


Fernanda Guimarães Lopes1; Juliana Cristina Silva Fraga1; Mariana Campos Souza Menezes1; Ana Karen Alves2; André Rossetti Portela3
Funding: None
Conflict of interest: None
Submitted on: 09/30/2025
Final decision: 12/21/2025
How to cite this article: Lopes FG, Fraga JCS, Menezes MCS, Alves AK, Portela AR. Bednar tumor: a case report. Surg Cosm Dermatol. 2026;18(1):e20260520.
Bednar tumor is a rare variant of dermatofibrosarcoma protuberans. A 45-year-old woman presented with a progressively enlarging bluish macule on the shoulder. Biopsy revealed a pigmented spindle cell neoplasm, with immunohistochemistry positive for CD34 and negative for S100 and SOX-10. Surgical excision with margin mapping was performed. Surgical treatment with margin control is the gold standard for the management of Bednar tumor. This technique ensures complete resection, with outcomes comparable to those of Mohs micrographic surgery. This case highlights the importance of clinical suspicion in atypical hyperpigmented skin lesions.
Keywords: Dermatofibrosarcoma; Immunohistochemistry; Dermatology
Dermatofibrosarcoma protuberans (DFSP) is a rare cutaneous neoplasm of dermal origin, characterized by slow growth, locally aggressive behavior, and a high rate of recurrence, although it has low metastatic potential.1-4 It accounts for approximately 1% of all cutaneous malignancies1,2 and less than 2% of all sarcomas,3 most commonly affecting young and middle-aged adults, although it may occur from childhood to advanced age.1,5 The most frequent sites include the trunk, shoulders, and proximal extremities,4,6 with less frequent involvement of the head and neck.7
Several histological variants of DFSP have been described, including atrophic, fibrosarcomatous, giant fibroblastoma, myxoid, and pigmented forms.3,4 The latter, known as Bednar tumor, was first described by Bednar in 1957 under the term storiform neurofibroma.1-3,7 It is an uncommon presentation, accounting for less than 5% of all DFSP cases,1-4,7 and is characterized by the presence of melanin-containing dendritic melanocytes dispersed among spindle cells arranged in a storiform pattern.3,4,7
Clinically, Bednar tumor typically presents as a hyperpigmented nodule or plaque, which may lead to diagnostic confusion with other pigmented lesions, such as desmoplastic malignant melanoma, blue nevus, pigmented neurofibroma, and melanotic schwannoma.1,3,4 Definitive diagnosis requires histopathological evaluation combined with immunohistochemical analysis,1,4,7 which aids in distinguishing between these entities.
A 45-year-old woman with no personal or family history of cutaneous neoplasms presented to a dermatology outpatient clinic in February 2025 with the complaint of a well-demarcated, painless bluish macule on the left shoulder, which had been progressively enlarging. She was unable to specify the onset of the lesion.
Given the clinical presentation and reported growth, a 4-mm punch biopsy (Figure 1) was performed for histopathological examination, which revealed a spindle cell neoplasm suggestive of fibrohistiocytic origin, with a melanocytic pigment component, extending to both radial and deep margins.
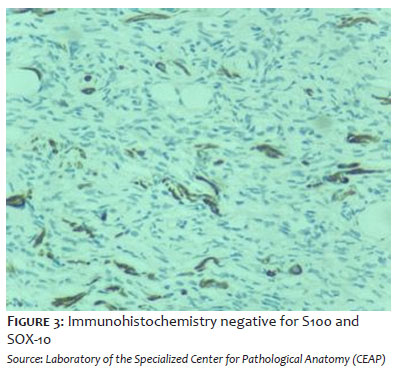
Complementary immunohistochemical analysis was performed to further define the diagnosis. The antibody panel demonstrated diffuse positivity for CD34 and was negative for CD10/56C6, D2-40, S100, and SOX-10 (Figures 2, 3, and 4).
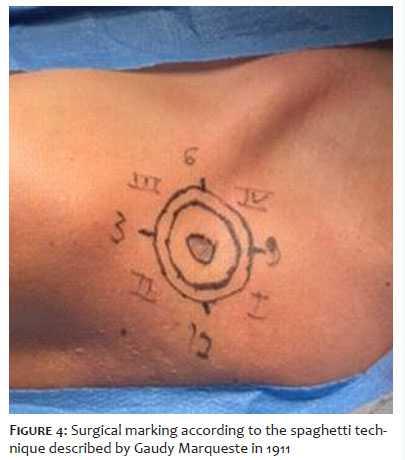
Based on these findings, surgical excision using the spaghetti technique, described by Gaudy Marqueste in 1911,8 was performed. In this approach, the tumor is preserved centrally while narrow, sequential peripheral segments are excised, carefully labeled according to their anatomical position, and submitted individually for histopathological evaluation of radial and deep margins.
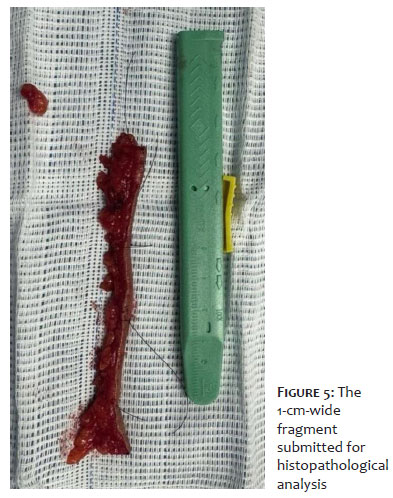
In the present case, the tumor remnant was maintained centrally, and a 2-cm margin was delineated for excision of a 1-cm-wide peripheral fragment (Figures 5 and 6). This fragment was divided and marked into 4 quadrants for microscopic evaluation of surgical margins.
