


Fernanda Manfron Batista Rosas1; Fabiane Mulinari-Brenner2; Karin Adriane Helmer1
Introduction: Acne scars are common, and their treatment is challenging. Several techniques have been used to remove, reposition, and flatten acne scars to improve the appearance of the skin’s surface. More recently, fractional CO2 laser has been used to correct such scars due its good results and shorter recovery time.
Objective: To evaluate and compare fractional CO2 laser vs. dermabrasion-based treatment of acne scars.
Methods: Nine patients were assessed – six received fractional CO2 laser and three were treated with dermabrasion. Subjective and objective parameters were evaluated for both treatment modalities.
Results: Both patient groups showed objective and subjective improvement.
Conclusions: This study has demonstrated that fractional CO2 laser and dermabrasion-based treatments have similar efficacy in moderate to severe acne scars.
Keywords: CICATRIX; ACNE VULGARIS; LASER THERAPY.
Acne has a 90% prevalence rate among adolescents,1 persisting into adulthood in 12-14% of cases, with severe social and psychological implications.2,3 Inflammatory lesions may result in permanent scarring.4 Roughly 1% of the population develops acne scars, although only one in seven people deem it a disfiguring condition.5
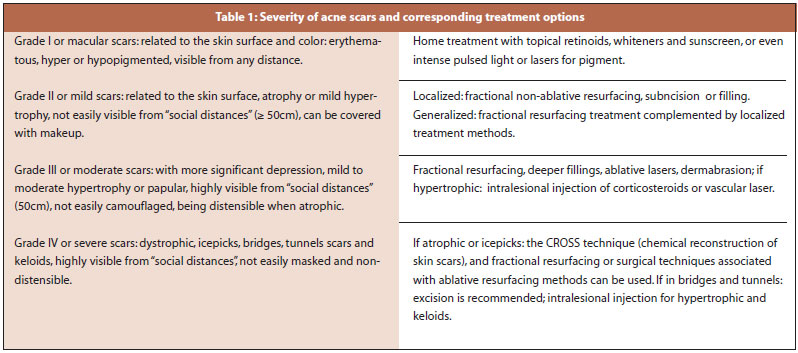
Acne scars can be of three types: hypertrophic (keloidal, papular andbridges), dystrophic, and depressed (distensible and non-distensible). The latter can be further subdivided into superficial, medium or crateriform and deep (icepick and tunnel scars).6 The severity of these scars can be classified into four grades, 7 with the type and severity of the scars determining the viable treatment options (Table 1).8-10
Resurfacing (i.e. remodeling of the skin surface) involves the removal of the epidermis and superficial dermis, leaving the skin appendages (sebaceous glands, hair follicles and sweat ducts) untouched, and promoting the production of collagen and the regeneration of the skin.11,12 Resurfacing methods include phenol or trichloroacetic acid based chemical peelings, dermabrasion, or ablative lasers.
Dermabrasion is a classic method of ablative resurfacing that was first described in the mid twentieh century.13 It is a mechanical method that employs either an electronic device with rotating diamond fraises, or the manual use of sandpaper, which allows more control of the treated depth. The risk of unsightly scarring depends on the depth reached – which is operator-dependent – and means that proper training is crucial. Reepithelialization begins at the wound’s borders and from the epidermis of the skin appendages (particularly the hair follicles). Healing is therefore slower, and adverse effects, such as erythema and edema, can be more prolonged.14
One or two sessions are recommended for the treatment of acne scars. The most commonly reported complication is hyperpigmentation.15 Bagatin et al. described the use of dermabrasion in conjunction with isotretinoin as a treatment that will not result in hypertrophic scars, and leading to the improvement of atrophic lesions.16
Treatments using new technologies have become popular in recent years for correcting acne scars. Ablative CO2 laser had long been considered by most authors to be the gold standard for the correction of depressed, icepick type scars. However, due to complications inherent in this method and also the long recovery time, its use was discontinued. With the introduction of fractional technology, CO2 laser has recovered its main role in the treatment of acne scars.17-23 The concept of fractional photothermolysis – treating zones in the epidermis and/or dermis while leaving some areas untouched following a grid pattern – was introduced by Manstein et al.in 2004.24 Those intact areas, located between the treatment zones, help lead to a faster reepithelialization (about five days) and a decreased risk of unsightly scars and dyschromia.8,17,25 This technique has lent safety to the treatment of extrafacial areas and for patients with higher phototypes. The number of sessions has an inverse relationship with the level of laser energy used (i.e. higher energy levels are capable of achieving good results with fewer sessions), however with a correspondingly higher rate of complications. In an attempt to reduce these limitations, Metelmann et al.26 described the Croll’s localized technique (reconstructive surgery of acne scars using a localized laser), which by reducing the laser device’s spot area and adapting it to the lesion’s shape, decreases the distance between points and increases the depth of the shots.
