which no longer had a raised surface. Only post-inflammatory hyperpigmentation was observed at the scar's site (Figure 2).
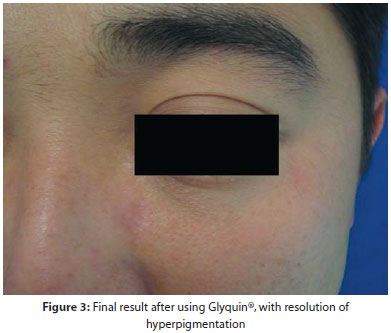
The patient was instructed to use Glyquin® nightly for a month, on alternate days, in addition to sunscreen. There was resolution of the hyperpigmentation, with excellent aesthetic results (Figures 3-4).
The non-ablative fractional 1,550nm Er:Glass laser has proved to be a fast, safe, effective, and non-invasive treatment of atrophic scars, and additionally, does not lead to the loss of facial volume at the scar site.
Because the laser pulse energy is proportional to the TMZ' depth, high energy levels lead to deeper tissue coagulation and dermal remodeling, which is desirable for the treatment of atrophic scars.
Non-ablative fractional lasers have been studied for the treatment of acne scars and atrophic scars in patients with Asian skin types. One of the most common side effects of laser treatment in pigmented skin is post-inflammatory hyperpigmentation. The pulse's density is a critical factor in the development of that complication. In severe cases however, it is necessary to use high-density pulses depending on the desired result. 1,5,6
As compared to ablative resurfacing, fractional photothermolysis creates localized islands of thermal injury, which are associated with a lower incidence of post-inflammatory hyperpigmentation. Furthermore, the 1,550nm wavelength has water as its main chromophore (without significant absorption by melanin) thereby reducing the risk of pigment disturbance, especially in patients with dark skin. 7
The present case report corroborates the use of less-invasive treatments, such as non-ablative fractional lasers, in difficultto-treat dermatoses and in treating Asian skin types safely and effectively.
1. Chan NP, Ho SG, Yeung CK, Shek SY, Chan HH. The use of non-ablative fractional resurfacing in Asian acne scar patients. Lasers Surg Med. 2010;42(10):710-5.
2. Osório NEGS, Torezan LAR, Niwa ABM, Nascimento DIS. Procedimentos associados à luz. In: Belda Jr W, Chiacchio N, Criado PR. Tratado de Dermatologia. São Paulo: Ed. Atheneu; 2010. p. 2: 2511-38.
3. Bogdan Allemann I, Kaufman J. Fractional photothermolysis-an update. Lasers Med Sci. 2010;25(1):137-44.
4. Sherling M, Friedman PM, Adrian R, Burns AJ, Conn H, Fitzpatrick R, et al. Consensus recommendations on the use of an erbium-doped 1,550-nm fractionated laser and its applications in dermatologic laser surgery. Dermatol Surg. 2010;36(4):461-9.
5. Park GH, Rhee DY, Bak H, Chang SE, Lee MW, Choi JH, et al. Treatment of atrophic scars with fractional photothermolysis: short-term follow-up. J Dermatolog Treat. 2011;22(1):43-8.
6. Cho SB, Lee SJ, Cho S, Oh SH, Chung WS, Kang JM, et al. Non-ablative 1550-nm erbium-glass and ablative 10 600-nm carbon dioxide fractional lasers for acne scars: a randomized split-face study with blinded response evaluation. J Eur Acad Dermatol Venereol. 2010;24(8):921-5.
7. Alajlan AM, Alsuwaidan SN. Acne scars in ethnic skin treated with both non-ablative fractional 1,550 nm and ablative fractional CO2 lasers: comparative retrospective analysis with recommended guidelines. Lasers Surg Med. 2011;43(8):787-91.
This study was carried out at the Santa Casa de Misericórdia de São Paulo (ISCMSP) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}