


Autores: Clarissa Brito Farias; André Martins Ornelas; Flauberto de Sousa Marinho
Funding: None
Conflict of interest: None
Submitted on: 08/05/2025
Final decision: 10/07/2025
How to cite this article: Farias CB, Ornelas AM, Marinho FS. Exuberant chronic paronychia: a surgical approach using the square flap technique. Surg Cosmet Dermatol. 2026;18(1):20260505.
Chronic paronychia is an inflammatory condition of the proximal nail fold, often associated with prolonged exposure to moisture and irritant substances. Surgical treatment is indicated in refractory cases. We report the case of a patient with involvement of all digits and an unsatisfactory response to clinical therapies. The square flap technique was employed, yielding favorable functional and aesthetic outcomes. This case highlights the efficacy of the surgical approach and underscores the importance of dermatologists' training in nail surgery techniques.
Keywords: Nails; Paronychia; Nail Diseases
Chronic paronychia (CP) is an inflammatory disorder of the proximal nail fold (PNF) lasting longer than 6 weeks. It accounts for approximately 18% of nail dystrophies and most commonly affects the first, second, and third fingers of the dominant hand, particularly in women with repeated exposure to moisture, cleaning agents, and local trauma. Health care professionals, homemakers, and food industry workers are among the most affected populations.1,2
CP etiology is multifactorial and involves cuticle disruption with exposure of the eponychium, irritant contact dermatitis, and secondary fungal infection (especially with Candida albicans).1-3 Cases associated with the use of medications, such as retinoids, tyrosine kinase inhibitors, and epidermal growth factor receptor inhibitors, have also been reported.4
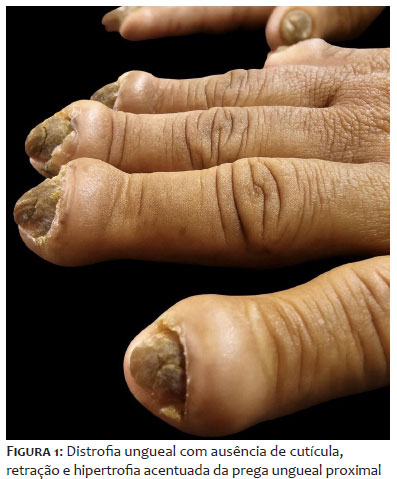
Clinically, CP is characterized by hypertrophy of the PNF and lateral nail folds, absence of cuticle, onychodystrophy, and pain.1-3 Initial treatment aims to eliminate triggering factors and includes topical and/or systemic medications such as antifungals, antibiotics, corticosteroids, and emollients. However, outcomes are often unsatisfactory and slow to achieve. Refractory cases, after at least 6 months of clinical treatment, may benefit from surgical intervention.5 Several techniques have been described in the past decade, among which the square flap technique, proposed by Ferreira Vieira d'Almeida et al. in 2016, stands out for providing favorable functional and aesthetic outcomes, in addition to reduced healing time.6
This study aimed to report a severe CP case treated surgically with the square flap technique. We provide a detailed description of the procedure, the outcomes obtained, and a brief literature review comparing different surgical techniques commonly employed in the treatment of CP. For this review, we conducted searches in the PubMed, SciELO, and CAPES Journals databases using the descriptors "chronic paronychia," "surgical treatment," and "paronychia surgeries."
A 44-year-old previously healthy woman, a homemaker, reported progressive nail changes for more than 20 years. She denied any family history of nail disorders. She reported previous use of topical and systemic antifungals, corticosteroids, and antibacterial agents without significant improvement.
On physical examination, nail dystrophy was observed in all fingers, with absence of cuticle, retraction, and marked hypertrophy of the PNF (Figures 1 and 2). Given the lack of response to prior therapies, surgical intervention was indicated.
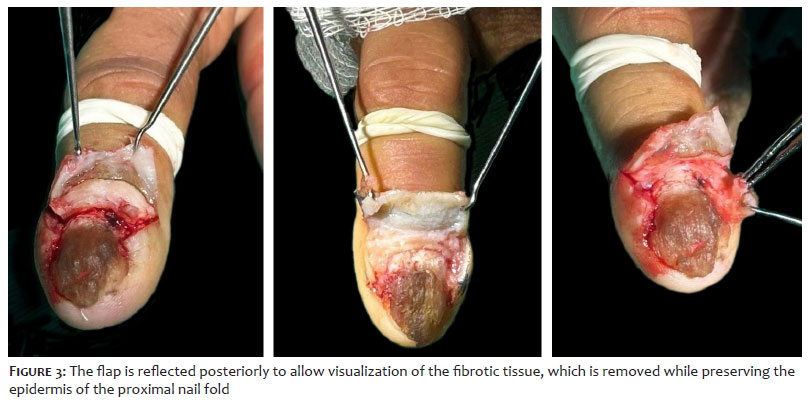
With the patient in the supine position and the upper extremity placed on a side table, antisepsis was performed using 2% chlorhexidine. A proximal digital nerve block was administered using 2% lidocaine without vasoconstrictor, followed by placement of a tourniquet at the base of the finger. Oblique markings measuring 3-4 mm were made over the PNF, followed by corresponding incisions. An incision was then made parallel to the epidermis, below the fibrotic tissue and above the nail plate, using a dental spatula to assist and prevent damage to the nail matrix.
