


Camila Medyk; Victória Prudêncio Ferreira; Milene Cripa Pizzato de Araújo; Rogerio Nabor Kondo; Cássio Rafael Moreira
Funding: None
Conflict of interest: None
Submitted on: 04/25/2025
Final decision: 07/13/2025
How to cite this article: Medyk C, Ferreira VP, Araújo MCP, Kondo RN, Moreira CR. Giant atypical fibroxanthoma on thoracic trunk: a case report. Surg Cosmet Dermatol. 2025;17:e20250466.
O fibroxantoma atípico (FXA) é um tumor mesenquimal raro que geralmente acomete pacientes com idade avançada, do sexo masculino, em áreas fotoexpostas. É mais frequente na cabeça e pescoço, mas também pode ocorrer no tronco e nas extremidades. Atualmente, é considerado um tumor benigno de diagnóstico por exclusão, com baixa taxa de recidiva e metástase. O tratamento é realizado com excisão cirúrgica, o que permite o diagnóstico por avaliação histológica e imuno-histoquímica.
Keywords: Tórax; Oncologia Cirúrgica; Dermoscopia; Neoplasias; Imuno-Histoquímica; Sarcoma
Atypical fibroxanthoma (AFX) is a rare mesenchymal tumor that typically affects elderly male patients in sun-exposed areas.1 It is more frequently found on the head and neck, but may also occur on the trunk and extremities.1 It is currently regarded as a benign tumor diagnosed by exclusion, with a low rate of recurrence and metastasis.2 Treatment is performed by surgical excision, which allows for diagnosis by histological and immunohistochemical evaluation.1
A 72-year-old male patient presented with a vegetative lesion on the anterior trunk for 6 months, which had progressed with rapid growth, ulceration, and recurrent episodes of bleeding. He also reported local pain and pruritus.
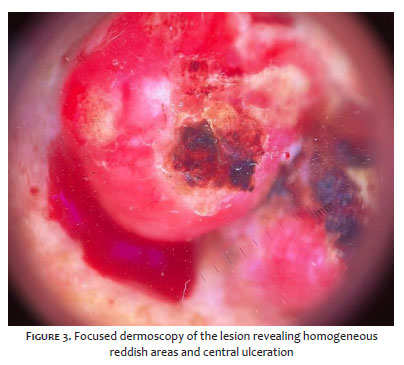
Physical examination revealed an exophytic lesion with an irregular surface, erythematous-violaceous in color, friable and exudative, located on the anterior thorax, measuring approximately 6 cm at its greatest diameter (Figures 1 and 2). Focused dermoscopy showed homogeneous reddish areas and central ulceration (Figure 3). The patient also exhibited marked photoaging, as well as lesions suspected to be basal cell carcinoma on the cervical region, a diagnosis confirmed after excision.
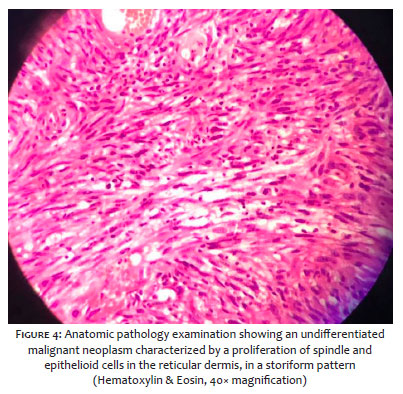
An excisional biopsy of the anterior trunk lesion was performed on the same day of the visit. Histopathological examination showed an atypical proliferative lesion, ulcerated, composed of spindle cells arranged in a storiform pattern, involving the dermis, with a high mitotic index and free surgical margins (Figure 4). The adjacent dermis showed marked elastosis. Immunohistochemical analysis was positive for CD10 and negative for SOX-10, cytokeratins, p40, ERG, Melan-A, desmin, S-100, and CD34.
The patient has shown good postoperative wound healing and remains under follow-up in our clinic.
In general, AFX presents as a possibly ulcerated single lesion measuring less than 2-3 cm.3,4 It is more frequent in elderly patients, but cases in younger individuals have been reported.4 The association with sun exposure is well documented, with mutations in the p53 gene.4,5 Pigmented variants exist, and a differential diagnosis with melanoma is required due to hemosiderin deposition.4 Dermoscopy is nonspecific, showing homogeneous reddish areas with possible ulceration. The mean time to diagnosis reported in the literature is 3 months after lesion onset.2
Histology shows a well-circumscribed dermal neoplasm composed of histiocytoid, epithelioid, spindle-shaped, and multinucleated giant cells arranged in a storiform pattern,1 demonstrating exophytic, nodular, or polypoid growth. AFX is a diagnosis of exclusion; squamous cell carcinoma, spindle cell carcinoma, desmoplastic melanoma, poorly differentiated leiomyosarcoma, and angiosarcoma must be ruled out with the aid of immunohistochemistry. The neoplasm exhibits strong CD10 positivity and negativity for S100, cytokeratin, and vascular markers (such as CD34 and CD31),1 and may be positive for CD68, CD99, CD163, and vimentin.5
More recent studies consider AFX and pleomorphic dermal sarcoma to be part of a single spectrum. Both share similar epidemiological, histological, and immunohistochemical features, but differ in clinical behavior and aggressiveness. The sarcoma typically presents as a larger, thicker, and deeper tumor at diagnosis, with lymphatic, vascular, and perineural invasion, as well as necrotic areas, and carries a higher risk of relapse and metastasis.1,2
The recommended treatment is complete excision of the lesion with safety margins. Clinical follow-up every 3 to 6 months during the first 3 years is recommended, especially for higher-risk patients.3,5
This article reports a rare case of AFX in an elderly patient with marked photoaging who presented with a larger-than-average lesion on the trunk at diagnosis. It is possible that these features were related to delayed access to specialized dermatologic care, which was 6 months, longer than the average reported in the literature. Treatment was initiated on the day of the visit, and the presence of ulceration and lesion size prompted further evaluation, including chest CT to rule out metastases, in line with more recent studies that consider this neoplasm part of the spectrum of pleomorphic dermal sarcomas.
Camila Medyk
ORCID: 0009-0000-3491-5813
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Victória Prudêncio Ferreira
ORCID: 0000-0001-9642-5940
Approval of the final version of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Milene Cripa Pizzato de Araújo
ORCID: 0000-0001-8749-2586
Statistical analysis, Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Cássio Rafael Moreira
ORCID: 0000-0002-8781-1505
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical revision of the manuscript.
1. Iglesias-Pena N, Martínez-Campayo N, López-Solache L. Relation between atypical fibroxanthoma and pleomorphic dermal sarcoma: histopathologic features and review of the literature. Actas Dermo-Sifiliográficas (English Edition). 2021;112(5):392–405.
2. Ríos-Viñuela E, Pons Benavent M, Monteagudo C, Nagore E, Sanmartín O. Fibroxantoma atípico y sarcoma pleomórfico dérmico: estúdio bicéntrico retrospectivo de 74 casos. Actas Dermo-Sifiliográficas. 2022;113(6):654–6.
3. Jara N, Solé Z S. Fibroxantoma atípico. Caso clínico. Revista médica de Chile. 2019;147(10):1346–9.
4. De la Fuente EG, Sols M, Pinedo F, Álvarez-Fernández JG, Vicente FJ, Naz E, et al. Fibroxantoma atípico. Estudo clinicopatológico de 10 casos. Actas Dermo- Sifiliográficas. 2005;96(3):153–8.
5. Iorizzo LJI, Brown MD. Atypical Fibroxanthoma: a Review of the Literature. Dermatol Surg. 2011;37(2):146–57.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}