


José Roberto Pegas1; Karine Valentim Cade2; Michelle Yoko Kiyomura3; Aline Soares de Sousa3; Iracema Lerianna Mayer de Souza Bazzo2; Antônio José Tebcherani4
Summary: Acquired digital fibrokeratoma is a rare benign fibroepithelial condition, which typically occurs as a solitary asymptomatic nodule in fingers and toes. The authors report the clinical case of a female patient affected by two digital fibrokeratomas in the 4th and 2nd left fingers, respectively.
Keywords: NEOPLASMS, FIBROEPITHELIAL; FIBROMA; FINGER INJURIES.
Acquired digital fibrokeratoma (ADF) is a benign, fibrous tissue tumor that was first described by Bart et al. in 1968.1 Its etiology is still unknown, with trauma being regarded as the most important predisposing factor. ADF usually presents as a single, smooth, asymptomatic, fingerlike monochromic nodule, that can be sessile or pedunculated. An important differential clinical sign is the presence of a collarette at the base of the lesion. ADF tumors do not undergo spontaneous regression, and are more common in adults.2
Diagnosis is carried out through histology in all cases, and is characterized by orthokeratosis, acanthosis and hyperkeratosis. Surgical excision is the treatment of choice. 3,4
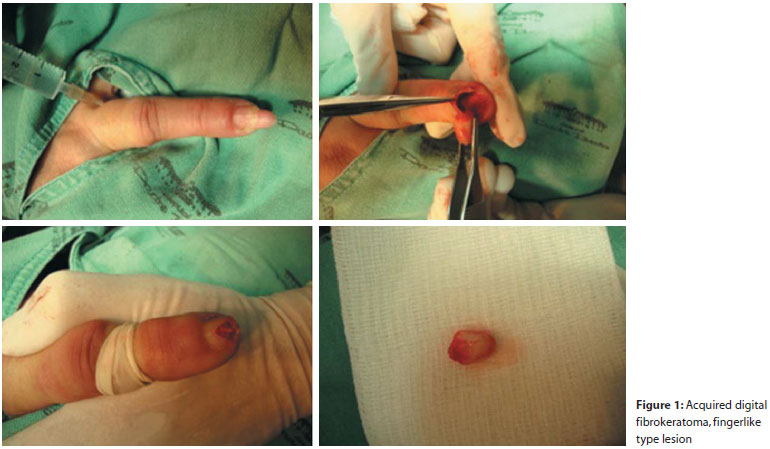
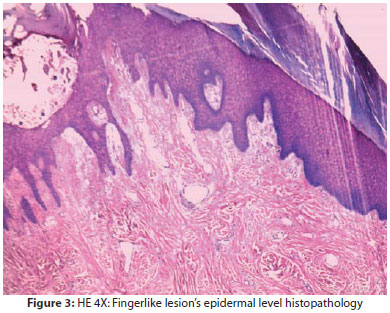
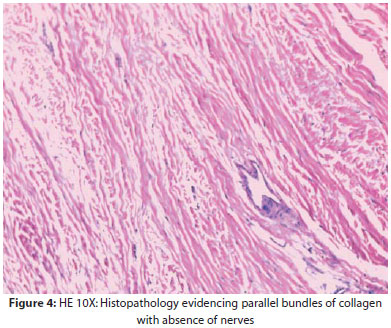
A 52-year-old female patient with a history of diabetes mellitus, hypertension, and dyslipidaemia reported asymptomatic lesions in the fourth left finger for seven years and in the second left finger for a year. No correlation with trauma was described. Physical examination evidenced two elongated hornlike lesions of different dimensions. The lesion located on the fourth left finger measured 1.0 x 0.8 x 0.8 cm. The second tumor (second left finger), measured 0.3 x 0.2 x 0.1 cm. Both were located in the hyponychium, emerging distally, in the shape of a finger (fingerlike) (Figure 1). After dermatological examination, the following diagnostic hypotheses were considered: supernumerary finger, Köenen’s tumor, verruca vulgaris (common wart), cutaneous horn, fibroma, and acquired digital fibrokeratoma. The patient was referred for surgical excision of the lesions (Figure 2), at which time a subsequent histological examination revealed a fingerlike type lesion (Figure 3), covered by an epidermis, with parallel collagen bundles observed in the stroma and an absence of nerve bundles with blood vessels (Figure 4).
