


Mariana Freitas de Assis Pereira Rosa1; Carlos Arthur de Figueiredo Athayde2; Gustavo Costa Verardino3; Ricardo Barbosa Lima4
Funding: None
Conflict of interest: None
Submitted on: 10/31/2025
Final decision: 12/21/2025
How to cite this article: Rosa MFAP, Athayde CAF, Verardino GC, Lima RB. Negative pigment network and its importance in the diagnosis of melanoma: a case report. Surg Cosmet Dermatol. 2026;18(1):e20260535.
The "negative pigment network" is a dermoscopic feature observed in melanomas, melanocytic nevi, and dermatofibromas; however, studies indicate that it is more frequently associated with melanoma. The aim of this case report is to highlight the negative pigment network as an important clue in the diagnosis of melanoma and that its presence, even in the absence of other typical dermoscopic features of melanoma, should prompt further investigation followed by biopsy to confirm the diagnosis.
Keywords: Melanoma; Dermoscopy; Diagnosis
The dermoscopic feature described as "negative pigment network (NPN)," introduced by Menzies et al. in 1996, consists of serpiginous, interconnected hypopigmented lines forming a mesh-like pattern, with darker areas filling the spaces between them. This finding is seen as the inverse of the pigment network, and is also termed "inverse network."1 Its presence may be observed in melanomas, congenital and acquired melanocytic nevi, Spitz nevi, and dermatofibromas. However, NPN has emerged as an important dermoscopic criterion in the diagnosis of melanoma due to its high specificity (77.4%), despite its low sensitivity (34.6%).1,2 We report a case in which NPN was the main dermoscopic finding suggestive of melanoma in a lesion lacking other characteristic melanoma features.
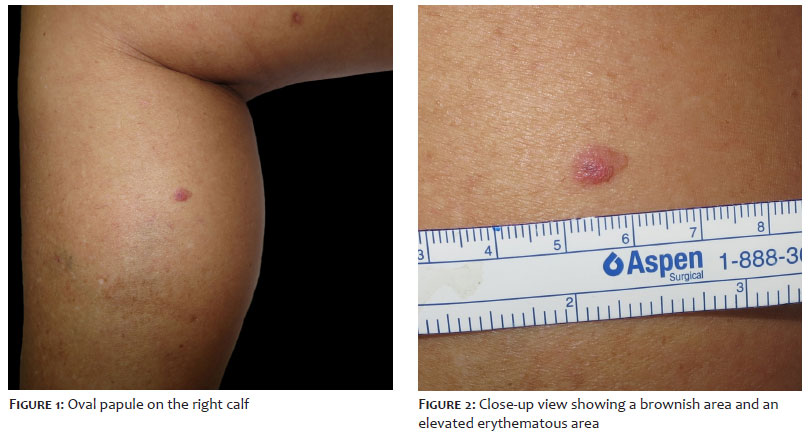
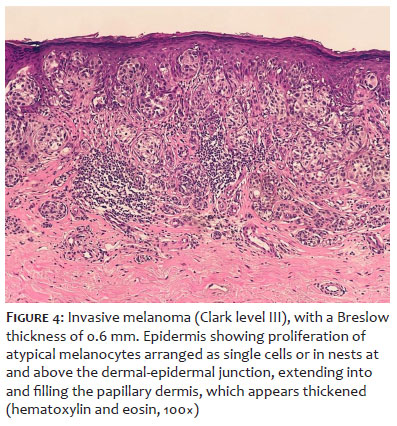
A 71-year-old man presented with an erythematous, infiltrated, warm, and painful area on the left leg following local trauma, consistent with cellulitis. A full-body skin examination was performed, and an oval papule with regular borders was identified on the right calf. The lesion displayed a brownish area and a more elevated erythematous area with a finely granular surface, measuring 8 mm in its greatest dimension (Figure 1-2). Dermoscopic examination revealed a predominant NPN pattern, with brown areas and erythematous areas. Between the white reticular lines, brownish globular-like structures and dotted vessels were observed (Figure 3). Based on the clinical and dermoscopic features, melanoma was the leading diagnostic hypothesis, and an excisional biopsy with a 2-mm longitudinal margin was performed. Histopathological examination revealed an invasive melanoma, Clark level III, with a Breslow thickness of 0.6 mm (Figure 4). The patient was subsequently referred for margin widening.
