


Sarah de Oliveira Mendes; Thamires Alcântara Bezerra de Assis; Ana Beatriz Araújo Leite; Conceição Virgínia Costa Batista
Funding: None
Conflict of interest: None
Submitted on: 07/16/2025
Final decision: 08/26/2025
How to cite this article: Mendes SO, Assis TAB, Leite ABA, Batista CVC. Facial rosacea outside the nasal region: Case report and surgical approach. Surg Cosmet Dermatol. 2025;17:e20250495.
Rosacea is a chronic inflammatory skin disease that can manifest with isolated phymatous alterations. This case report describes the case of a patient with a rare and exuberant clinical presentation, successfully treated with a conventional surgical approach.
Keywords: Rosacea; Surgical Procedures, Operative; Dermatology
Rosacea is a chronic inflammatory dermatosis affecting approximately 2% to 22% of the world population.1 Its etiology involves neurovascular and immune alterations, as well as individual environmental triggers.2 Skin lesions predominantly occur in the centrofacial region and are characterized by recurrent episodes of flushing, persistent erythema, papules, pustules, and telangiectasias.3,4 Phymatous changes correspond to facial skin thickening due to fibrosis and/or sebaceous glandular hyperplasia. They most commonly affect the nose,3,5 but may also be found in other regions, such as forehead, chin, and ears.4
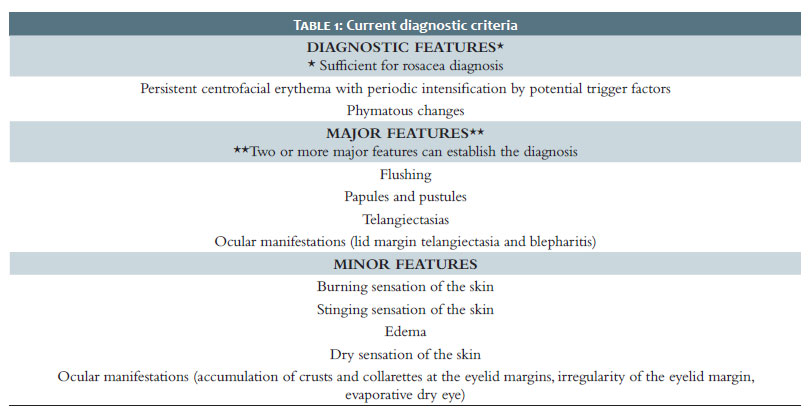
Consensus diagnostic criteria have evolved from a morphological classification into a phenotype-based system (Table 1). However, rosacea remains a clinically diagnosed disease where phymatous changes are considered pathognomonic.3,2
The phymatous form is a rare manifestation, and there are few case reports of facial rosacea sparing the nasal region.6 The goal of this study is to present a rare and exuberant case of phymatous rosacea as well as the outcomes of a surgical approach to treatment.
A 67-year-old male patient residing in the metropolitan area of Recife presented with progressive and additive lesions on the face and ears for approximately 40 years. He reported a history of previous surgical procedures on some lesions, without relapse, but did not provide any information on the techniques used.
Dermatological examination revealed erythematous, infiltrative plaques located in the malar and glabellar regions and on the auricular lobules; scars from previous excisions on the forehead and mandibular angle; and atrophic scars on the chin, residual from acne (Figure 1).
Histopathological examination of the left malar region found chronic perifolliculitis associated with cicatricial fibrosis, findings consistent with rosacea. Based on clinical and histopathological evaluation, a diagnosis of an uncommon presentation of phymatous rosacea was established, characterized by exuberant lesions and facial involvement sparing the nasal region.
The surgical approach chosen used tangential excision with a cold scalpel and a No. 15 blade, followed by refinement with an electric scalpel available in the operating room (20 watts). A straight electrode tip was used to correct surface irregularities and to perform gentle coagulation of bleeding points. In the glabellar region, an advancement flap had been planned; however, local skin laxity allowed approximation of the wound edges and primary closure, making the flap unnecessary. In the malar region, healing by secondary intention was adopted. The postoperative course was uneventful, and the post-inflammatory erythema had resolved completely at follow-up in 2025.
