


Verônica Hamann Aita; Claudia Prócel; Nicoly de Souza Jacques; Fernando Eibs Cafrune
Funding: None
Conflict of interest: None
Submitted on: 06/15/2025
Final decision: 12/03/2025
How to cite this article: Aita VH, Jacques NS, Prócel C, Cafrune FE. Lip reconstruction using superficial flaps: functional and aesthetic integration. Surg Cosmet Dermatol. 2026;18(1):e20260480.
Mohs micrographic surgery is the preferred technique for the treatment of skin cancers involving the lip region. Reconstruction of surgical defects in this area is particularly complex, requiring preservation of anatomical structures, respect for cosmetic subunits, and maintenance of function whenever possible. This study describes 4 cases of lip surgical defects managed with different reconstructive techniques: mucosal rotation flaps, double V-Y advancement flaps, and O-Z rotation flaps. The choice of technique was individualized according to the location and size of the defect, aiming to achieve symmetry, preserve oral sphincter function, and obtain satisfactory aesthetic outcomes.
Keywords: Surgical Flaps; Mohs Surgery; Lip
The lips are a common site for skin cancer. Basal cell carcinoma (BCC) is the most frequent subtype affecting the upper lip, whereas squamous cell carcinoma (SCC) predominates in the lower lip.1,2 Surgical treatment is typically indicated, with Mohs micrographic surgery (MMS) providing superior margin control, greater tissue preservation, and lower recurrence rates.3,4
Nevertheless, reconstruction of surgical defects in the lip region remains challenging. The lips have limited tissue availability for primary closure, and their boundaries encompass multiple cosmetic subunits, increasing the risk of substantial distortion, facial asymmetry, and functional impairment.3,4
In this study, we describe 4 cases involving defects of the upper or lower lip that achieved favorable aesthetic and functional outcomes after reconstruction using mucosal rotation flaps, double V-Y advancement flaps, and double O-Z rotation flaps.
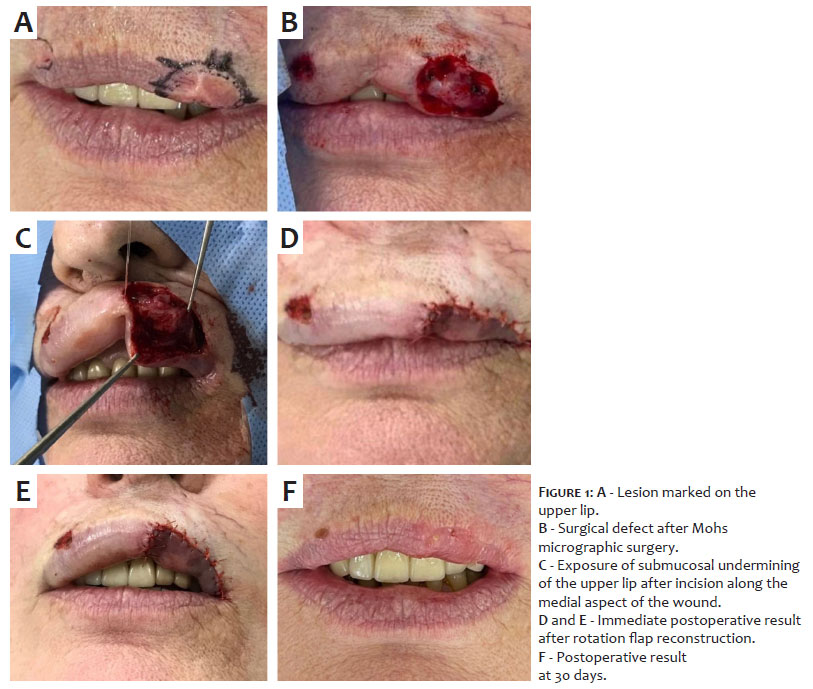
A 70-year-old woman was diagnosed with superficial BCC on the left upper lip and underwent MMS. The procedure resulted in a surgical defect measuring 16 x 11 mm in diameter after tumor-free margins were confirmed at the second stage. Reconstruction was performed using a rotation flap. This technique involved an incision along the medial aspect of the surgical defect, extending toward the inner labial mucosa. Submucosal undermining of the adjacent upper lip tissue was then performed to facilitate tissue mobilization and rotation. A Burow's triangle was excised, with its lateral limit at the labial commissure. The wound edges were approximated using 5-0 Vicryl sutures, selected for their flexibility and ability to promote optimal edge coaptation (Figure 1).
