


Diana Coello Bonilla1; Giovanna Gelli Carrascoza1; Gabrielle Cassulo Franciscatti2; Maria Victória Quaresma1
Funding: None
Conflict of interest: None
Submitted on: 02/25/2025
Final decision: 12/30/2025
How to cite this article: Bonilha DC, Carrascoza GG, Franciscatti GC, Quaresma MV. Trichotemnomania in androgenetic alopecia: a case report. Surg Cosmet Dermatol. 2026;18(1):e20260443.
Trichotemnomania is a rare, underrecognized obsessive-compulsive disorder characterized by repetitive cutting of hair. Its clinical presentation may mimic other hair disorders, often leading to misdiagnosis and unnecessary treatments. We report the case of a 25-year-old man presenting with scalp hair thinning. Trichoscopy revealed areas of miniaturized hairs with heterogeneous shaft diameters, consistent with androgenetic alopecia, adjacent to irregular patches of uniformly short hairs with blunt ends, suggestive of mechanical trimming. Detailed history-taking confirmed the coexistence of trichotemnomania, supported by the patient's report of recurrent and deliberate use of a razor to cut his hair.
Keywords: Alopecia; Hair Diseases; Obsessive-Compulsive Disorder
Trichotemnomania is an obsessive-compulsive behavior characterized by recurrent cutting of hair using scissors or a razor.1 The term derives from the Greek thrix (hair), temnein (to cut), and mania (madness). This rare and often underrecognized condition presents as self-induced alopecia resulting from habitual cutting or shaving. Although not entirely voluntary, the behavior is typically driven by an urge to relieve stress, and patients may be reluctant to disclose it.2
Due to its limited recognition in dermatologic practice, trichotemnomania is frequently misdiagnosed as alopecia, particularly alopecia areata or trichotillomania.3 It may occur as an isolated condition or in association with other hair disorders.
We report a case of trichotemnomania associated with androgenetic alopecia (AGA), highlighting its clinical, trichoscopic, and histopathologic characteristics and emphasizing the importance of considering this entity in the differential diagnosis of alopecia.
A 25-year-old man with a prior diagnosis of acute lymphocytic leukemia, treated with bone marrow transplant 6 years earlier, presented with a 2-year history of progressive hair loss without identifiable causes or associated symptoms.
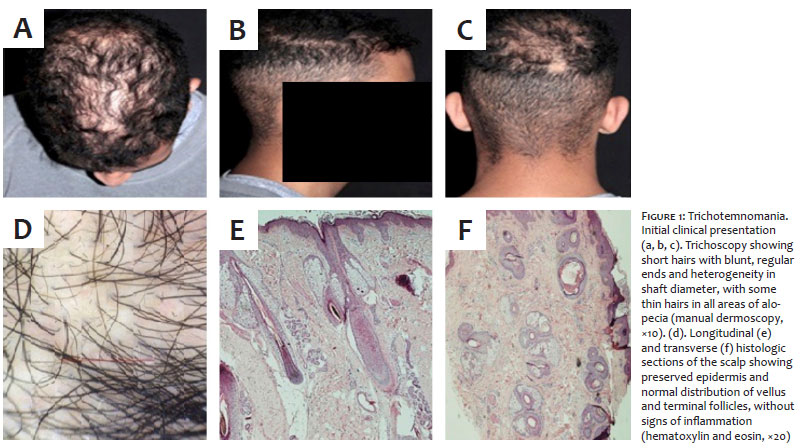
Dermatologic examination revealed areas of non-scarring alopecia with hair thinning in the vertex and frontal regions, accompanied by irregular, sharply demarcated patches in the biparietal and occipital regions. The scalp surface appeared normal, and the hair-pull test was negative (Figure 1a–c).
Trichoscopy revealed miniaturized hairs and heterogeneous shaft diameters, consistent with AGA. In addition, short hairs of uniform length with blunt ends were observed, suggesting a coexisting mechanical trimming process. No broken hairs, black dots, or signs of perifollicular inflammation were identified (Figure 1d).
Laboratory tests, including HIV and syphilis serologies, yielded negative results. Histopathologic examination of an occipital scalp biopsy showed preserved epidermal architecture, with both terminal and vellus hair follicles and no evidence of inflammation, fibrosis, or scarring (Figure 1e–f).
During subsequent evaluations, the patient reported the use of synthetic products to conceal areas of alopecia and admitted to frequent shaving with a razor, as well as the use of hair-coloring products. The clinical, histopathologic, and trichoscopic findings supported the diagnosis of trichotemnomania superimposed on AGA.
The patient was advised to discontinue shaving until re-evaluation. At a 3-week follow-up visit, increased hair density was observed in the previously affected areas, further supporting the diagnosis of trichotemnomania (Figure 2). The patient did not return for subsequent dermatologic follow-up.
Trichotemnomania is a rare disorder within the obsessive-compulsive spectrum, characterized by recurrent cutting or shaving of one's own hair, typically as a coping mechanism for psychological distress.1 Although the scalp is most commonly affected, involvement of the eyebrows, eyelashes, axillae, and pubic region has also been reported.4 Because the behavior may be partially involuntary or unacknowledged, patients frequently deny or are unaware of its self-induced nature, contributing to underdiagnosis.
