


David Oschilewski Lucares1; José Javier Rodriguez2; Andréia Leverone3; Robertha Carvalho de Nakamura4
Introduction: A poorly described aspect of onychocryptosis – the main cause for nail unit surgeries – is how to perform its surgical closure. The present article describes a new technique denominated alpha stitch that allows the straightening out of the nail fold by positioning it at or below the nail plate’s level.
Objective: To demonstrate the benefits of the alpha stitch surgical closure technique in the surgical matricectomy for onychocryptosis.
Methods: Twenty patients with onychocryptosis grades II and III underwent surgical matricectomy and were followed up for six months. The surgical closure was performed using the alpha stitch technique.
Results: A total of 27 lateral nail folds were operated, with 81.8% yielding the expected result, and 18.1% presenting uncertain outcomes.
Conclusions: The alpha stitch allows the proper healing of the straightened out nail fold, which is positioned at or below the nails plate’s level, with good results, fast recovery, minimal morbidity and a small number of recurrences. The technique can also be used in surgical procedures involving other nail disorders.
Keywords: NAIL DISEASES; AMBULATORY SURGICAL PROCEDURES; SURGICAL PROCEDURES, MINOR; SUTURE TECHNIQUES.
Subcutaneous onychocryptosis is one of the most common diseases of the nail unit, having a high morbidity rate and a disabling clinical picture. It is more prevalent in adolescents and young male adults, at a ratio of 3:1.1-4 Several factors determine this condition: heredity, constitution, disproportionate nail plate and nail bed widths, and increased transverse curvature of the nail plate. Other additional aggravating factors are: medial deviation of the hallux, thinning of the nail plate, periungual tissue thickening, hyperhidrosis of the feet, convex cut of the free distal fold of the nail plate, and the wearing of pointed or excessively tight shoes.1-5
The clinical picture, classified by Heifetz according to the degree of severity, is characterized by the presence of inflammatory signs such as erythema, mild edema, and pain caused by pressure on the lateral nail fold (Grade I onychocryptosis). These symptoms are caused when a nail plate with an inward pointing lateral spike advances into the periungual tissue, triggering an inflammatory reaction.
If the injury persists, inflammatory reactions increase, possibly leading to the emergence of exudate, secondary infection, and local drainage (Grade II onychocryptosis). If the process continues further, the symptoms intensify, with the formation of granulation tissue and hypertrophy of the lateral nail fold (Grade III onychocryptosis).1-6
Diagnosis is mainly clinical, with imaging-based analysis being necessary when there is a suspicion of bone alteration or local infection. X-ray examination is an inexpensive and effective way to screen for bone alterations. Infectious alterations become apparent through X-rays only when 50-60% of the bone in the vertebral body is destroyed, therefore it shows as normal during the initial infection period. Bone scintigraphy is effective for observing osseous remodeling. The most sensitive and specific imaging study for the detection of infections is the MRI.7-9
The therapeutic approach can be carried out in two ways: conservative and surgical. For Grade I, the guidance is to follow a conservative approach, with different treatment modalities available.7-16 On the other hand, for Grades II and III, the alternative that yields the best outcomes is the surgical approach.3-5 The more frequently used techniques are surgical matricectomy (surgical excision of the lateral matrix horn) and chemical matricectomy (phenolization). In the latter approach, healing takes place by secondary intention. In surgical matricectomy, the removal of the matrix is carried out after surgical incision of the proximal fold in order to remove the matrix horn, nail spike and/or to resect the lateral fold’s fibrosis (if present) aiming at normalizing the architecture of the affected area.3-5,17-30 In the latter approach, surgical closure is of paramount importance, and is the central subject of the present study.
