


Joaquim José Teixeira de Mesquista Filho1; Fernanda Campany2
This study describes a technique for correcting entropion based on the case of a female patient who had that alteration in the left lower eyelid, in addition to sagging and fat pseudo-herniation in the left and right eyelid areas. Bilateral upper and lower blepharoplasty was performed, with wedge resection of the orbicularis muscle and tarsus in both lower eyelids, followed by reconstruction. The patient presented good functional and aesthetic results, with no complications.
Keywords: BLEPHAROPLASTY; ENTROPION; RECONSTRUCTION.
Entropion is a senile disorder in which the eyelid turns in toward the eyeball, which can cause irritation, tearing, hyperemia and even corneal ulcers and scarring.1
It is associated with horizontal eyelid laxity, which is caused by the weakening and laxity of the orbicularis muscle, tarsus and chantal ligaments, or by the detachment of the capsulopalpebral fascia.1-3
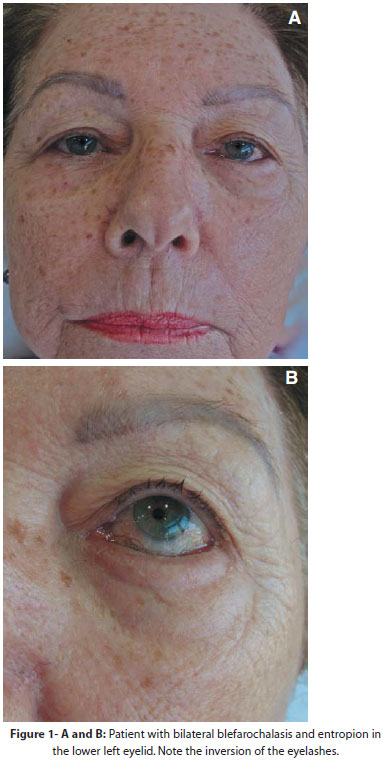
A seventy-six-year-old female patient with sagging and excess skin in the upper and lower eyelid regions. She also presented inversion of eyelashes towards the eyeball (entropion) in the left lower eyelid, causing hyperemia, irritation and great local discomfort (Figure 1).
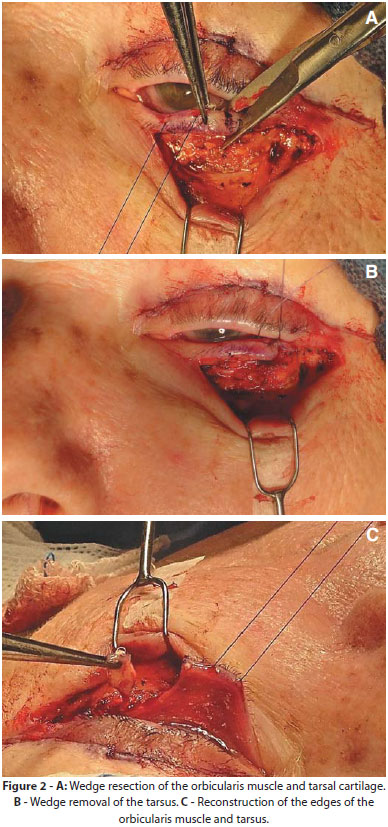
Following local anesthesia, the excision of the lower eyelids's skin was performed along the ciliary margin, with the visualization of the orbicularis muscle. For the correction of the entropion, the wedge excisionwas carried out with an iris scissors, encompassing the orbicularis muscle and tarsus, exposing the eyeball. After hemostasis, the repositioning and reconstruction of the palpebral border was carried out withsimple suture of the muscle and tarsal borders in multiple levels, using 6.0 Vicryl absorbable sutures (Figure 2). The last stage of the surgery consists of the excision of the lower eyelids' excess skin and the suture with 6.0 nylon thread. The patient also underwent upper blepharoplasty during the procedure.
