


Nicole Russell1; Siddharth Srikakolapu2; Jane Scribner2
Funding: None.
Conflict of interest: None.
Submitted on: 09/22/2024
Final decision: 01/30/2025
How to cite this article: Russel N, Srikakolapu S, Scribner J. A case of kidney transplant rejection secondary to cemiplimab for recurrent cutaneous squamous cell carcinoma. Surg Cosmet Dermatol. 2025;17:e20250409.
We report a case involving a 71-year-old male with a history of kidney transplant on immunosuppressive therapy and non-melanoma skin cancers who developed persistent lesions on the cheek and forehead after multiple skin cancer treatments. Biopsies identified poorly differentiated cutaneous squamous cell carcinoma. The patient underwent excisional salvage therapy with flap reconstruction, complicated by infection requiring debridement. He subsequently presented with in-transit dermal metastases and began treatment with cemiplimab. Unfortunately, after two cycles, he faced graft rejection and transitioned to hemodialysis. A recent PET-CT revealed no evaluable disease, and there were no clinical signs of recurrence at his last follow-up.
Keywords: Programmed Cell Death 1 Receptor; Carcinoma, Squamous Cell; Graft Rejection; Kidney Diseases.
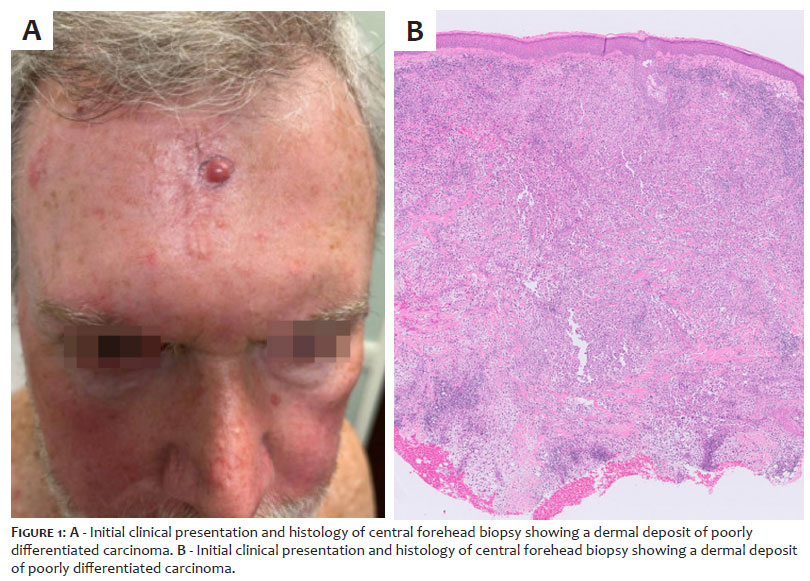
A 71-year-old male with a history of kidney transplant secondary to IgA nephropathy on tacrolimus and prednisone and multiple non-melanoma skin cancers, treated with photodynamic therapy, 5-fluorouracil, and Mohs surgery, presented to dermatology clinic with non-healing lesions of the left cheek and central forehead adjacent to previous Mohs scars. Examination revealed a scaly papule with an erythematous base on the left cheek and left forehead, a reddish-purple papule adjacent to a scar on the central forehead, and an ulcerated violaceous papule adjacent to a scar on the left anterior cheek/temple region.
Previous biopsies from the sites of concern found moderately well-differentiated squamous cell carcinoma. Biopsies obtained during the current visit revealed dermal deposition of poorly differentiated cutaneous squamous cell carcinoma extending to deep and peripheral margins. Special stains were positive for P63 and CD10 and negative for desmin and SOX-10 (Figure 1A and 1B).
In addition, the central forehead lesion had special stains positive for CK903, P40/CK 5/6, GATA-3, and PAX-8. The patient was diagnosed with recurrent locally aggressive cutaneous squamous cell carcinoma (T1N0M0) induced by post-transplant immunosuppressive therapy. He subsequently underwent excisional salvage therapy and local flap reconstruction. The postoperative course was complicated by skin graft wound healing and deterioration. Bacterial cultures grew Serratia marcescens resistant to augmentin, and the patient completed a course of Bactrim with concurrent wound debridement. The patient was found to have progressive gross residual in-transit dermal metastases at the graft site, for which cemiplimab was initiated (Figure 2). Initiation of cemiplimab required discontinuation of tacrolimus and initiation of sirolimus. The patient received two cycles of cemiplimab. Unfortunately, the patient presented to the emergency department with graft rejection secondary to cemiplimab. The patient was placed on hemodialysis and cemiplimab was discontinued. A recent PET-CT scan revealed no obviously evaluable disease. The patient had no clinical signs of recurrence at his most recent follow-up visit (Figure 3).
Solid organ transplant recipients receiving chronic immunosuppression therapy have a markedly increased risk of developing cutaneous squamous cell carcinoma, accounting for 40% of all malignancies in organ transplant recipients. Cemiplimab is a monoclonal antibody directed at PD-1 which has shown significant responses in patients with locally advanced or metastatic cutaneous squamous cell carcinoma and has become a mainstay of treatment. Hanna et al. report that no kidney allograft rejection events were observed during a phase I study of cemiplimab for kidney transplant recipients with advanced cutaneous squamous cell carcinoma when used in combination with pulsed-dose corticosteroids and mTOR inhibitors. Cui et al. report that solid organ transplant rejection rates may be as high as 40% with anti PD-L1 agent monotherapy and suggest PD-L1 positive expression in graft biopsy may be an effective marker for predicting transplant rejection.
Nicole Russell
ORCID: 0009-0009-3745-6902
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature
Siddharth Srikakolapu
ORCID: 0000-0002-2606-1042
Approval of the final version of the manuscript, Preparation and writing of the manuscript
Jane Scribner
ORCID: Aguardando!
Approval of the final version of the manuscript
1. Hanna GJ, Dharanesswaran H, Giobbie-Hurder A, Harran JJ, Liao Z, Pai L, et al. Cemiplimab for kidney transplant recipients with advanced cutaneous squamous cell carcinoma. J Clin Oncol. 2024;42(9):1021-30.
2. Cui X, Yan C, Xu Y, Li D, Guo M, Sun L, et al. Allograft rejection following immune checkpoint inhibitors in solid organ transplant recipients: a safety analysis from a literature review and a pharmacovigilance system. Cancer Med. 2023;12(5):5181-94.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}