


Rasha Aoun; Dalia Hossam; Ahmed Sadek; Shaimaa Farouk
Funding: None
Conflict of interest: None
Submitted on: 12/18/2024
Final decision: 03/20/2025
How to cite this article: Aoun R, Hossam D, Sadek A, Farouk S. Assessing the impact of anti-nuclear antibodies on the severity and types of vitiligo: a retrospective clinical investigation. Surg Cosmet Dermatol. 2025;17:e20250432.
INTRODUCTION: Vitiligo is an autoimmune pigmentary disorder characterized by depigmented macules on the skin. It is associated with a range of autoimmune diseases. Antinuclear antibodies (ANA) are implicated in vitiligo, but their association with disease severity remains unclear.
OBJECTIVE: This study aims to assess antinuclear antibody (ANA) serum levels and evaluate their relationship with the severity and types of vitiligo.
METHODS AND PATIENTS: This is a retrospective study using preexisting patient records from the Pigmentary Disorders Unit of the Cairo Hospital of Dermatology and Venereology. The analysis included patients with complete medical records, including demographic data, clinical evaluation (VIDA and VASI scores), and laboratory results for ANA titer. Their correlation with disease severity and patient demographics was analyzed.
RESULTS: The study found that 462 patients (33%) were positive for ANA, with a higher prevalence in females (350 patients; 75.8%). A significant correlation was observed between ANA positivity and family history of vitiligo and systemic autoimmune diseases such as type 1 diabetes mellitus and thyroid disease. Weak positive correlations were found between ANA, different types of vitiligo, and disease severity scores.
CONCLUSION: Vitiligo is strongly associated with systemic autoimmune conditions. Routine monitoring of autoimmune markers in patients with vitiligo is recommended.
Keywords: Vitiligo; Antibodies, Antinuclear; Autoimmune Diseases.
Vitiligo is a pigmentary disorder of autoimmune etiology characterized by depigmented macules or patches on the skin. Its worldwide prevalence is estimated at around 0.5%–2%.1 Though not a life- or organ-threatening condition, it has a significant impact on the psychological well-being and quality of life of patients.
Clinically, it can be classified into three main types: segmental, non-segmental, and mixed (segmental and non-segmental).2 The Vitiligo Area Scoring Index (VASI) and the Vitiligo Disease Activity Score (VIDA) are two key tools used to assess vitiligo in clinical practice. VASI calculates a score based on the percentage of affected skin in order to evaluate the extent and degree of depigmentation, making it useful for tracking treatment response over time.3 VIDA, on the other hand, measures disease activity based on patient-reported progression over the previous six months, offering insight into how active it is.4 Together, they provide a comprehensive view of both disease severity and progression.
Vitiligo is thought to have a complex pathogenesis and to be a multifactorial polygenic disorder. The exact cause of the loss of epidermal melanocytes in vitiligo is still unknown, despite a number of proposed theories, including autoimmune, autocytotoxic, biochemical, neural, and genetic mechanisms.5 Currently, the most likely explanation is the autoimmune theory.6 Autoantibodies known as antinuclear antibodies (ANA) target various cellular components.
Many different types of connective tissue diseases typically have positive ANA levels, and laboratory tests are often used to screen for systemic lupus erythematosus (SLE) and other connective tissue diseases due to their extremely high sensitivity but low specificity.7 There is debate over whether to check ANA levels in patients with vitiligo. According to a recent meta-analysis, the prevalence of ANA is higher among patients with vitiligo compared to the general population.8 As an autoimmune condition involving T lymphocytes, ANA positivity may be highly prevalent among patients with vitiligo. The objective of this study was to assess antinuclear antibody levels and their relationship with the severity of different types of vitiligo.