The present study’s objective was to evaluate the efficacy and side effects of the fractional CO2 laser and dermabrasion-based treatment of acne scars, comparing the two methods.
A retrospective study of patients with acne scars and treated with fractional CO2 laser and dermabrasion at the Cosmiatry Outpatient Clinic of the Hospital de Clinicas of the UFPR, was carried out between July and December 2010. All procedures were performed by resident physicians under the supervision of a preceptor physician.
Nine patients were included – seven women and two men, aged 27-58, with acne scars grade III or IV, no history of previous ablative treatment, and with no active acne lesions.
The patients were divided into two groups, according to their personal preference for treatment type after receiving an explanation of the two types of procedures (fractional CO2 laser and dermabrasion). An informed consent contract was signed by each patient, according to the specific type of procedure he or she would undergo.
Six patients received three sessions of fractional CO2 laser treatment at 30-day intervals. Three patients received a single dermabrasion session.
The patients’ skin was prepared with triple formulation (0.05%tretinoin, 4% hydroquinone and 0.01% fluocinolone acetonide) at least 15 days before the procedure. An anti-herpetic therapy (acyclovir 400mg, 8/8h) was started one day before the procedure, and maintained for five days.
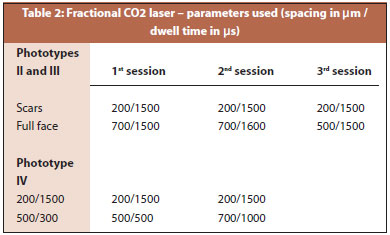
The patients treated with fractional CO2 laser (n= 6) were instructed to use a topical anesthetic cream (Dermomax®, Laboratório Aché, São Paulo, Brazil, lidocaina 4%) 30 to 45 minutes before the procedure. This was removed immediately before the laser application. The device used was the SmartXide Deka®, with 30MJ-power, and following the parameters described below. A reduced space and a greater depth in the scars were maintained (when compared with the remaining areas of the face), according to the patients’ respective phototypes (Table 2). After treatment, the patients were instructed to wash their face two times a day and apply solid petrolatum for five days.
Patients undergoing dermabrasion received anesthesia with 2% lidocaine before the treatment, followed immediately by local application of 35% trichloracetic acid across the face, and subsequent sanding with electric dermoabrasor and a manual finish with sandpaper number 180 on the scars’ sites. Dressing with neomycin and tulle was put in place on the treated area, and kept in place for 40 hours. Moisturizer cream was applied on the remaining areas of the face. After the removal of the dressing, patients were instructed to clean the face three times a day at home and apply antibiotic cream for five days. Both groups were instructed to resume the use of the triple formula after medical evaluation (between seven to 14 days of the procedure) and sunscreen seven days after the procedure.
Subjective evaluations were carried out with patients regarding the discomfort and pain tolerance during procedures, the results, and the side effects. The objective assessment was carried out by three experienced dermatologist physicians, and was conducted through the analysis of photographs taken from five different angles, in order to evidence the depth of the scars (30º and 45º to the right, 0º central, 30º and 45º to the left).
The discomfort described during the procedure varied from moderate to significant among patients treated with CO2 laser. Each of the three patients who underwent dermabrasion described a different degree of discomfort: absent, moderate, and significant. Crusts developed with 67% and 100% of patients treated with CO2 and dermabrasion, respectively. Of those, 67% also presented with petechiae, all with complete resolution within seven days. Only one dermabrasion patient (one from a grand total of nine) had post-inflammatory hyperpigmentation, which receded within eight weeks under treatment (4% hydroquinone and 0.05% clobetasol cream).
The subjective assessment, carried out with a questionnaire given 30 days after the treatment with fractional CO2, suggested 50% of patients had moderate improvement and 50% significant improvement – an evaluation that has persisted for at least 90 days after the procedure. Of the patients who underwent dermabrasion, only two were evaluated after 30 days, describing moderate to significant improvement. All three patients answered the questionnaire in the 90-day follow up, with 33% reporting moderate improvement, and 67% reporting significant improvement.