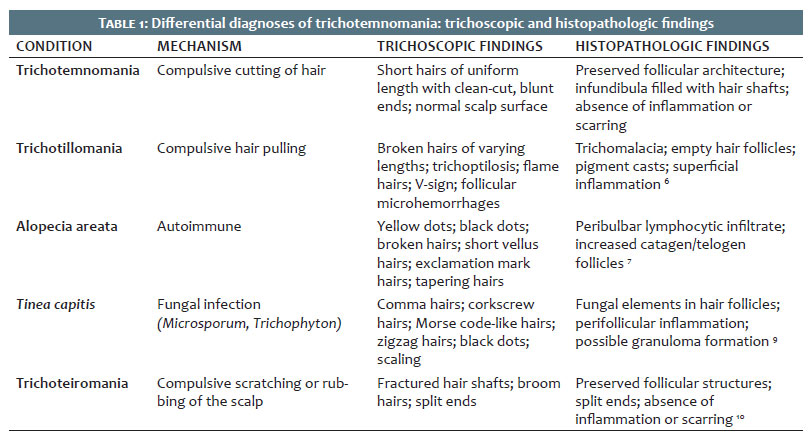
The condition is often misdiagnosed as trichotillomania, alopecia areata, or tinea capitis.2 Table 1 summarizes the main differential diagnoses of trichotemnomania.
Diagnosis relies on the integration of clinical, trichoscopic, and histopathologic findings. Clinically, trichotemnomania presents as sharply demarcated patches containing short hairs of uniform length with blunt, evenly cut ends, while the scalp surface remains normal, without erythema, scaling, or follicular damage.1
Trichoscopy plays a central role in the investigation of trichotemnomania. It reveals hair shafts with clean-cut ends and uniform length, consistent with mechanical trimming rather than follicular destruction. These findings contrast with the irregular shaft fractures, trichoschisis, and trichoptilosis seen in trichotillomania, as well as with the exclamation mark hairs, yellow dots, and black dots typically observed in alopecia areata.5
Histopathologically, in trichotemnomania, scalp biopsy demonstrates preserved follicular architecture, with all infundibula filled with hair shafts and absence of inflammation, fibrosis, or scarring.1 This contrasts with the histopathology of trichotillomania, which may show empty hair follicles, hair follicle involution (catagen), and traumatic changes,6 and of alopecia areata, which typically exhibits peribulbar lymphocytic infiltrate.7
In the present case, trichotemnomania coexisted with AGA. In AGA, androgen-mediated follicular miniaturization occurs in genetically susceptible follicles, leading to the progressive transformation of terminal follicles (producing thick, pigmented hairs) into vellus follicles (producing thin, short hairs). This results in the heterogeneity of hair shafts at different stages of disease progression.8 Trichotemnomania does not alter this process but superimposes uniformly cut hairs onto this background, potentially complicating diagnosis.
Management of trichotemnomania requires a multidisciplinary approach involving dermatologists, psychiatrists, and psychologists, since the behavior is often associated with stress, anxiety, or obsessive-compulsive disorders. Patient education, stress management, and behavioral therapy are essential to prevent recurrence.
Given its frequent underdiagnosis, trichotemnomania should be considered by dermatologists in the differential diagnosis of patients presenting with patchy hair thinning, preserved follicular openings, and uniformly cut hairs, particularly when trichoscopic and histopathologic findings are inconsistent with alopecia areata or trichotillomania. Importantly, trichotemnomania may coexist with other hair disorders, further complicating the clinical picture. Early recognition is essential to avoid unnecessary interventions and to ensure timely psychological support and follow-up.
Diana Coello Bonilla
ORCID: 0009-0005-6503-082X
Preparation and writing of the manuscript, Critical review of the literature.
Giovanna Gelli Carrascoza
ORCID: 0009-0002-6431-6090
Preparation and writing of the manuscript, Critical review of the literature.
Gabrielle Cassulo Franciscatti
ORCID: 0009-0007-7216-0045
Critical review of the literature, Critical revision of the manuscript.
Maria Victória Quaresma
ORCID: 0000-0003-2891-1650
Conception and design of the study, Effective participation in the conduct of the study, Critical review of the literature.
1. Happle R. Trichotemnomania: obsessive-compulsive habit of cutting or shaving the hair. J Am Acad Dermatol. 2005;52(1):157-9.
2. Mutluer T, Ateş B, Nasıroğlu S, Eray Ş. Three adolescent cases of a very rare disorder: Trichotemnomania. Psychiatry Clin Psychopharmacol. 2019;29(3):212-5.
3. Gallouj S, Rabhi S, Baybay H, Soughi M, Meziane M, Rammouz I, et al. Trichotemnomanie associée à une trichotillomanie: intérêt diagnostique de la dermoscopie. Ann Dermatol Venereol. 2011;138(3):140-1.
4. Thadchanamoorthy V, Thirukumar M, Dayasiri K, Thamilvannan N, Jeyakumar J. Trichotemnomania in an adolescent girl: a case report of an Asian child and literature review. Case Rep Dermatol Med. 2020;2020:6615250.
5. Rudnicka L, Rakowska A, Kerzeja M, Olszewska M. Hair shafts in trichoscopy: clues for diagnosis of hair and scalp diseases. Dermatol Clin. 2013;31(4):695-708.
6. Bergfeld W, Mulinari-Brenner F, McCarron K, Embi C. The combined utilization of clinical and histological findings in the diagnosis of trichotillomania. J Cutan Pathol. 2002;29(4):207-14.
7. Al-Dhubaibi MS, Alsenaid A, Alhetheli G, Abd Elneam AI. Trichoscopy pattern in alopecia areata: a systematic review and meta-analysis. Skin Res Technol. 2023;29(6):e13378.
8. Liu Y, Tosti A, Wang ECE, et al. Androgenetic alopecia. Nat Rev Dis Primers. 2025;11(1):73.
9. Waśkiel-Burnat A, Rakowska A, Sikora M, Ciechanowicz P, Olszewska M, Rudnicka L. Trichoscopy of tinea capitis: a systematic review. Dermatol Ther (Heidelb). 2020;10(1):43-52.
10. Freyschmidt-Paul P, Hoffmann R, Happle R. Trichoteiromania. Eur J Dermatol. 2001;11(4):369-71.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}