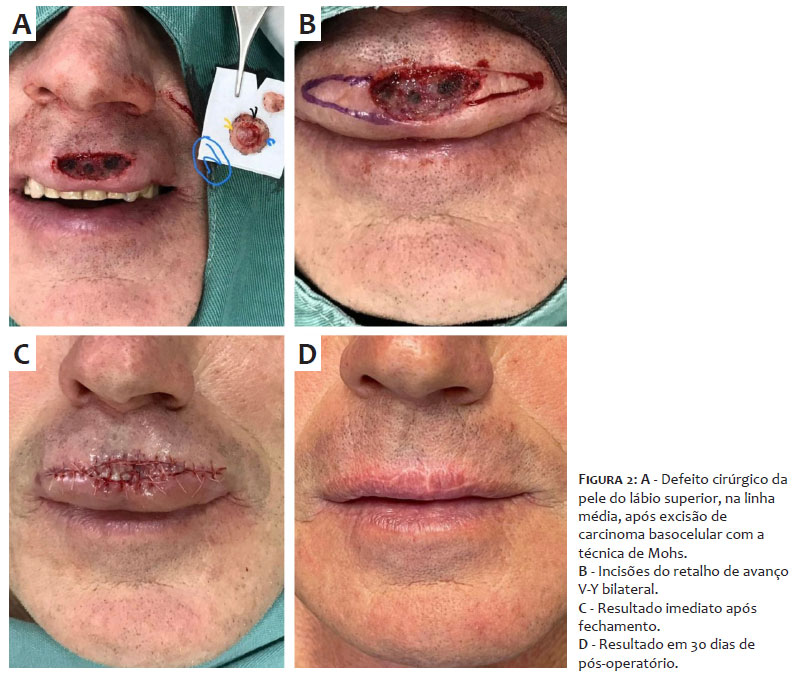
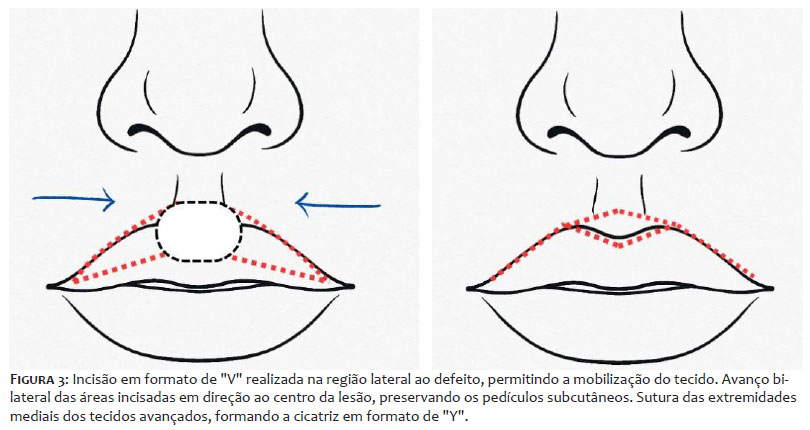
A 59-year-old man presented with nodular BCC located centrally along the vermilion border of the upper lip, measuring 9 x 10 mm in diameter. MMS was performed, achieving tumor-free margins at the first stage. Reconstruction was performed using a double V-Y advancement flap. A V-shaped incision was made adjacent and lateral to the defect, allowing mobilization with compatible tissue. Unlike the conventional approach, this procedure was performed bilaterally, followed by horizontal advancement of the incised areas toward the center of the initial defect while preserving subcutaneous pedicles to maintain adequate perfusion. Both advanced flaps were then sutured at their medial edges, and the margins of the donor sites were closed with linear edge-to-edge sutures, resulting in a bilateral Y-shaped scar (Figures 2 and 3).