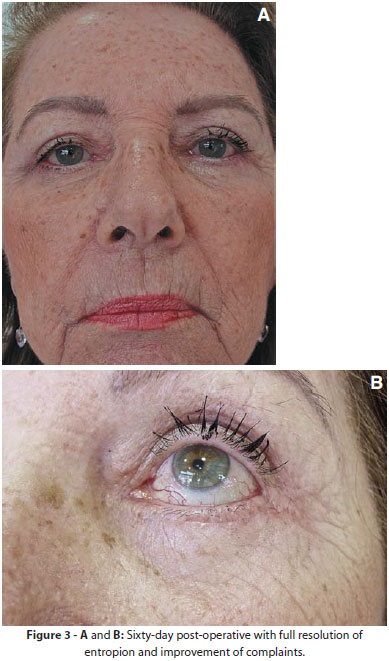
The suture was removed after seven days with absence of complications in the post-operative period. There was a good aesthetic result two months after the surgery, with the maintainance of the correct eyelid position and absence of irritative symptoms in the eyeball (Figure 3). Follow up visits are carried out every six months.
Senile entropion occurs in individuals older than 60, being more frequent in women, possibly due to the relatively smaller size of the tarsal plate in women. The lower eyelids are most affected, usually with complete involvement of the eyelid margin.3
Surgery is the only effective and definitive treatment.2 Thorough knowledge of eyelid anatomy is essential to determine the etiology and carry out the surgical intervention of the lower eyelid abnormalities.
The eyelid is divided into an anterior and a posterior lamella. The anterior lamella consists of skin and orbicularis muscle. The posterior lamella consists of the rectractor eyelid system, tarsusand conjunctiva. The first is the fascia that splits to encapsulate the inferior oblique muscle and then re-joins to form the dense fibrous sheet (fascia capsulopalpebral),4 which inserts in the lower edge of the tarsal plate. The failure of this fascia to insert in the lower eyelid's tarsus commonly causes instability in the rotation movement and entropion.5
The tarsal plates are composed of dense connective tissue. The lower eyelid's tarsus is 4-5mm high 16-20mm long and 1mm thick. They are anchored medially and laterally to the orbital rim by cathal tendons. The posterior surface is covered by densely adherent conjunctiva.5
Senile entropion is caused mainly from muscle and tarsal laxity and sagging, causing the edge of the eyelid to lose its correct positioning. Performing the resection of the lower eyelid's muscle band causes the horizontal shortening of the orbicularis muscle and tarsus, lending them more firmness and allowing their return to the correct position.2
The most common complications in the post-operative period are hematomas and, less frequently, ectropion, dehiscence and recurrence of entropion, with the possibility of further surgery.2
Based on the main causes of the condition, the procedure was demonstrated to be a simple, safe and effective option, yielding good functional and aesthetic result for the treatment of the senile entropion.
1. Fonseca Junior NL, Lucci LMD, Rehder JRCL. A importância da enoftalmia senil no desenvolvimento do entrópio involucional. Arq Bras Oftalmol. 2007;70(1):63-6.
2. Morano FG, Amâncio Jr M, Brejon R, Esper CR, Farias JCM. Entrópio senil da pálpebra inferior: cirurgia baseada na etiopatogenia. Rev Bras Cir Plast. 2010;25(2):231-7.
3. Bashour M, Harvey J. Causes of involutional ectropion and entropion age related tarsal changes are the key. Ophthal Plast Reconstr Surg. 2000;16(2):131-41.
4. Dryden RM, Leibsohn J, Wobig J. Senile entropion. Pathogenesis and treatment. Arch Ophthalmo. 1978;96(10):1883-5.
5. Park SS, Little S. Reconstrução das pálpebras. In: Baker SR. Retalhos locais em reconstrução facial. 2.ed: Elsevier, 2009. p. 390-3.
This study was carried out at the Instituto de Dermatologia Professor Rubem D. Azulay of the Santa Casa de Misericórdia do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}