How the surgical closure should be performed – often described with the use of simple stitches – is a poorly evaluated aspect in the treatment of onychocryptosis.17-30 The authors believe that the use of simple stitches has the disadvantage that the lateral nail fold heals in intimate contact with the nail plate, where local friction between the plate and the fold can precipitate a possible clinical recurrence. In order to address this issue, the authors developed a surgical closure technique denominated the alpha stitch. The goal is to position the lateral fold at the nail plate level or below it; in other words, to rectify the nail fold, obtaining healing and thus preventing recurrence.5
General research
The present paper details a prospective, descriptive study of a series of cases of patients diagnosed as having Grade III onychocryptosis, who underwent surgical matricectomy wherein surgical closure was performed through the alpha stitch. The patients were selected from among a group who had sought treatment spontaneously at the outpatient clinic of a center specializing in nails, and were later invited to participate in the study. In all cases authorization has been granted via the signing of a term of informed consent. The study was submitted for prior review of the Research Ethics Committee of the institution where the study was carried out.
Inclusion criteria were: patients of both genders, older than 21 years of age, diagnosed with Grade II onychocryptosis (due to the presence of a nail spike in the proximal region) and Grade III onychocryptosis (due to hypertrophy of the lateral fold). Patients who had the condition to a lesser degree, had a local infection requiring prior drainage, were allergic to the anesthetics provided, had coagulation disorders, hypertension, diabetes, or were pregnant, were excluded.
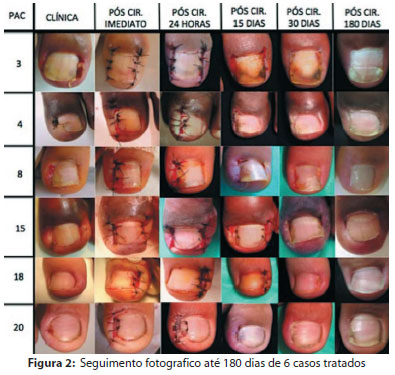
Clinical controls were carried out through photographic records before and immediately after the procedure, 24 hours after the procedure, and 15, 30 and 180 days after the surgery. Patients were instructed to keep their feet elevated on the days immediately after the surgery and were instructed in the use of analgesics and daily dressing with antibiotic cream. The stitches were removed on the 15th day of the post-operative period. Also, other clinical and epidemiological information was obtained through a specifically developed questionnaire. Data were tabulated in Microsoft Excel 2003, for further analysis.
Lateral surgical matricectomy technique:
• Patient in supine position, with knees bent
• Cleansing of the affected foot with povidone-iodine solution
• Sterile field preparation, exposing the affected toe
• Anesthetic nerve block
• Application of tourniquet at the base of the affected toe, for a bloodless operative field
• Removal of granulation tissue through elliptical incision in the affected lateral nail fold, from the proximal nail fold up to the anterior border, allowing better visualization of the underlying structures, and matrix horn and proximal nail spike. If there is hypertrophy of the lateral fold (Grade III onychocryptosis), excision of fibrosis is carried out
• Detachment of the lateral fold of the nail plate, from the free border to the lateral nail matrix
• Cutof the lateral plate, in a straight line directed to the nail matrix, surpassing the proximal fold, reaching the lateral matrix horn
• Attachment of the entire plate and nail matrix horn, already cut with long straight forceps, and subsequent rotation in a continuous circular motion until the incised nail plate and matrix horn breaks loose
• Curettage of the visible lateral nail bed, where the excess granulation tissue is located
Technique of surgical closure with alpha stitch:
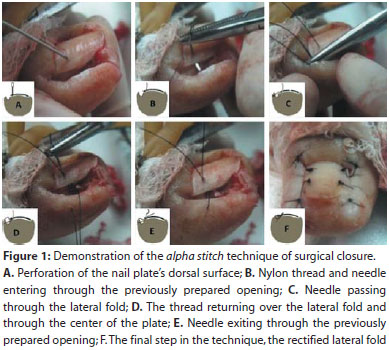
• Drilling of the dorsal surface of the nail plate with needle 21G, at 2-3mm from the lateral fold of the affected side, with rotational movements (Figure 1A)
• The 4.0 nylon threaded needle penetrates the previously prepared opening, passing between the nail bed and nail plate (the nail bed is not traumatized), coming out flush with the free border of the nail plate (Figure 1B)