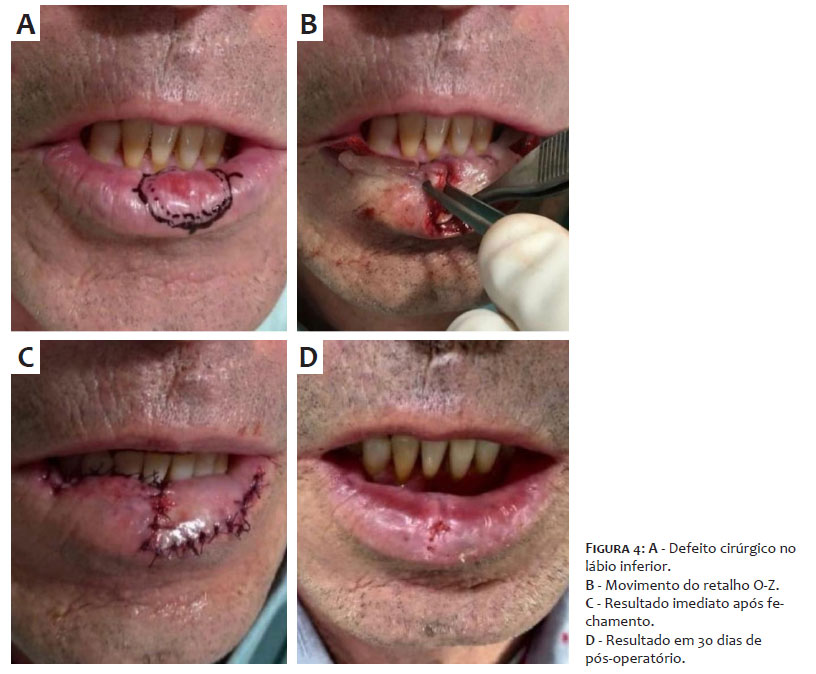
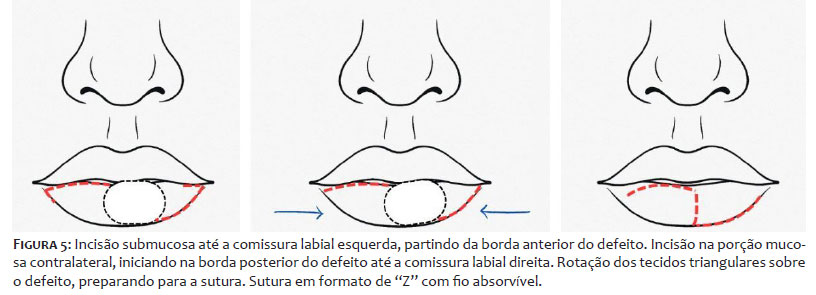
A 54-year-old man underwent MMS for invasive SCC located centrally on the vermilion border of the lower lip. After confirmation of tumor-free margins at the first stage, reconstruction was performed using a double O-Z rotation flap. An initial incision was made in the submucosal plane extending from the anterior border of the defect to the left labial commissure. A second incision was made on the contralateral side of the mucosa, extending from the posterior border of the defect to the right labial commissure. The 2 triangular flaps were then rotated over the defect and sutured in a Z configuration using 4-0 Vicryl (Figures 4 and 5).
CASE 4
A 68-year-old man presented with moderately differentiated SCC located in the vermilion border of the left lower lip. Tumor excision was performed using a conventional surgical approach. Reconstruction was performed using a mucosal rotation flap. An incision was made along the medial aspect of the surgical defect on the lower lip, extending toward the inner mucosa. Submucosal undermining of the perilesional tissue was performed to allow adequate coverage of the defect. To compensate for tissue rotation and prevent redundancy, a lateral triangular excision was performed up to the labial commissure. The mobilized tissue was then rotated anteriorly and sutured using 5-0 Vicryl (Figure 6).
MMS with complete margin control not only achieves significant cure rates but also allows for maximal tissue preservation for reconstruction. Reconstruction of surgical defects from skin cancer involving the lip region remains technically challenging due to the limited tissue availability and the high risk of functional impairment. Microstomia and sensory innervation may occur, leading to changes in aesthetic perception, mastication, and speech articulation.3
Some reconstructive options have been described for this anatomical site, including healing by secondary intention, primary closure, or wedge excision. Although these approaches are less complex and may yield satisfactory outcomes in selected cases, they carry an increased risk of unpredictable results, such as scar contracture and eclabium.1
Mucosal advancement flaps are most commonly reserved for superficial reconstructions of the vermilion border.5 However, this technique has inherent limitations, including varying degrees of contracture and cosmetic distortion due to differences in color and texture between the labial mucosa and vermilion border.6 Additionally, increased dryness and occasional lip sensory loss have been reported.7
The mucosal rotation technique, as described in cases 1 and 4, tends to mitigate these drawbacks. In this approach, only the medial portion of the defect is rotated and advanced anteriorly, preserving the lateral mucosal tissue, from which only a Burow's triangle is excised to facilitate proper edge alignment.