In the general review, carried out 90 days after the procedure, the treatments were described as very good and excellent by CO2 and dermabrasion patients, who stated they would recommend the therapies.
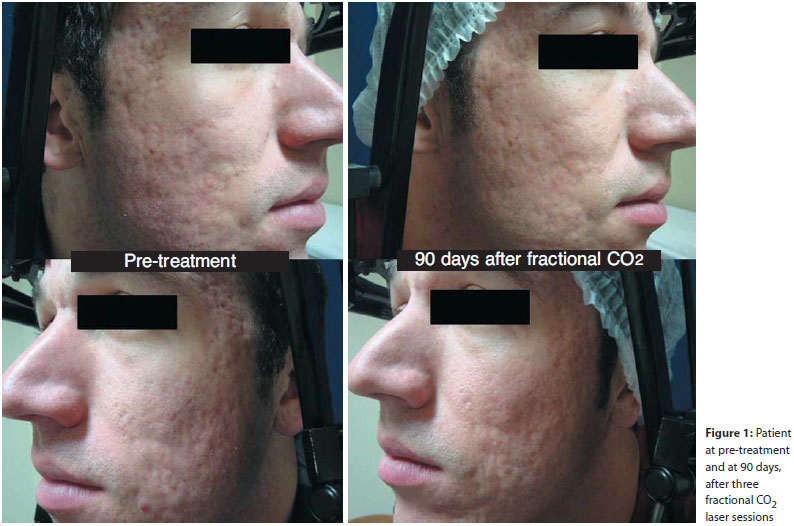
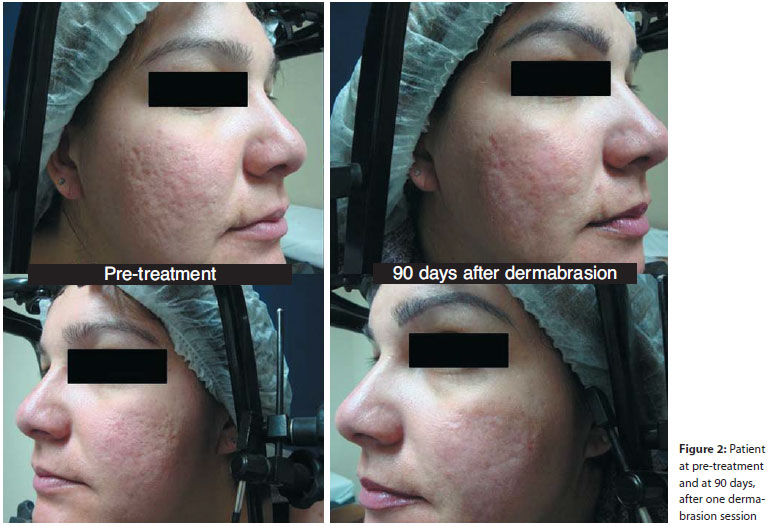
In the objective evaluation, carried out through photographs (Figures 1 and 2), one evaluator physician reported one instance of an absent answer from a single patient, while another reported one significant answer in another patient, at 30 days after treatment with CO2. All other evaluations reported moderate to significant improvement. Ninety days after, however, some degree of improvement was reported in all patients treated with fractional CO2 or dermabrasion, most of them moderate.
The Wilcoxon test indicated an absence of statistical difference between treatments after 30 and 90 days. The Kendal test, used to analyze the existence of agreement between evaluators, suggested there was no statistical difference between the evaluator physicians 1, 2, and 3. On the other hand, there was statistical difference (p = 0.036) between patients and evaluators in the comparison of the degree of improvement 30 days after treatment. In this case, the patients' subjective assessment was better than the those of the physicians, which can be explained by the difficulty in photographically recording the improvement in the relief height of scars. The Mann-Whitney U-Test was used to compare the two treatments in light of the results. There was a difference between the treatments regarding erythema and swelling (greater in dermabrasion, with p = 0.005 to 0.034, depending on the items evaluated), nonetheless there was no difference in the improvement degree and general evaluation of the treatments.
The treatment of acne scars requires the use of multiple related techniques, 24 with fractional CO2 laser and dermabrasion being recommended for resurfacing grades III and IV scars. These techniques can be used in conjunction with surgical corrections, chemical peels and fillers.