This approach resulted in a square flap filled with fibrosis. The flap was reflected posteriorly to allow visualization of the fibrotic tissue, which was then removed using a No. 11 scalpel blade while preserving the epidermis of the PNF (Figure 3). The detached epidermis was repositioned and secured with simple interrupted 4-0 nylon sutures (Figure 4). Fibrotic tissue present in the lateral nail folds was removed through the same access. A pressure dressing was applied at the end of the procedure.
The surgical procedures were performed with 4- to 6-week intervals between the affected digits. Postoperatively, the patient was instructed to clean the area with saline solution and to use dipyrone for analgesia, along with cefadroxil 1 g/day for 7 days. Biotin 10 mg/day and fluconazole 150 mg 3 times weekly were also prescribed during follow-up.
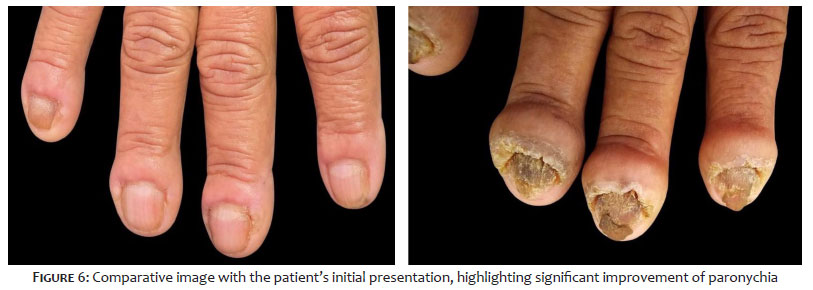
The patient demonstrated regression of nail fold hypertrophy, new cuticle formation, and improvement in both functional and aesthetic aspects of the nails (Figure 5). Compared with the initial presentation, a marked improvement was observed (Figure 6).
CP is an inflammatory disorder of the PNF, clinically characterized by erythema, edema, hypertrophy of periungual tissues, and absence of cuticle for at least 6 weeks. The nail plate becomes dystrophic, and patients may experience local pain, substantially impairing quality of life. Repeated exposure to moisture and irritants damages the cuticle, facilitating the entry of allergens and pathogens into the nail folds, leading to recurrent episodes of acute inflammation and subsequent fibrosis. The nail folds become progressively more exposed, compromising the protective seal and perpetuating the continuous entry of microorganisms and irritant or allergenic substances.1,2
Clinical management of CP involves eliminating triggering factors, including excessive moisture, irritant substances (such as detergents and soaps), and repeated trauma. Topical therapies include corticosteroids, antifungals, and calcineurin inhibitors. Intralesional corticosteroid injections have also been described as an option for more severe cases. Oral antifungal agents, especially fluconazole and itraconazole, are indicated when C. albicans involvement is confirmed or in refractory cases before proceeding with surgical intervention.1,2 However, conservative treatment is often ineffective, since fibrosis and progressive impairment of the vascular supply prevent drugs from reaching the nail folds, limiting treatment success.1
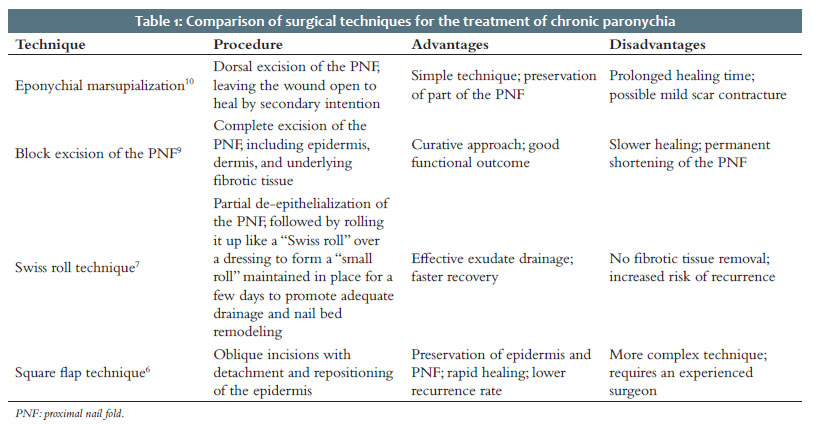
Nail surgery requires specific technical expertise and careful patient selection and is generally reserved for cases refractory to clinical management. Multiple surgical techniques for CP have been described over recent decades, each differing in complexity, recovery time, and aesthetic outcomes. The primary goal of surgery is to remove the fibrosis and adjacent chronically inflamed tissue, thus enabling cuticle regeneration and improved drug penetration.1,2,5 Table 1 summarizes the main surgical techniques.