Another technique, less commonly described in the literature — typically used for scalp reconstruction but effective in various anatomical regions — is the double O-Z rotation flap, as detailed in case 3. This method involves incisions that create 2 triangular flaps, which are repositioned and sutured in a Z configuration. This design minimizes traction on mucosal tissue while preserving lip volume.
Bilateral advancement flaps are indicated for larger defects of the upper lip, particularly those extending beyond the boundaries of the philtrum and compromising the mucocutaneous junction, or in cases where the natural curvature of the philtrum has been lost due to age-related lip atrophy.8 Unilateral V-Y advancement flaps, based on a subcutaneous pedicle, are suitable for lateral upper lip defects larger than 1 cm, whereas bilateral V-Y advancement flaps are recommended for central lip defects.1 In case 2, a double V-Y advancement flap was selected to allow mobilization of adjacent tissue with optimal compatibility in color, texture, and thickness. The technique provided adequate defect coverage, restoring anatomical symmetry and function while preserving the oral sphincter without the need for muscle transposition, which would be difficult to achieve with other reconstructive techniques.
Multiple techniques have been described for lip reconstruction after MMS. The choice of technique depends on the size and depth of the defect, as well as the aggressiveness and histologic subtype of the tumor, with the overarching goal of preserving anatomical boundaries and aesthetic subunits.
Primary closure should be reserved for smaller defects in selected cases. Mucosal rotation and double O-Z rotation flaps appear more favorable than mucosal advancement techniques due to superior preservation of lip tissue, resulting in reduced aesthetic and functional impairment. In contrast, double V-Y advancement flaps contribute to maintaining lip symmetry and preserving neural and sphincter function.
Therefore, selecting the most appropriate reconstructive technique requires comprehensive anatomical knowledge, surgical expertise, and continuous updating based on techniques described in the literature.
Verônica Hamann Aita
ORCID: 0000-0002-5746-1970
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Nicoly de Souza Jacques
ORCID: 0009-0009-3799-1497
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Claudia Prócel
ORCID: 0009-0009-6006-8326
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Fernando Eibs Cafrune
ORCID: 0000-0002-6645-0122
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
1. Chellapan B; Obanigba G; Hoyer P; Ross L. Lip Reconstruction After Mohs Micrographic Surgery: A Guide on Flaps. Cutis. 2023;111(4):205-9.
2. Goldman A, Wollina U, França K, Lotti T, Tchernev G. Lip repair after Mohs surgery for squamous cell carcinoma by bilateral tissue expanding vermillion myocutaneous flap (Goldstein technique modified by Sawada). Open Access Maced J Med Sci. 2018;6(1):93–5.
3. Ubaldo HDC, Frey MN, Dellatorre G. Emprego do retalho de avanço em ilha (V-Y) na reconstrução labial após cirurgia micrográfica de Mohs: relato de três casos. Surg Cosmet Dermatol. 2019;11(3):248–51.
4. Cerci FB, Kubo EM. Retalho de rotação para reconstrução de lábio cutâneo superior após cirurgia micrográfica de Mohs. An Bras Dermatol. 2010;85(5):680–3.5. Baker SR. Retalhos Locais na Reconstrução Facial. 4th ed. São Paulo: Di Livros; 2022.
5. Eirís N, Suarez-Valladares MJ, Blanco HAC, Rodríguez-Prieto, MA. Bilateral mucosal rotation flap for repair of lower lip defect. J Am Acad Dermatol 2015;72:e81-2.
6. Rohrer TE, Cook JL, Kaufman AJ. Flaps and Grafts in Dermatologic Surgery. 2nd ed. Philadelphia: Elsevier; 2017.
7. Kaufman AJ, Grekin RC. Bilateral advancement flaps for upper lip reconstruction. In: Roenigk RK, Roenigk HH, editors. Dermatologic Surgery. Principles and Practice. 2nd ed. New York: Marcel Dekker; 1996. p. 617–22.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}