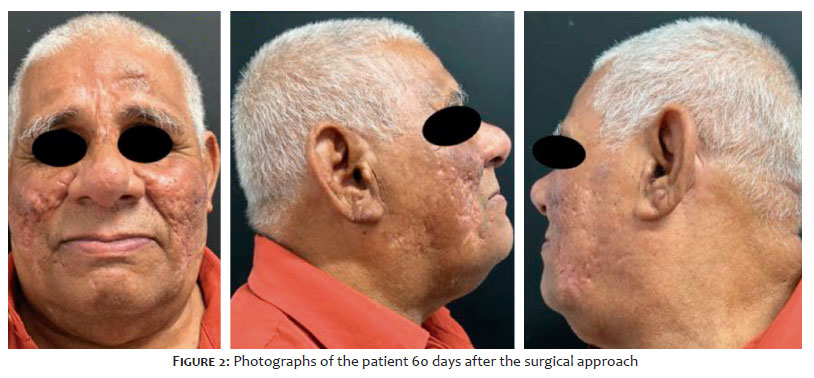
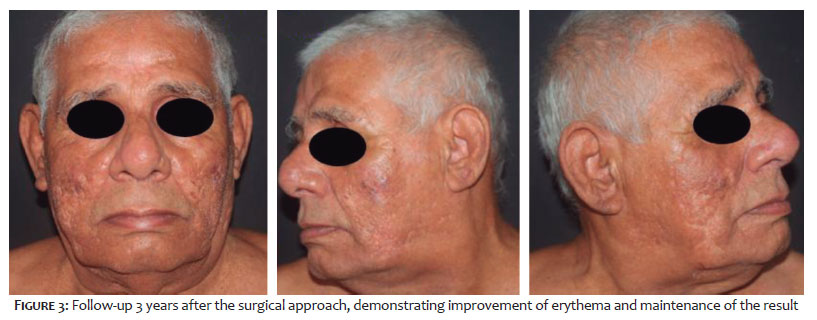
The aesthetic outcome of the first procedure was considered excellent, with a considerable reduction in facial tumors and skin surface irregularities (Figure 2). Regression of postoperative erythema was observed 3 years after the intervention, with no lesion relapse and sustained patient satisfaction, who reported an improvement in quality of life (Figure 3). Therefore, no further therapeutic interventions were required.
Although phymatous rosacea is a benign condition, it may cause functional and aesthetic impairment, requiring a therapeutic approach.1,2 Clinical treatment options include the use of isotretinoin and tetracyclines for inflammatory forms of the disease. For fibrotic lesions, however, optimal treatment involves removal of the lesion without damage to adjacent structures and skin appendages.1,2
Several methods have been described and employed in the treatment of fibrotic forms, with reports of excisional surgical procedures dating back to the 17th century. Even so, there is still no universally accepted treatment method for the condition, with excisional surgical approaches and ablative lasers predominating in the medical literature. The most frequently reported methods include conventional surgery, electrosurgery, cryosurgery, and radiofrequency. Among ablative techniques, CO2 lasers (10,640 nm) and Er:YAG (erbium-doped yttrium–aluminum–garnet) lasers (2,940 nm) stand out. 1,2
There are no studies demonstrating the superiority of one technique over another, and given the wide range of therapeutic options available, each patient should be assessed individually to select the most appropriate method, taking into consideration factors such as accessibility, availability, and patient-specific characteristics in order to determine the best risk-benefit balance.2
The patient described in this report showed both aesthetic and functional improvement, with no postoperative complications, demonstrating that a conventional surgical approach can be effective even in uncommon presentations of phymatous rosacea.
Sarah de Oliveira Mendes
ORCID: 0009-0006-0319-1860
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature.
Thamires Alcântara Bezerra de Assis
ORCID: 0000-0002-8017-9906
Author’s contribution: Approval of the final version of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Ana Beatriz Araújo Leite
ORCID: 0000-0003-0027-6720
Author’s contribution: Approval of the final version of the manuscript, Acquisition, analysis and interpretation of data.
Conceição Virgínia Costa Batista
ORCID: 0000-0002-3724-8742
Approval of the final version of the manuscript, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Fink C, Lackey J, Grande DJ. Rhinophyma: a treatment review. Dermatol Surg. 2018;44(2):275-82.
2. Oliveira CMM, Almeida LMC, Bonamigo RR, Lima CWG, Bagatin E. Consensus on the therapeutic management of rosacea – Brazilian Society of Dermatology. An Bras Dermatol. 2020;95(Suppl 1):53–69.
3. Schaller M, Almeida LMC, Bewley A, Cribier B, Del Rosso J, Dlova NC. Recommendations for rosacea diagnosis, classification and management: update from the global rosacea consensus 2019 panel. Br J Dermatol. 2020;182(5):1269-76.
4. Suzuki NN, Palo JS, Magalhães RF, Buffo TH, Stolf HO. Full thickness cross-shaped excision for rhinophyma in a patient with multiple comorbidities. Surg Cosmet Dermatol. 2020;12(Suppl 1):124–7.
5. Tan J, Almeida LMC, Bewley A, Cribier B, Dlova NC, Gallo R. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global rosacea consensus (ROSCO) panel. Br J Dermatol. 2017;176(2):431-8.
6. Van Zuuren EJ, Arents BWM, van der Linden MMD, Vermeulen S, Fedorowicz Z, Tan J. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22(4):457-65.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}