Histopathological analysis confirmed that both radial and deep margins were free of tumor involvement. Subsequently, complete excision of the tumor remnant was performed, including the adjacent skin corresponding to the previously established safety margin. Reconstruction was performed using a rotation flap, considering the anatomical site and the need for coverage with adjacent tissue of similar texture and color (Figures 7 and 8).
The final excised specimen consisted of a grayish, rounded skin fragment measuring 4.5 × 3.5 × 0.8 cm, containing a centrally located ulcerated lesion measuring 2.7 × 2.5 cm. The findings were suggestive of DFSP.
Bednar tumor is a rare variant of DFSP characterized by the presence of melanin and dendritic spindle cells in the tumor stroma.7 It is a slow-growing neoplasm with low metastatic potential but a high risk of local recurrence if not adequately excised.6
The clinical presentation observed in this patient — a painless, progressively enlarging bluish macule — illustrates the diagnostic challenge of this variant, which may be mistaken for blue nevus, pigmented dermatofibroma, desmoplastic melanoma, or pheohyphomycosis.1-4 Histopathological examination combined with immunohistochemistry is essential for diagnosis, with the characteristic pattern of CD34 positive and S100/SOX-10 negative confirming the fibrohistiocytic origin of the tumor.5,7
Surgical excision with margin mapping is effective in ensuring complete tumor removal, although Mohs micrographic surgery remains the gold standard treatment.9,10 Studies have demonstrated that histological margin control significantly reduces local recurrence rates compared with conventional excision.10
In the present case, the spaghetti technique was employed, in which the main lesion is initially preserved in situ, and peripheral ("spaghetti-like") tissue segments are excised around the lesion and submitted individually for histopathological analysis to determine the presence of tumor cells at the margins. After confirmation of clear margins, definitive excision of the central lesion is performed. A disadvantage of this method is the requirement for at least 2 surgical stages, which may increase the risk of local complications and prolong healing time.11
Reconstruction using a rotation flap was selected due to the shoulder location, allowing preservation of both function and aesthetics. Local reconstructive techniques are often necessary given the wide margins recommended (generally 2-4 cm).12
Due to the rarity and nonspecific clinical features of Bednar tumor, its recognition requires a high index of clinical suspicion and accurate histopathological confirmation. Reporting additional cases and ongoing literature review are essential to improve understanding of the biological behavior and optimal management of this rare neoplasm.
Bednar tumor is a rare cutaneous neoplasm with low metastatic potential but a high risk of local recurrence. Early diagnosis, combined with appropriate histopathological and immunohistochemical evaluation, is crucial for effective management. Complete surgical excision, preferably with margin control, is the treatment of choice. This case underscores the importance of continuous monitoring of pigmented lesions and the use of safe surgical techniques to prevent recurrence.
Fernanda Guimarães Lopes
ORCID: 0000-0003-1665-6437
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Juliana Cristina Silva Fraga
ORCID: 0000-0002-1593-8742
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to studied cases, Critical review of the literature, Critical revision of the manuscript.
Mariana Campos Souza Menezes
ORCID: 0000-0002-7727-6430
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to studied cases, Critical review of the literature, Critical revision of the manuscript.
Ana Karen Alves
ORCID: 0009-0002-8709-3910
Author's contribution: Approval of the final version of the manuscript, Conception and design of the study, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
André Rossetti Portela
ORCID: 0000-0002-7040-8138
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Kalonia T. Bednar tumour, an uncommon tumour of the skin: a report of two cases. Pan Afr Med J. 2022;42:261.
2. Amonkar GP. Bednar Tumor: An Uncommon Entity. Dermatopathology (Basel). 2016;3(2):36-8.
3. Dumitru A. When an old pigmented lesion becomes serious: the problematic diagnosis of low-grade skin malignancies – Bednar tumor with fibrosarcomatous transformation. Rom J Orthop Surg Traumatol. 2021;3(1):14–21.
4. Spandidos DA. Fibrosarcomatous pigmented dermatofibrosarcoma protuberans: a case report with review of the literature. Oncol Lett. 2012;4(1):191–4.
5. Haque AU. Fine Needle Aspiration Cytology of Pigmented Dermatofibrosarcoma Protuberance (Bednar Tumor) & its Pathogenesis. Int J Pathol. 2018;16(2):82–6.
6. Mendes M. Tumor de Bednar (dermatofibrossarcoma protuberante pigmentado): relato de um caso. An Bras Dermatol. 2004;79(1):87–90.
7. Fletcher CD, Theaker JM, Flanagan A, Krausz T. Pigmented dermatofibrosarcoma protuberans (Bednar tumour): melanocytic colonization or neuroectodermal differentiation? A clinicopathological and immunohistochemical study. Histopathology. 1988;13(6):631-643.
8. Ciongariu A, et al. Bednar tumor with fibrosarcomatous transformation – case presentation and literature review. Rom J Orthop Surg Traumatol. 2021;4(3):124–129.
9. Lowe GC. Dermatofibrosarcoma protuberans: treatment with Mohs micrographic surgery or wide local excision. J Am Acad Dermatol. 2018;78(3):492–7.
10. Gloster HM Jr. Surgical treatment of dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1996;35(6):943–7.
11. Shimizu GS, Hamdar FB, Santos CHST. Uso da técnica em "spaghetti" para tratamento cirúrgico do lentigo maligno. Rev Bras Cir Plást. 2019;34(1):151-5.
12. Cockerell CJ. Surgical margins and reconstructive options for dermatofibrosarcoma protuberans: a review. Dermatol Surg. 2012;38(10):1600–9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}