This was a retrospective clinical investigation using preexisting patient records from the Pigmentary Disorders Unit of the Cairo Hospital of Dermatology and Venereology (Al-Haud Al-Marsoud). It included patients with a confirmed diagnosis of vitiligo based on clinical and Wood's lamp examination and who had complete medical records, including demographic data, clinical evaluation (VIDA and VASI scores), and laboratory results for ANA titer. The study was conducted from September 2023 to October 2024. Patients with vitiligo were included regardless of sex and age. Records of pregnant or lactating women, as well as patients with a history of malignancies, were excluded.
Patient data were extracted from the medical records of the Pigmentary Disorders Unit at the Cairo Hospital of Dermatology and Venereology, including:
1. Demographic data (age, sex, and family history of vitiligo).
2. Clinical history (onset, course, duration of the lesion, history of medications, systemic diseases such as diabetes mellitus, systemic lupus erythematosus, and thyroid disease) and associated dermatological disorders (eg, alopecia areata and psoriasis).
3. Vitiligo Disease Activity Score (VIDA);
This includes a six-point scale to measure vitiligo activity (scoring from +4 to -1) as shown in the figure.4
3.1 Active disease: VIDA score +4 to +1
3.2 Stable disease: VIDA score 0 to -1
4. Vitiligo Area Scoring Index (VASI).21
The formula comprises involvement of all body areas (probable range, 0–100) as follows: VASI = ∑ All body sites (hand units) × (remaining depigmentation). One hand unit, consisting of the palm plus the volar surface of all fingers, represents approximately 1% of the total body surface area. The degree of remaining depigmentation is recorded as the closest percentage: 0%, 10%, 25%, 50%, 75%, 90%, or 100%. At 100% depigmentation, no pigment remains; at 90%, there are specks of pigment; at 75%, the depigmented area exceeds the pigmented area; at 50%, the depigmented and pigmented areas are identical; at 25%, the pigmented area exceeds the depigmented area; at 10%, there are only specks of depigmentation.
5. Laboratory test results:
Antinuclear antibodies (ANA) were detected by immunofluorescence staining on Hep-2 sections. ANA were classified as positive when detectable at 1:80, 1:160, and 1:320 dilution or higher.
According to the inclusion and exclusion criteria, 2390 patients were eligible for this study but only 1400 had complete medical records, including demographic data, clinical evaluation, VIDA and VASI scores, and laboratory results for ANA titer.
