


Natália Marques Franco1; Luciena Cegatto Martins Ortigosa2
The keratoacanthoma is a fast growing benign skin tumor that is composed of squamous cells and has clinical and histopathological features similar to those of the squamous cell carcinoma, and may undergo spontaneous regression without any treatment. It mainly affects elderly and immunosuppressed males who have fair skin, occuring in body sites that have been chronically exposed to sunlight, such as the face, forearms and backs of hands. The differential diagnosis with squamous cell carcinoma is particularly important. The recommended treatment is its surgical excision. Other treatment modalities, such as cryotherapy, electrocoagulation and intralesional injection of chemotherapeutic agents, are also available.
Keywords: KERATOACANTHOMA; LASER THERAPY; SKIN.
Intense pulsed light (IPL) is a non-ablative technology that employs light for various applications. IPL systems are high intensity pulsed sources that emit polychromatic light in a broad spectrum of wavelengths, between 515 and 1,200nm.1.2 These sources generate heat in the skin, reaching targets such as melanin and blood vessels, allowing the correction of various pigmented lesions and stimulating collagen production by dermal fibroblasts. Through the dissipation of energy, it acts on various chromophores in a process that promotes non-coherent tissue renewal through intense filtered light, based on the principle of selective photothermolysis.3
The use of lasers and IPL can cause several complications. Among the slight complications possible are prolonged erythema, acne, millia, purpura, superficial erosions and contact dermatitis. Among moderate complications are infections, altered pigmentation (such as hyper and hypocromias), toxicity due to the use of topical anesthetic and keratoacanthomas (KA). Severe complications include hypertrophic scarring, disseminated infection, and ectropion formation, among others.
The development of a KA following the use of IPL is described in the present study.
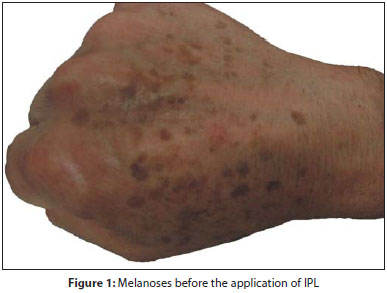
A Caucasian, 59-year-old physician male patient sought care at the Dermatology Service of the Faculdade de Medicina de Presidente Prudente (Unoeste) – Presidente Prudente (SP), Brazil, in July 2011 hoping to improve the appearance of his hands. The dermatologic examination suggested the patient had Fitzpatrick Phototype I and hyperpigmented brownish patches, ranging from light to dark hues, on the back of the hands, a feature characteristic of solar melanoses (Figure 1). The patient underwent an IPL session with the equipment Harmony® (Alma Lasers, Caesarea, Israel), using a 540nm filter, program 12, energy at 18J/cm2, which resulted in improvement of the lesions' appearance. Three weeks later, however, a pinkish papule with regular borders, and smooth surface, with a crusted and hardened mass in the center emerged on the dorsum of the right hand (Figure 2).
Due to the presence of symptoms suggestive of KA following IPL, the differential diagnosis for squamous cell carcinoma (SCC) through histology was not necessary.
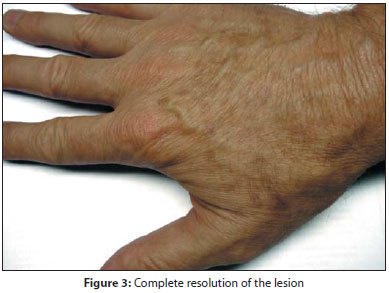
The patient was treated topically with topical 5% imiquimod three times per week for eight weeks. There was complete resolution of the lesion after three months (Figure 3). The patient was satisfied with the aesthetic result achieved.