• The needle crosses the lateral fold at 3-4mm from the free border of the fold (Figure 1C)
• The nylon thread returns over the lateral fold; the needle passes through the center of the nail plate (between the nail bed and the nail plate) (Figure 1D), exiting through the opening prepared at the beginning of the procedure (Figure 1E)
• After passing through the central orifice of the nail plate, the thread must by pulled in such a way as to approximate the free border of the lateral fold, positioning the latter at the nail plate level or below it, in a rectified manner
• Completion of the suture (Figure 1F). The final aspect resembles the letter alpha of the Greek alphabet
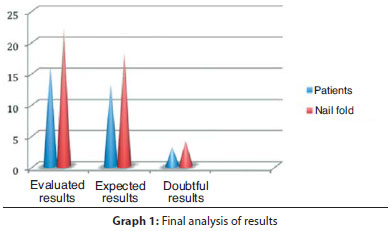
Twenty patients were included in the study, with 27 nail folds having undergone surgical closure with the alpha stitch technique. Four patients (five nail folds) did not return for the 180-day follow-up and were excluded from the final analysis of results. The final results evaluation, comprising 16 patients and 22 operated nail folds, was carried out six months after the end of the treatment. In the final analysis, 13 patients (18 operated nail folds) (81.8%) had results as expected (i.e. rectified nail fold, positioned at the level of or below the nail plate (Figure 2). In 3 patients (4 operated nail folds) (18.1%), results were less certain with the nail folds positioned at a higher level than that of the nail plate. The surgical procedure performed to resolve the onychocryptosis was successful in 100% of the cases (Graph 1).
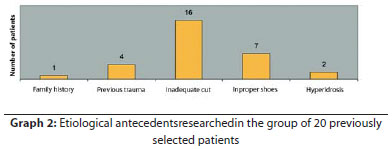
The gender distribution was 13 men and seven women. The patients’ age varied from 21 to 53 years (mean = 31.2 years). Twelve patients reported previous history of onychocryptosis (with 11 reporting it occurring at the same site). Ten patients had undergone previous treatment (5underwent conservative techniques, 3underwent surgical techniques, and 2underwent both). The details of the measures taken were unknown in most cases. Etiological antecedents were also investigated (Graph 2).
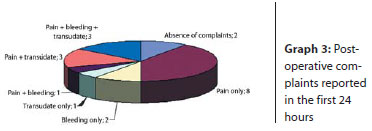
In the 24-hour post-operative control period, 18 of the 20 patients initially included in the study reported complaints. The distribution of patients according to the combinations of complaints described can be seen in Graph 3. The most common symptom was a mildly intense pain, which responded well to an analgesic.
No suture dehiscence was observed in the 15-day post-operative control; five patients still reported complaints during this timeframe. Two patients described pain, two were still experiencing transudate, and one described both symptoms – of mild intensity in all cases. There were no signs of active infection. In all cases it was possible to remove the stitches.
In the 30-day post-operative control period, only two patients reported complaints – one of pain and another of transudate, both mild. None of the patients required the use of analgesic medication. Also, no infection was observed and there was no need for antibiotics in the same period. All reported satisfaction with the aesthetic result of the treatment. The average time for the patients to return to their daily activities was 16.8 days.
One patient experienced recurrence six months after the procedure. Both corners of the patient’s toe were affected, with the recurrence located in one of the lateral folds. The patient admitted to having cut the nail convexly, having worn boots, and having not rested as instructed. (Figure 2)
Men were more frequently affected than women (approximate ratio of 2:1). Sixty percent of patients have reported a history of onychocryptosis, with 41% having had three or more episodes, corroborating the findings in the literature. 1-6,18,29
Regarding the study’s main objective, the authors believe that the proposal of rectifying the nail fold using the alpha stitch in surgical matricectomy, when treating Grade II and III onychocryptosis, was clearly demonstrated.