All statistical analyses were performed using SPSS, version 28 (SPSS Inc., Chicago, IL). The data are presented as n and %. P-values of ≤0.05 and ≤0.01 were considered the cutoff point for statistically significant differences between variables. Categorical variables are presented as frequency and percentage, while continuous variables are presented as mean (SD). Categorical variables were compared using the chi-square (χ2) test, and Pearson's correlation coefficient when necessary. Statistical significance was set as p < 0.05. Two-way ANOVA was used to assess differences in mean changes in quantitative variables.
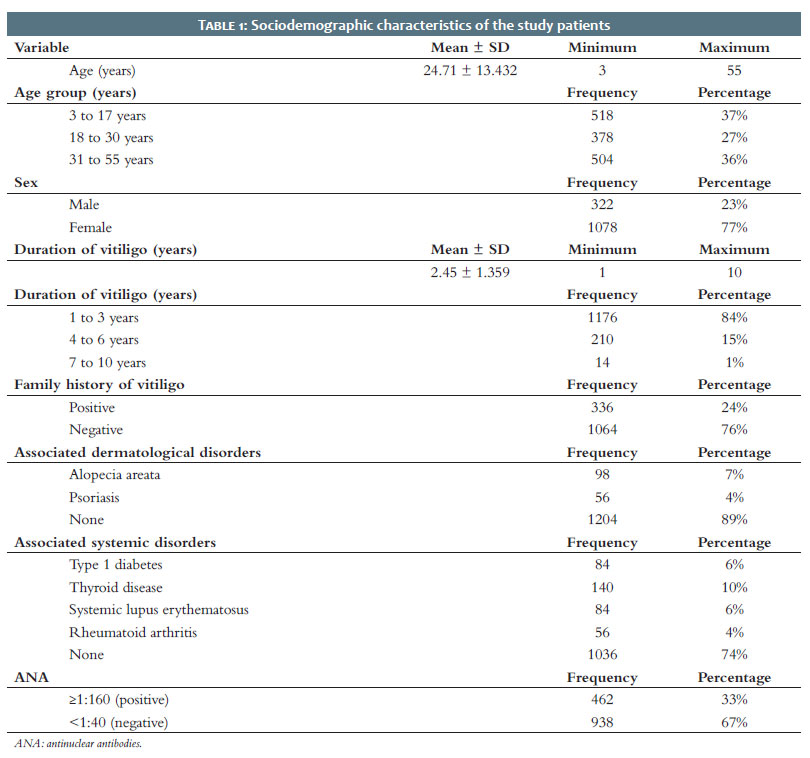
This study included 1400 patients diagnosed with vitiligo. The mean age of patients was 24.71 (13.432) years, ranging from 3 to 55 years. By age group, 37% of patients were 3–17 years old, 27% were 18–30 years old, and 36% were 31–55 years old. Most participants were female (77%), with males comprising 23% of the total. Mean disease duration was 2.45 (1.359) years, ranging from 1 to 10 years. Disease duration was distributed as follows: 84% of patients had vitiligo for 1 to 3 years, 15% for 4 to 6 years, and only 1% for 7 to 10 years. Positive family history was reported by 24% of patients, whereas 76% had no family history. In terms of associated dermatological disorders, 7% of patients reported having alopecia areata (AA) and 4% had psoriasis. However, 89% of patients had no associated dermatological disorders. In addition, 6% had type 1 diabetes mellitus (DM), 10% had thyroid disease (TD), 6% had SLE, and 4% had rheumatoid arthritis (RA), while 74% had no associated systemic disorders. Finally, 33% were positive for ANA and 67% were negative (Table 1).
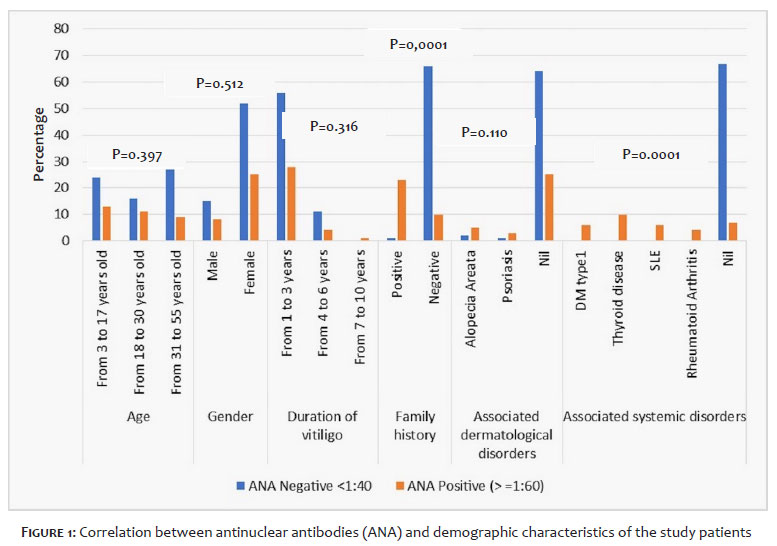
A weak positive correlation was found between ANA and age group, sex, and disease duration (χ2 = 1.85, p = 0.397- χ2 = 0.043, p = 0.512, and χ2 = 2.307, p = 0.316, respectively). A highly significant positive correlation was found between family history of vitiligo and ANA positivity (χ2 = 56.388, p < 0.0001). Among patients with a family history of vitiligo, 69.7% were positive for ANA, compared to 30.3% of patients with no family history of the disease. A weak positive correlation was found between ANA and associated dermatological disorders (χ2 = 1.580, p = 0.110). A highly significant positive correlation was found between ANA and associated systemic disorders (χ2 = 50.758, p < 0.0001) due to all patients (100%) with type 1 DM. TD was the most frequent among patients positive for ANA (30.3%), followed by type 1 DM and SLE (18.2%), and RA (12.1%) (Figure 1).