The present study demonstrated that fractional CO2 laser and dermabrasion are effective in the treatment of acne scars. Responses to the treatments are comparable, though with different recovery times, with all patients reporting moderate to significant improvement (51-100%). The data obtained is consistent with the literature, which shows minimum improvement of 26-50% in the texture, atrophy, and general appearance of scars in patients treated with two or three fractional CO2 sessions.18, 20,23,27
The objective of these treatments is long-term improvement for the patients. The edema and the dyschromias seem to interfere with the physicians’ proper assessment of patients during the first weeks of treatment. The most obvious improvement – observed both objectively and subjectively three months after the end of the treatment – is consistent with studies that show that neocollagenesis persists for at least three months after the end of the treatments.23,28 Long-term studies suggest a progressive improvement in the first six months after the end of the treatments.18
The most frequent side effect reported in the literature, following fractional CO2 laser, is post-inflammatory hyperpigmentation. This side effect is more frequently associated with higher phototypes and when more aggressive parameters are used. 18In the present study, none of the patients treated with this technique showed postinflammatory hyperpigmentation, which may have been prevented by the use of triple formulation in the preparation of the skin and/or the use of more aggressive parameters, in a focused way on the scars only, as described by Mettelmann et al. 26
Regarding the evaluation of dermabrasion as a treatment for correcting acne scars, only a few studies have been published on the subject over the past 15 years.29 Fulton and Rahimi 14 evaluated 25 volunteers who underwent the procedure, describing satisfied patients who reported minimal complications (hyperpigmentation being the most frequent, reported in 36% of cases). In the present study one dermabrasion patient (33%) had this complication, with the remaining three reporting moderate to significant improvement of scars.
In the literature, only one prospective study has compared the use of fractional CO2 laser and dermabrasion in the treatment of surgical scars on the face (coinciding with the present study’s objective), and concluded that the laser modality is safer, notwithstanding the efficacy of both methods.30
Recognizing that the small number of patients in this study presents limitations for interpreting its results, the study has nonetheless demonstrated a similar efficacy (absence of statistical difference) for the treatment of acne scars with fractional CO2 laser and dermabrasion. New technology-based treatments, which are progressively less dependent on operator-physicians, are becoming increasingly popular, since parameters pre-set by the device manufacturers can be used instead. Nevertheless, it is important to note that the treatment of acne scars is multimodal and varied, and better responses result from a combination of techniques, with dermabrasion still providing excellent outcomes and low complication rates, albeit with a longer recovery time.
1. C. Prevalence, severity, and severy risk factors of acne in high school pupils: a community-based study. J Invest Dermatol. 2009; 129 (9) 2136-41.
2. Williams C, Layton AM. Persistant acne in women: implications for the patient and for therapy. Am J Clin Dermatol. 2006; 7(5) 281-90.
3. Capitanio B, Sinagra JL, Bordignon V, Fei PC, Picardo M, Zouboulis CC. Underestimated clinical features of postadolescent acne. J Am Acad Dermatol. 2010; 63 (5) 782-88.
4. Fabbrocini G, Annunziata MC, D'Arco V, De Vita V, Lodi G, Mauriello MC, et al. Acne scars: Patogenesis, Classification and Treatment. Dermatol Res Pract. 2010;2010:893080.
5. Cunliffe WJ, Gould DJ. Prevalence of facial acne vulgaris in late adolescence and in adults. BMJ. 1979; (1) 1109-10.
6. Kadunc BV, Almeida ART. Surgical treatment of facial acne scars based on morphologic classification: A Brazilian Experience. Dermatol Surg. 2003; 29 (12): 1200-9.
7. Goodman GJ, Baron JA. Post acne scarring - a qualitative global scarring grading system. Dermatol Surg. 2006;32(12):1458-66.
8. Goodman GJ. Treatment of acne scarring. Int J Dermatol. 2011;50(10):1179-94.
9. Lee JB, Chung WJ, Kwahck H, Lee KH. Local treatment of acne scars with trichloroacetic acid: chemical reconstruction of acne scars method. Dermatol Surg. 2002; 28(11): 1017-21.
10. Fabbrocini G, Cacciapuoti S, Fardella N, Pastore F, Monfrecola G. CROSS technique: chemical reconstruction o skin scars method. Dermatol Ther. 2008; 21(Suppl 3): S28-32.