There was good control of post-operative symptoms, with minimal morbidity and excellent healing. Pain was the main symptom reported by patients, followed by transudate and bleeding. The pain was mild in most cases, with good response to the administration of a light analgesia (paracetamol). Eighty-five percent of patients used the medication for only one day, and a maximum of three days in two cases. Fifteen days after the surgery only five patients reported some complaints, always of mild intensity and without the need for medication. Thirty days after the surgery, only two patients reported symptoms: one pain and the other, transudate, both of mild intensity. Interestingly, those latter cases did not present symptoms in previous controls. This degree of morbidity after the procedure is consistent with several case series in the surgical matricectomy technique.18-21, 25, 27
Bleeding was reported in only six patients during the24-hourcontrol period. In the main reference literature, transudate is described as the primarypost-operative symptom, lasting from three to four weeks.1,4,6 The patients in the present case series did not report transudate as the main symptom. Seven patients had this symptom –mostly mild – on the day after the surgery (five 15 days after and only two 30 days after). This good result was due possibly to the surgical closure of the nail fold in a rectified manner, obtained with the alpha stitch – as the lateral fold is positioned at the levelof the nail plate or below it, exerting good compression and local hemostasis. Furthermore, there is no perforation of the nail bed. The stitch’s tension force may have also contributed to the good result, since there was no suture dehiscence in any case.
The average time that it took patients to return to normal activity was 16.8 days (varying between 7 and 25 days). This time frame is slightly shorter than that described by Bostanci et al., who performed matricectomy through phenolization (mean: 18.02 days).19
During the surgical procedure, the attention given for the complete removal of the lateral region of the nail matrix influenced the low recurrence rate, which was reported by only one patient after the study course (180 days), and moreover being caused due to induced factors (i.e. convex cut of the nail plate).
Recurrence is common after matricectomy, with incomplete removal of the lateral nail matrix being the main cause.29 All patients reported satisfaction with the surgery’s aesthetic outcome.
The authors believe that nail unit surgery should be treated with more precision due to its special anatomy and physiology. This includes such fundamental aspects as the implementation of a specific stitch for the onychocryptosis surgery. Using the alpha stitch for surgical closure allows the proper healing of the nail fold, by fixing its position at the level of or below the nail plate. This stitch technique produces good cosmetic results, faster recovery times, minimal morbidity, and a small number of recurrences.
The alpha stitch technique of surgical closure is simple and easy to learn, and can be easily incorporated into the dermatologist’s daily practice in the surgical treatment of onychocryptosis. It would also be possible to use it in surgical procedures to correct other nail disorders, such as lateral longitudinal biopsy and tumor excisions, suggesting that this closure technique has a promising future. The authors believe that the technique resulted in good outcomes in the present study, however due to the small sample size, further studies must be carried out to corroborate their findings.
1. Ignez MM, Azulay RD. Alteraciones ungueales. In: Azulay RD, Azulay DR, Azulay-Abulafia L. Dermatología. 4 ed. Rio de Janeiro: Editora Guanabara Koogan; 2006. p. 680-97.
2. Tosti A, Piraccini BM, Di Chiacchio N. Doenças das Unhas. São Paulo: Editora Luana; 2007.
3. Baran R, Dawber RPR. Diseases of the nail and their Management. 3rd edith. Oxford: Blackwell Scientific Publications; 2001. p. 492-506.
4. Baran R. Cirugía de la uñas. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick: Dermatología en Medicina General. 5 ed. Buenos Aires: Panamericana, 2005. p.2934-44.
5. Baran, R.; Nakamura, R.C. Doenças das unhas, do diagnóstico ao tratamento. Primeira edição, 2011. Elsevier editora ltda.; 58-65; 137-139.
6. Heifetz CJ. Ingrown toenail. A clinical study. Am J Surg. 1937; 38:298.
7. emedicine.com [homepage]. Ingrown nails, 2009 [acesso 13 Out 2009]. http://emedicine.medscape.com/article/909807-overview
8. Heidelbaugh JJ, Lee H. Management of the ingrown toenail. Am Fam Physician. 2009; 15;79(4):303-8.
9. Termaat MF, Raijmakers PG, Scholten HJ, Bakker FC, Patka P, Haarman HJ. The Accuracy of Diagnostic Imaging for the Assessment of Chronic Osteomyelitis: A Systematic Review and Meta-Analysis. J Bone Joint Surg Am. 2005; 87(11):2464-71.