This kind of tumor predominantly affects adult males over 40 years of age. It develops in the distal extremities, especially in fingers and toes, and can also occur on the lower lip, nose, elbow, pre-patellar region, nail bed, and heels.
With some exceptions, most cases reported in the literature describe lesions that are less than a centimeter long.5 According to Baykal et al., despite the scarcity of cases reported in medical literature, the frequency of ADF may be underestimated due to the fact that that tumor resembles many benign lesions that usually do not require routine histopathological examination.6
All extremity tumors that present elongated ends in the shape of projectiles (fingerlike), should be considered for ADF during a differential diagnosis. Other possible diagnoses are: supernumerary finger, common wart, cutaneous horn, pyogenic granuloma, Köenen’s tumor, soft fibroma, neurofibroma and eccrine poroma.5,6
A supernumerary finger, also called polydactyly, is described as a congenital lesion usually located at the base of the fifth finger, with a histopathology suggesting abundant nerve bundles.
In turn, the common wart often displays a roughened surface. Both the common wart and the supernumerary finger have an epidermal collarette, which is also seen in ADF.
A Köenen's tumor can be difficult to differentiate histopathologically and can be considered a variant of the disease because it often presents a small distal segment, with loose collagen, several blood vessels, and a large proximal portion consisting of dense collagen bands and few capillaries. A Köenen's tumor is a lesion characteristic of tuberous sclerosis: not arising before puberty, emerging from the nail folds, being usually multiple and of pinkish or skin color, and located predominantly on the feet.
As with ADF, pyogenic granuloma presents with an epidermal collarette, however it is usually more friable and onsets suddenly. The cutaneous horn has a rough or warty surface, and has its main differential diagnosis in histopathology.2,6 Fibrokeratomas are benign fibroepithelial tumors marked by hyperkeratosis and acanthosis. The dermis is filled with thick collagen bundles occurring parallel to the tumor’s axis. Elastic fibers will be thin, and while sparse, not completely absent and often very vascularized. 4,7
Kint et al. described three histological types: "dome shaped" lesion with elastic fibers and numerous dermal capillaries (Type I); particularly high and hyperkeratotic lesion with many fibroblasts and few elastic fibers (Type II); edematous lesion that alternates between a flat and “dome” reliefs, with few cells and no elastic fibers (Type III).8 The present case was compatible with Type I.
Surgical treatment leads to healing in most cases, and recurrence is rare (Figures 3 to 4).
The present case emphasizes the importance of this benign tumors’ categorization – with fingerlike format – since it can be easily misdiagnosed for other common tumors during differential diagnosis. The present case has also shown the rare occurrence of the same kind of lesion arising in two different fingers.
1. Bart RS, Andrade R, Kopf AW, Leider M. Acquired digital fibrokeratomas. Arch Dermatol. 1968;97(2):120-9.
2. Berger RS, Spielvogel RL. Dermal papule on a distal digit. Acquired digital fibrokeratoma. Arch Dermatol. 1988;124(10):1559-60;1562-3.
3. Frydman AF, Mercer SE, Kleinerman R, Yanofsky VR, Birge MB. Acquired fibrokeratoma presenting as multiple plantar nodules. Dermatol Online J. 2010;16(10):5.
4. Lee DR, Lee JY, Ahn JY, Park MY. A case of acquired digtalfibrokeratoma accompanied by pyogenic granuloma. Dermatol Online J. 2009;15(1):8.
5. Choi JH, Jung SY, Chun JS, Seo JK, Le D. Giant Acquired digtalfibrokeratoma occurring on the left great toe. Ann Dermatol. 2011;23(1):64-6.
6. Baykal C, Buyukbabani N, Yazganoglu D, Saglik E. Acquired digtalfibrokeratoma. Cutis. 2007;79(2):129-32 .
7. Freitas PM, Chavier MHSB, Pereira GB, Rochael MC, Cortes JLO, Quevedo LP, et al. Acquired fibrokeratoma presenting as a giant pedunculatedlesiono n the heel. Dermatol Online J. 2008;14(12):10.
8. Kint A, Baran R, De Keyser H. Acquired (digital) fibrokeratoma. J Am Acad Dermatol.1985;12(5 pt 1):816-21.
This study was carried out at the Complexo Hospitalar Padre Bento de Guarulhos – Guarulhos (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}