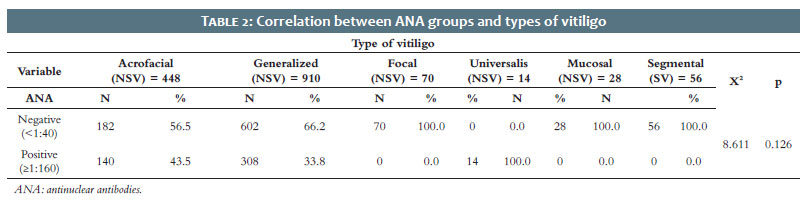
A weak positive correlation was observed between ANA values and different types of vitiligo. Negative ANA <1:40 was more frequent across all types of vitiligo except universalis (Table 2).
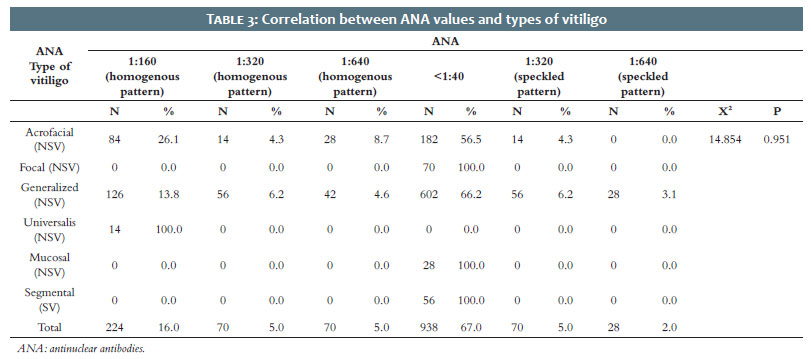
A weak positive correlation was found between ANA values and types of vitiligo (χ2 = 14.573, p = 0.951). The acrofacial (NSV) and generalized (NSV) forms were the most frequent types of vitiligo in relation to ANA levels (Table 3).
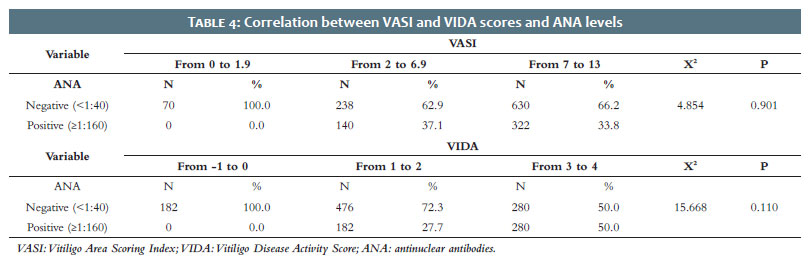
A weak positive correlation was observed between VASI scores, VIDA scores, and ANA values (Table 4).