10. Senapati A. Conservative outpatient management of ingrowing toenails. J R Soc Med. 1986; 79(6):339-40.
11. Nazari S. A simple and practical method in treatment of ingrown nails: splinting by flexible tube. J Eur Acad Dermatol Venereol. 2006;20(10):1302-6.
12. Kim YJ, Ko JH, Choi KC, Lee CG, Lim KJ. Nail-splinting technique for ingrown nails: the therapeutic effects and the proper removal time of the splint. Dermatol Surg. 2003;29(7):745-8.
13. Gupta S, Sahoo B, Kumar B. Treating ingrown toenails by nail splinting with a flexible tube: an Indian experience. J Dermatol. 2001;28(9):485-9.
14. Erdogan FG. A simple, pain-free treatment for ingrown toenails complicated with granulation tissue. Dermatol Surg. 2006;32(11):1388-90.
15. Arai H, Arai T, Nakajima H, Haneke E. Formable acrylic treatment for ingrowing nail with gutter splint and sculptured nail. Int J Dermatol. 2004;43(10):759-65.
16. Ishibashi M, Tabata N, Suetake T, Omori T, Sutou Y, Kainuma R, et al. A simple method to treat an ingrowing toenail with a shape-memory alloy device. J Dermatolog Treat. 2008; 19(5):291-2.
17. Rounding C, Bloomfield S. Surgical treatments for ingrowing toenails. Cochrane Database Syst Rev. 2005; 18(2):CD001541.
18. Zuber TJ. Ingrown toenail removal. Am Fam Physician. 2002;65(12):2547-52, 2554.
19. Bostanci S, Ekmekçi P, Gürgey E. Chemical matricectomy with phenol for the treatment of ingrowing toenail: a review of the literature and follow-up of 172 treated patients. Acta Derm Venereol. 2001;81(3):181-3.
20. Cameron PF. Ingrowing toenails: an evaluation of two treatments. Br Med J (Clin Res Ed). 1981;283(6295):821-2.
21. Andreassi A, Grimaldi L, D'Aniello C, Pianigiani E, Bilenchi R. Segmental phenolization for the treatment of ingrowing toenails: a review of 6 years experience. J Dermatolog Treat. 2004;15(3):179-81.
22. Shaikh FM, Jafri M, Giri SK, Keane R. Efficacy of wedge resection with phenolization in the treatment of ingrowing toenails. J Am Podiatr Med Assoc. 2008;98(2):118-22.
23. Bostanci S, Kocyigit P, Gürgey E. Comparison of phenol and sodium hydroxide chemical matricectomies for the treatment of ingrowing toenails. Dermatol Surg. 2007;33(6):680-5.
24. Bossers AM, Jansen, IMC, Eggink WF. Rational therapy for ingrown toenails a prospective study. Acta Orthopaedica Belgica. 1995; 58(3) 325-9.
25. Gerritsma-Bleeker CLE, Geelkerken RH. Partial Matrix Excision or Segmental Phenolization for Ingrowing Toenails. Arch Surg. 2002; 137:320-5.
26. Álvarez-Calderón R. Becerro de Bengoa M, Losa R,Sánchez, López D. Winograd technique. About one case. Rev Inter de Cienc Podol, 2008; 2-2: 49-56.
27. Carmona FJG, Galea JMP, Morato DF. Onicocriptosis crónica. Piel. 2005; 20(1): 53-5.
28. Jhonstone MW. Ingrown nail and others toenail problems. Surgical Treatments. California: Medicine;1962. p. 222-6.
29. Tamura BM, Golcman B, Cucé L, Sotto MN, Novo NF. Matricectomia da unha encravada do hálux: estudo imuno-histoquímico da matriz retirada. Surg Cosmet Dermatol. 2009;1(3):120-4.
30. Reis CMS, Reis Filho EGM. Tratamento cirúrgico da onicocriptose: excisão do tecido mole circunjacente ao leito ungueal utilizando radioeletro-cirurgia e criocirurgia. Surg Cosmet Dermatol. 2010;2(3):180-3.
This study was carried out at the Centro de Estudos da Unha of the Instituto de Dermatologia Professor Rubem David Azulay of the Santa Casa de Misericórdia do Rio de Janeiro – Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}