Block excision of the PNF, proposed by Baran and Bureau in 1981, involves complete removal of the inflamed tissue, including the eponychium, through a wedge-shaped excision measuring 5-6 mm in width and extending from one lateral nail fold to the other. Although technically straightforward, this method may result in scar contracture and permanent deformities.1,5,9
Eponychial marsupialization, described by Keiser and Eaton in 1976, consists of crescent-shaped excision of the PNF while maintaining the eponychium intact. The excision area begins approximately 1 mm from the distal margin of the eponychium and extends proximally for about 6 mm. This technique facilitates drainage and reduces chronic inflammation but is associated with prolonged healing time and risk of recurrence.1,10
Another method indicated for the surgical management of CP is the "Swiss roll" technique. This approach involves partial de-epithelialization of the PNF, which is then rolled up like a "Swiss roll" over a dressing to form a "small roll" maintained in place for a few days. This maneuver promotes exudate drainage and facilitates nail bed remodeling. Despite its simplicity and relatively rapid recovery, this technique does not remove fibrotic tissue, which may predispose to recurrence in chronic cases.7
More recently, the square flap technique, developed by Ferreira Vieira d'Almeida et al. in 2016, has gained attention for enabling selective removal of fibrotic tissue while preserving the epidermis and nail matrix. This results in improved anatomical recovery, reduced healing time, and favorable functional and aesthetic outcomes. By preventing retraction of the PNF, the technique preserves nail plate length.1,2,6
The square flap technique allows excision of fibrotic tissue without complete removal of the PNF and lateral nail folds. Initially, oblique incisions measuring 4-5 mm in length are made on both sides of the PNF. An incision is then carefully made parallel to the epidermis, below the fibrotic tissue, to prevent damage to the nail matrix. The resulting square flap is elevated using forceps, and the fibrotic tissue is excised while preserving the PNF epidermis. The square flap is subsequently repositioned, and closure is achieved with simple interrupted sutures. Nail fold skin quality is of vital importance for the success of this technique.1,6
A retrospective study by Ferreira Vieira d'Almeida et al. involving 48 patients demonstrated promising results with the square flap technique, with significant clinical improvement in 95.6% of cases and a recurrence rate of only 4.4%.6 These findings support the role of surgical intervention as an effective option in refractory CP. Therefore, when properly performed, this technique yields excellent functional and cosmetic outcomes with a low recurrence rate. However, its complexity and execution time require a highly experienced surgeon, underscoring the importance of surgical expertise for optimal results.6
In addition to selecting an appropriate surgical technique, an individualized treatment plan and a close postoperative follow-up are essential to achieve favorable outcomes. In this context, biotin supplementation has gained attention as an adjuvant in nail regeneration, particularly due to its role in keratinization and strengthening of the nail plate, contributing to more effective and sustained functional recovery.7,8
The square flap technique is an effective and safe option for the treatment of refractory CP, providing both functional and aesthetic improvement with a low risk of complications and recurrence. This technique should be considered among treatment options when conservative treatment fails. Although technically more demanding, it offers several advantages, such as faster postoperative recovery, enabling earlier return to daily activities. Moreover, this technique preserves nail plate length, which is a major advantage in maintaining both nail appearance and function.
Clarissa Brito Farias
ORCID: 0009-0009-5395-045X
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
André Martins Ornelas
ORCID: 0009-0002-0393-7205
Preparation and writing of the manuscript, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Flauberto de Sousa Marinho
ORCID: 0000-0002-9337-9931
Approval of the final version of the manuscript, Conception and design of the study, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Relhan V, Bansal A. Acute and chronic paronychia revisited: A narrative review. J Cutan Aesthet Surg. 2022;15:1–16.
2. Srivastav Y, Shrivastava N, Kumar M. Paronychia: Its Diagnosis and Current Potential Treatment-based Management: Brief Schematic Review. Asian J Res Dermatol. 2023;6(1):112–120.
3. Davis DA, Hurt MA. Chronic paronychia: Modern diagnostic and therapeutic approaches. Clin Dermatol. 2021;39(1):53–9.
4. Yang JH, Kim MS, Shin JU. Chronic paronychia induced by epidermal growth factor receptor inhibitors. Int J Dermatol. 2020;59(2):e58–60.
5. Scher RK, Daniel CR III. Nails: Therapy, Diagnosis, Surgery. 4th ed. Elsevier Saunders; 2018.
6. Ferreira Vieira d'Almeida L, Papaiordanou F, Araújo Machado E, Loda G, Baran R, Nakamura R. Chronic paronychia treatment: Square flap technique. J Am Acad Dermatol. 2016;75(2):398–403.
7. Piraccini BM, Alessandrini A. Nutritional factors and hair loss. Clin Dermatol. 2021;39(1):52–60.
8. Trüeb RM. Nail disorders: What's new? J Dtsch Dermatol Ges. 2023;21(3):305–12.
9. Baran R, Bureau H. Surgical treatment of recalcitrant chronic paronychia of fingers. J Dermatol Surg Oncol. 1981;7:106–7.
10. Keiser JJ, Eaton RG. Surgical cure of chronic paronychia by eponychial marsupialization. Plast Reconstr Surg. 1976;58:66–70.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}