Vitiligo is a dermatological disorder characterized by melanocytic abnormalities that result in depigmentation of the skin, mucous membranes, and hair. Although vitiligo can develop at any age and in any ethnic group, it usually manifests before the age of thirty. The onset of vitiligo has been linked to a number of etiological factors, including the immune, neurological, and endocrine mechanisms, environmental exposures, and genetics. Although vitiligo and autoimmune diseases can coexist, these associations do not always result in depigmentation.9
The present study included 1400 patients with vitiligo ranging in age from 3 to 55 years (mean, 24.7 years), consistent with other reports. In one study of 246 vitiligo cases, the average age was 25.9 years, while another reported a mean age of 34.5 years for 69 patients with vitiligo. Moreover, in a study of 74 patients with vitiligo, age ranged from 5 to 68 years (mean, 31.5 years), similar to the findings of the present study.10
In this study, 322 patients were male (23%), while 1078 (77%) were female. Morales-Sánchez et al. (2017) report that among 150 patients with vitiligo recruited for their study, 103 (68.7%) were women and 47 (31.3%) were men.11 In contrast, Dégboé et al. (2017) had more males (131; 53.3%) affected than females (115; 46.7%).12 The number of female patients with vitiligo may be higher because women notice changes in appearance and approach doctors sooner than men; in addition, because of social stigma, younger women tend to report the condition earlier due to matrimonial concerns.13
Duration of vitiligo in this study ranged from 1 to 10 years, most commonly 1 to 3 years (84%). Taneja et al. (2021) report durations of 2 to 4 years, very similar to the results of the present study; the small difference may be due to the larger number of patients (200 cases).14
A positive family history of vitiligo was present in 24% of cases in the present study, while 76% of cases had no family history. Alenizi et al. (2014) report that 18% of patients had a positive family history of vitiligo; with the small difference possibly explained by the difference in sample size (the present study included 1400 patients, Alenizi et al. had 74).15
In terms of dermatological disorders associated with vitiligo, AA was found in 7% of patients and psoriasis in 4%, while 83% had none. Barbulescu et al. (2020) report that vitiligo and AA are common autoimmune conditions characterized by white spots on the skin and bald spots on the scalp.16 A retrospective study of 1098 patients with vitiligo found AA to be the most common autoimmune disease associated with vitiligo.17
Associated systemic disorders found in the present study included type 1 DM (6%), TD (10%), SLE (6%), and RA (4%). The large-scale cross-sectional study by Choi et al. (2017) found that 86,210 patients with vitiligo were at an increased risk of SLE.18 In a descriptive cross-sectional study, 7.79% of 154 patients with vitiligo also had psoriasis.19 In line with the results of the present study, Percivalle et al. (2009) report that among 712 patients with vitiligo, only 3% had associated psoriasis.20 In a 10-year retrospective study involving 3280 patients, Sheth et al. (2013) showed that comorbid autoimmune conditions occur in approximately 23% of patients with vitiligo, including TD, RA, inflammatory bowel disease (IBD), SLE, and type 1 DM.21
Several studies have suggested vitiligo is associated with various other autoimmune diseases, including thyroid conditions, AA, type 1 DM, pernicious anemia, and RA. Among these, thyroid disorders were frequent among patients with vitiligo.21,22
The prevalence of positivity for antinuclear antibodies (ANA) in the present study was 33%. The findings are consistent with those reported by Chaiyabutr et al. (2020) in their study of 85 Thai patients with vitiligo, where ANA prevalence was 35.3%. That study concluded that the positive speckled ANA pattern was the most common, while the homogenous pattern ANA was the most common in the present study.23 ANA positivity was higher in females (75.8%) than males (24.2%); in line with those reported by Chaiyabutr et al. (2020), who concluded that female gender was a factor associated with ANA positivity (90%).23
There was no statistically significant correlation between age group and ANA positivity; patients aged 3 to 17 years had the highest positivity for ANA (39.4%), followed by those aged 18 to 30 years (33.3%). These findings are in line with the report by Chaiyabutr et al. (2020), who concluded that "ANA-positive was not associated with age but associated with the female gender."23
Kroon et al. (2013) found no correlation between presence of antibodies and recent disease activity or other clinical characteristics such as age, sex, extension, and duration of vitiligo; likewise, the present study found no significant correlation between ANA positivity and disease duration.24 There was a significant correlation between ANA positivity and family history of vitiligo; the same finding was reported by Lin X et al. (2011).25 A positive correlation was found between ANA positivity and associated dermatological disorders such as AA and psoriasis, in line with the findings reported by Garg et al. (2015).26 There was a significant correlation between ANA positivity and associated systemic disorders for all patients with type 1 DM, TD, SLE, and RA, in line with the findings of Chivu et al. (2022).9 Kanani et al. (2023) concluded that there is a significant association between vitiligo and other autoimmune diseases.