KA is a common, fast-growing benign skin tumor with histological features similar to those of the squamous cell carcinoma (SCC), with a tendency to spontaneous regression.5 It is more frequent in fair-skinned adults between 55- and 65-years old, and rarely occurs in African or Asian descendent patients. It affects both genders equally, with a slightly higher incidence in men.5 It has a higher incidence in the elderly and immunocompromised patients.6
Many factors are involved in its development. The chronic exposure to ultraviolet radiation plays an important role, which is demonstrated by the higher occurrence in areas exposed to the sun. Among other causes are the HPV virus, chemical carcinogens, mechanical trauma, association with other skin diseases and genetic factors.5
Little is known about the KA's pathogenesis and the exact mechanism of regression of the lesion in the absence of any treatment. Studies have revealed the presence of the expression of the p53 oncoprotein in most cases, suggesting a possible role of that gene in the development of KA.5
Characteristically, it presents a lesion that grows in a few weeks, followed by slow involution during a period that varies from two to six months. The proliferative phase is characterized by the formation of a firm papule with erythematous or pigmented border, that grows over a period of two to six weeks, reaching about 2cm in diameter. The lesion is most frequently diagnosed during its maturation phase, which presents as an erythematous nodule with a keratin central area. Its resolution is characterized by the expulsion of keratin, leaving a hypopigmented scar.5
KA's histology depends on the stage of the tumor. Its characteristic architecture includes hyperkeratosis and acanthosis, atypical cells and mitoses figures. Inflammatory infiltrate may be present due to necrosis of keratinocytes.5 The differential diagnosis with SCC is key: KA is a rounded tumor composed primarily of well-differentiated squamous epithelium with little pleomorphism and a strong tendency to form keratin. It presents with epithelial infiltration, smooth, regular and well-defined surface. On the other hand, SCC presents greater anaplasia and keratin production is scarce or absent.5
Only a few KA patients have impaired humoral or cellular immunity. Some KAs present changes in Class II HLA antigens. The role of immunity in spontaneous regression has been researched, with the appearance of an erythematous halo around some KAs in regression being clinically observed. Histology shows a dense mononuclear infiltrate and fibroblastic reaction in the site, with the presence of Langerhans cells and the detection of anti-squamous cells antibody associated with the regression.6 There is, however, increasing evidence that it is not immunologically mediated, implying similarity to the pattern of natural regression seen within the normal hair follicle.6
Regression of KA can happen spontaneously, nevertheless it would cause an aesthetically undesirable scar. Therefore, the treatment must be initiated as soon as possible, with complete surgical excision recommended in most cases.5
Other forms of treatment include cryotherapy, electrocoagulation and intralesional injection of chemotherapeutic agents (methotrexate, bleomycin, 5-fluorouracil, interferon-alpha and triamcinolone). Radiotherapy is indicated for lesions of difficult surgical access.5
Systemic treatment includes retinoids, methotrexate, cyclophosphamide or 5-fluorouracil.5 Photodynamic therapy with aminolevulinic acid presents good therapeutic and aesthetic results.5
Topical imiquimod, an immunomodulator belonging in the agonist receptors 7 and 8 group, is effective. Four to 11 weeks of use are necessary, with side effects possible as a result of inflammation from an immune response (e.g. burning sensation, erythema, and erosions).7 The time required for the complete clinical resolution may be longer than that required for the histological remission, because the imiquimod-induced inflammation can hamper the physician's capacity to judge the clinical cure.7
After review of the literature, three KA cases associated with laser therapy were found: 4 one with eruptive KAs in the face two months after facial rejuvenation treatment with CO2 laser, 8 with the other two cases occurring in the legs, following fractional photothermolysis with 1,550nm laser (Fraxel). 9 Some authors speculate that trauma on the follicular unit during the treatment may induce tumors, however that hypothesis is not yet fully clarified.4
The case described in the present study differs from previous ones due to the fact that it is an isolated KA, which has not yet been described in association with IPL applied to the hands. The authors have chosen to use topical imiquimod in an attempt to prevent scarring at the site, since the patient was initially looking for a cosmetic procedure. The authors believe that imiquimod is effective and can be used safely when correctly applied by well-oriented patients who return for follow up visits.
The correct handling of the various techniques used in dermatology is of paramount importance and, in addition to the proper use and experience in dealing with devices, physicians must be able to diagnose and treat possible complications. Providing previous guidance and obtaining patient consent before performing any procedure is critical. Likewise, monitoring the development of the lesion during the treatment and after it, with follow-up visits to assess the results, are essential for early detection of possible complications.
1. Patriota RCR. Laser um aliado na dermatologia. Rev Med (São Paulo). 2007; 86(2):64-70.
2. Catorze MG. Laser: fundamentos e indicações em dermatologia. Med Cutan Iber Lat Am. 2009;37(1):5-27.
3. Issa MCA, Manela-Azulay M. Terapia fotodinâmica: revisão da literatura e documentação iconográfica. An Bras Dermatol.2010;85(4):.501-11.
4. Metelitsa AI, Alster TS. Fractionated laser skin resurfacing treatment complications: a re-view. Dermatol Surg. 2010;36(3):299.
5. Cerroni L, Kerl H. Keratoacanthoma. In: Goldsmith LA, Katz SI, Gilcherest BA, Paller AS, Leffel DJ, eds. Fitzpatrick`s Dermatology in General Medicine. 7th ed. New York: Mc Graw Hill; 2008. Cap. 117. p. 1050-2.
6. Schwartz RA. Keratoacanthoma. J Am Acad Dermatol. 1994;30(1):1-22.
7. Jeon HC, Choi M, Paik SH, Ahn CH MD, Park HS, Cho KH. Treatment of Keratoacanthoma with 5% Imi-quimod Cream and Review of the Previous Report. Ann Dermatol. 2011;23(3): 357-61.
8. Gewirtzman A, Meirson DH, Rabinovitz H. Eruptive keratoacanthomas following carbon dioxide laser resurfacing. Dermatol Surg 1999;25(8):666-8.
9. Mamelak AJ, Goldberg LH, Marquez D, Hosler GA, Hinckley MR, Friedman PM. Eruptive keratoacanthomas on the legs after fractional photothermolysis: report of two cases. Dermatol Surg 2009;35(3):513-8.
This study was carried out at the Faculdade de Medicina de Presidente Prudente (Unoeste) – Presidente Prudente (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}