NPN is a dermoscopic structure observed in both melanocytic and non-melanocytic lesions, which aids in the diagnosis of melanoma. In a study of 679 patients evaluating the frequency and characteristics of NPN in melanomas, Spitz nevi, and non-melanocytic lesions, Pizzichetta et al. found that this dermoscopic feature was significantly more frequent in melanomas (34.6%) than in Spitz nevi (28.8%), melanocytic nevi (18.2%), and dermatofibromas (11.3%).2 In a review of 401 melanomas, NPN was frequently identified in melanomas lacking typical dermoscopic features, suggesting that NPN may serve as a useful diagnostic clue in challenging cases.1 Likewise, in nevus‐associated melanomas without a clinically evident nevus component, NPN may also point toward the diagnosis.1,3
In the present case, the clinical appearance of the lesion showed subtle asymmetry and color variation, which did not allow for a definitive clinical diagnosis of melanoma. However, dermoscopy revealed NPN as a key finding, raising suspicion for melanoma even in the absence of more classic features such as atypical pigment network, blue-white veil, pseudopods, or radial streaks. This case report underscores the importance of NPN as a dermoscopic feature in the clinical evaluation of pigmented skin lesions.2
The presence of NPN, particularly when irregularly distributed or located peripherally, and when associated with other dermoscopic features such as asymmetric pigmentation and a multicomponent pattern, may improve diagnostic accuracy for melanoma. In melanomas, NPN is typically heterogeneous, with thicker hypopigmented lines surrounding pigmented polygonal areas of varying sizes, and may cover less than 20% of the lesion surface.1 In spitzoid melanocytic lesions, including spitzoid melanoma, NPN is more apparent in lesions > 5 mm, often associated with shiny white lines and dotted vessels in globular areas; the presence of blue-white veil may obscure NPN due to reduced color contrast.4 In the present case, NPN was irregularly distributed and associated with more than one color tone and a dotted vascular pattern, further supporting the diagnostic suspicion, consistent with previous studies.1,2,4
NPN may also be associated with invasive melanomas.1,5 In a retrospective study of 269 melanocytic lesions investigating dermoscopic predictors of melanoma in lesions ≤ 5 mm in diameter (mini-melanomas), the presence of NPN or blue-white veil was associated with invasive lesions.5 In the present case, although measuring > 5 mm, which may have facilitated visualization of NPN, the lesion was also associated with dermal invasion. Therefore, recognition of NPN during dermoscopic evaluation may serve as a warning sign in melanoma diagnosis and in preventing progression to more advanced stages of invasion.
Confocal microscopy studies have helped correlate dermoscopic components with histopathological findings of NPN. Farnetani et al. observed that, in melanocytic lesions, the hypopigmented lines of NPN correspond to broadened epidermal rete ridges with overlying surface dells and wedge-shaped hypergranulosis, whereas the pigmented areas between the lines correlate with a predominantly junctional proliferation of melanocytes along and between the elongated rete ridges. Additionally, they highlighted an important clinical distinction between melanomas and nevi with NPN. Melanomas tend to occur in older patients,6 as observed in our case.
The presence of NPN may increase the likelihood of a melanoma diagnosis, and its identification during dermoscopic examination should prompt further investigation or biopsy for diagnostic confirmation.1,2 This case also highlights the importance of performing a full-body skin examination regardless of the patient's presenting complaint. In this case, although the consultation was prompted by cellulitis, full-body skin examination enabled the detection of a highly aggressive neoplasm at a stage of lower morbidity, curable by surgery, owing to the identification of NPN on dermoscopy.
Mariana Freitas de Assis Pereira Rosa
ORCID: 0000-0002-8422-5332
Author's contribution: Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to studied cases, Critical review of the literature, Critical revision of the manuscript
Carlos Arthur de Figueiredo Athayde
ORCID: 0009-0003-0169-2264
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to studied cases, Critical review of the literature, Critical revision of the manuscript
Gustavo Costa Verardino
ORCID: 0000-0002-1212-3273
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Ricardo Barbosa Lima
ORCID: 0000-0002-4297-3236
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to studied cases, Critical review of the literature, Critical revision of the manuscript.
1. Bassoli S, Ferrari C, Borsari S. Negative pigment network identifies a peculiar melanoma subtype and represents a clue to melanoma diagnosis: a dermoscopic study of 401 melanomas. Acta Derm Venereol. 2013;93(6):650-5.
2. Pizzichetta MA, Talamini R, Marghoob AA. Negative pigment network: an additional dermoscopic feature for the diagnosis of melanoma. J Am Acad Dermatol 2013;68(4):552-9.
3. Reiter O, Kurtansky N, Nanda JK, Busam KJ, Scope A, Musthaq S, et al. The differences in clinical and dermoscopic features between in situ and invasive nevus‐ associated melanomas and de novo melanomas. J Eur Acad Dermatol Venereol. 2021;35(5):1111–8.
4. Spadafora M, Farnetani F, Borsari S, Kaleci S, Porat D, Ciardo S, et al. Clinical, dermoscopic and reflectance confocal microscopy characteristics associated with the presence of negative pigment network among spitzoid neoplasms. Exp Dermatol. 2025;34(8).
5. Nazzaro G, Maronese CA, Casazza G. Dermoscopic predictors of melanoma in small diameter melanocytic lesions (mini-melanoma): a retrospective multicentric study of 269 cases. Int J Dermatol. 2023;62(8):1040-9.
6. Farnetani F, Scope A, Mazzoni L, Mandel VD, Manfredini M, Magi S, et al. A comparative dermoscopic and reflectance confocal microscopy study of naevi and melanoma with negative pigment network. J Eur Acad Dermatol Venereol. 2019;33(12):2273–82.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}