The identification and characterization of antinuclear autoantibodies in patients with vitiligo are vital indicators that support the findings of previous research indicating vitiligo is an autoimmune disease and may help pave the way for determining the potential incidence of other autoimmune conditions.27 The present study found a weak positive correlation between ANA positivity and VASI scores, with 37.1% and 33.8% ANA-positive for VASI scores from 2 to 7 and for more than 7 to 13, respectively; similar to the findings of Chivu et al. (2022).9 There was a weak positive correlation between ANA positivity and different types of vitiligo, with 35% for the acrofacial (NSV) form and 33.8% for the generalized (NSV) form. This is in line with the findings of Ekhlas et al. (2023),27 but higher than the findings of Kasumagic-Halilovic et al. (2013),28 who detected ANA in 17% of patients with vitiligo; the difference may be due to the larger sample size in the present study.
The present study reported a significant prevalence of antinuclear antibodies in patients with vitiligo. Therefore, to enable early detection and timely interventions, screening for autoimmune diseases among patients with vitiligo is recommended. Vitiligo should be considered a systemic rather than a skin disease.
1. Dermatologists should routinely screen for anti-thyroid and antinuclear antibodies in patients with vitiligo, especially those with a family history of autoimmune disease.
2. For better outcomes, encourage a multidisciplinary approach, involving dermatologists, endocrinologists, and rheumatologists, to optimize care for patients with vitiligo with autoimmune markers.
3. Educate patients about the potential link between autoimmune markers and vitiligo, stressing the importance of regular monitoring and management of autoimmune conditions.
Rasha Aoun
ORCID: 0009-0008-3863-4275
Approval of the final version of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study.
Dalia Hossam
ORCID: 0000-0001-9806-1714
Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
Ahmed Sadek
ORCID: 0000-0002-1603-2790
Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
Shaimaa Farouk
ORCID: 0000-0003-2415-2511
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Joge RR, Kathane PU, Joshi SH. Vitiligo: a narrative review. Cureus. 2022;14(9):e29307.
2. Zhang Y, Cai Y, Shi M, Jiang S, Cui S, Wu Y, et al. The prevalence of vitiligo: a meta-analysis. PloS one. 2016;11(9):e0163806.
3. Al Hammadi A, Castro CCS, Parmar NV, Ubogui J, Hatatah N, Ahmed HM, Llamado L. Prevalence and burden of vitiligo in Africa, the Middle East and Latin America. Skin Health and Disease. 2024;4(1):e317.
4. Al-Shammari SA, Alotaibi HM, Assiri MA, Altokhais MI, Alotaibi MS, Alkhowailed MS. Quality of life in vitiligo patients in central Saudi Arabia. Saudi Med J. 2021;42(6):682-7.
5. Ezzedine K, Lim HW, Suzuki TA, Katayama I, Hamzavi I, Lan CC, et al. Revised classification/nomenclature of vitiligo and related issues: the Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25(3):E1-13.
6. Kemp EH, Waterman EA, Weetman AP. Autoimmune aspects of vitiligo. Autoimmunity. 2001;34(1):65-77.
7. Dwivedi M, Kemp EH, Laddha NC, Mansuri MS, Weetman AP, Begum R. Regulatory T cells in vitiligo: implications for pathogenesis and therapeutics. Autoimmunity Rev. 2015;14(1):49-56.
8. Alkhateeb A, Fain PR, Thody A, Bennett DC, Spritz RA. Epidemiology of vitiligo and associated autoimmune diseases in caucasian probands and their families. Pigment Cell Res. 2003;16(3):208-14.
9. Chivu AM, Bălășescu E, Pandia LD, Nedelcu RI, Brînzea A, Turcu G, et al. Vitiligo—thyroid disease association: when, in whom, and why should it be suspected? a systematic review. J Personal Med. 2022;12(12):2048.
10. Rashed L, Hay RA, Mahmoud R, Hasan N, Zahra A, Fayez S. Association of angiotensin-converting enzyme (ace) gene polymorphism with inflammation and cellular cytotoxicity in vitiligo patients. PloS one. 2015;10(7):e0132915.