11. Weinstein C, Roberts TL. Aesthetic skin resurfacing with the high-energy ultrapulsed CO2 LASER. Clin Plast Surg. 1997; 24(2): 379-405.
12. Weistein C. Carbon dioxide laser resurfacing. Long term follow-up in 2123 patients. Clin Plast Surg. 1998; 25(1):109-30.
13. Kurtin A. Corrective surgical planning of skin: new technique for treatment of acne scars and other skin defects. Arch Derm Syphilol. 1953; 68(4): 389-97.
14. Riviera AE. Acne scarring: a review and current treatment modalities. J Am Acad Dermatol 2008; 59(4): 659-75.
15. Fulton JE, Rahimi AD. Dermabrasion using CO2 dry ice. Dermatol Surg 1999; 25(7): 544-48.
16. Bagatin E, Guadahim LRS, Yarak S, Kamamoto CSL, Almeida FA. Dermabrasion for acne scars during treatment with oral isotretinoin. Dermatol Surg. 2010;36(4):483-89.
17. Jordan R, Cumminis C, Burls A. LASER resurfacing of the skin for the improvement of facial acne scarring: a systematic review of the evidence. Br J Dermatol. 2000;142(3):413-23.
18. Manuskiatti W, Triwongwaranat D, Varothai S, Eimpunth S, Wanitphakdeedecha R. Efficacy and safety of a carbon-dioxide ablative fractional resurfacing device for treatment of atrophic acne scars in Asians. J Am Acad Dermatol. 2010;63(2):274-83.
19. Avram MM, Tope WD, Yu T, Szachowicz E, Nelson JS. Hypertrophic scarring of the neck following ablative fractional carbon dioxide LASER resurfacing. Lasers Surg Med. 2009;41(3):185-8.
20. Chapas AM, Brightman L, Sukal S, Hale E, Daniel D, Bernstein LJ, Geronemus RG. Successful treatment of acneiform scarring with CO2 ablative fractional resurfacing. Lasers Surg Med. 2008;40(6):381-6.
21. Wang YS,Tay YK, Kwok C. Fractional ablative carbon dioxide LASER in the treatment of atrophic acne scarring in Asian patients: a pilot study. J Cosmet Laser Ther. 2010;12(2):61-4.
22. Cho SB, Lee SJ, Kang JM, Kim YK, Chung WS, Oh SH. The efficacy and safety of 10,600-nm carbon dioxide fractional laser for acne scars in Asian patients. Dermatol Surg. 2009;35(12):1955-61.
23. Chan NPY, Ho SGY, Yeung CK, Shek SYN, Chan HH. Fractional ablative carbon dioxide laser resurfacing for skin rejuvenation and acne scars in Asians. Lasers Surg Med. 2010;42(9): 615-23.
24. Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional photothermolisis: a new concept for cutaneous remodeling using microscopic pattern of thermal injury. Lasers Surg Med. 2004; 34(5):426-38.
25. Gotkin RH, Sarnoff DS, Cannarozzo G, Sadick NS, Alexiades-Armenakas M. Ablative Skin resurfacing with a novel microablative CO2 laser. J Drugs Dermatol. 2009; 8(2):138-44.
26. Metelmann U, Machado Filho CA, Meireles SIFC, Teixeira LPVB. Técnica de Croll: cirurgia de reconstrução com laser localizado em cicatrizes de acne. Surg Cosmet Dermatol. 2010; 2(4):336-9.
27. Ong MWS, Bashir SJ. Fractional laser resurfacing for acne scars: a review. Br J Dermatol.2012; 166(6):1160-69.
28. Hantash BM, Bedi VP, Kapadia B, Rahman Z, Jiang K, Tanner H, et al. In vivo histological evaluation of a novel ablative fractional resurfacing device. Lasers Surg Med. 2007;39(2):96-107.
29. Langdon RC. Regarding dermabrasion for acne scars. Dermatol Surg. 1999; 25(11): 919.
30. Christophel JJ, Elm C, Endrizzi BT, Hilger PA, Zelickson B. A randomized controlled trial of fractional laser thetapy and dermabrasion for scar resurfacing. Dermatol Surg. 2012;38(4): 595-602.
This study was carried out at the Dermatology Service of Hospital de Clinicas, Universidade Federal do Paraná (HC-UFPR) – Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}