11. Morales-Sánchez MA, Vargas-Salinas M, Peralta-Pedrero ML, Olguín-García MG, Jurado-Santa Cruz F. Impact of vitiligo on quality of life. Actas Dermosifiliogr. 2017;108(7):637-42.
12. Dégboé B, Atadokpèdé F, Saka B, Adégbidi H, Koudoukpo C, Yédomon H, do Ango‐ Padonou F. Vitiligo on black skin: epidemiological and clinical aspects in dermatology, Cotonou (Benin). Int J Dermatol. 2017;56(1):92-6.
13. Vora RV, Patel BB, Chaudhary AH, Mehta MJ, Pilani AP. A clinical study of vitiligo in a rural set up of Gujarat. Indian J Community Med. 2014;39(3):143-6.
14. Taneja N, Sreenivas V, Sahni K, Gupta V, Ramam M. Disease stability in segmental and non-segmental vitiligo. Indian Dermatol Online J. 2022;13(1):60-3.
15. Alenizi DA. Consanguinity pattern and heritability of vitiligo in Arar, Saudi Arabia. J Family Community Med. 2014;21(1):13-6.
16. Barbulescu CC, Goldstein NB, Roop DR, Norris DA, Birlea SA. Harnessing the power of regenerative therapy for vitiligo and alopecia areata. J Invest Dermatol. 2020;140(1):29-37.
17. Gill L, Zarbo A, Isedeh P, Jacobsen G, Lim HW, Hamzavi I. Comorbid autoimmune diseases in patients with vitiligo: a cross-sectional study. J Am Acad Dermatol. 2016;74(2):295-302.
18. Choi CW, Eun SH, Choi KH, Bae JM. Increased risk of comorbid rheumatic disorders in vitiligo patients: a nationwide population‐based study. J Dermatol. 2017;44(8):909-13.
19. Yazdanpanah MJ, Banihashemi M, Pezeshkpoor F, Moradifar M, Feli S, Esmaeili H. Evaluation between association of psoriasis and vitiligo. J Cutan Med Surg. 2015;19(2):140-3.
20. Percivalle S, Piccinno R, Caccialanza M. Concurrence of vitiligo and psoriasis: a simple coincidence? Clin Exp Dermatol. 2009;34(1):90-1.
21. Sheth VM, Guo Y, Qureshi AA. Comorbidities associated with vitiligo: a ten-year retrospective study. Dermatology. 2014;227(4):311-5.
22. McLeod DS, Cooper DS. The incidence and prevalence of thyroid autoimmunity. Endocrine. 2012;42(2):252-65.
23. Chaiyabutr C, Wongpraparut C, Charoenpipatsin N, Pruksaeakanan C, Silpa‐archa N. The necessity of antinuclear antibody investigation in pre‐phototherapy vitiligo patients: a retrospective study. Photodermatol Photoimmunol Photomed. 2020;36(5):373-7.
24. Kroon MW, Kemp EH, Wind BS, Krebbers G, Bos JD, Gawkrodger DJ, et al. Melanocyte antigen‐specific antibodies cannot be used as markers for recent disease activity in patients with vitiligo. J Eur Acad Dermatol Venereol. 2013;27(9):1172-5.
25. Lin X, Tian H, Xianmin M. Possible roles of B lymphocyte activating factor of the tumour necrosis factor family in vitiligo autoimmunity. Med Hypotheses. 2011;76(3):339-42.
26. Garg S, Mahajan VK, Mehta KS, Chauhan PS, Gupta M, Yadav RS, et al. Vitiligo and associated disorders including autoimmune diseases: a prospective study of 200 Indian patients. Pigment Internatinal. 2015;2(2):91-6.
27. Kanani E, Issa A, Al-Ahmadi K. Evaluation of autoimmune biomarkers in vitiligo patients' serum. J Population Ther Clin Pharmacol. 2023;30(2):283-90.
28. Kasumagic-Halilovic E, Ovcina-Kurtovic N, Jukic T, Karamehic J, Begovic B, Samardzic S. Vitiligo and autoimmunity. Med Arch. 2013;67(2):91.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}