


Lina María Osorio Cock1; Jaime Alberto Rengifo Palacios1; María Paulina Uribe Posada1; María Alejandra Sarabia de Capozzi2; María Aida Angulo Morillo3
Funding: None.
Conflict of interest: None.
Submitted on: 03/27/2025.
Final decision: 07/02/2025.
How to cite this article: Osorio Cock LM, Rengifo Palacios JA, Uribe Posada MP, Sarabia de Capozzi MA, Angulo Morillo MA. Advances in evaluation and management of hyaluronic acid-induced foreign body granulomas: a systematic review. Surg Cosmet Dermatol. 2025;17;e20250457.
We conducted a systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) of cases of foreign body granuloma (FBG) induced by hyaluronic acid (HA). A total of 27 patients with HA filler-induced FBG reported in literature were included. The estimated incidence of HA-induced FBG is 0.02%-0.6%. Several factors are involved, including cross-linking agents and impurities. The most frequent clinical presentation is asymptomatic nodules, although other lesions may occur. Histopathological examination is the gold standard for diagnosis, but ultrasound is a promising tool. Treatment options include expectant management, hyaluronidase, corticosteroids, 5-fluorouracil, and surgery.
Keywords: Hyaluronic Acid; Dermal Fillers; Granuloma, Foreign-Body.
Hyaluronic acid (HA) injection is the second most common aesthetic nonsurgical procedure, with a 28.9% increase over the past 5 years.1 Although minimally invasive, it can lead to complications. Classically, complications are divided into 3 groups based on the time of onset: early (within 14 days), late (14 days to 1 year), and delayed (over 1 year).2 Among the late and delayed complications, foreign body granulomas (FBGs) are noteworthy. FBG is a histological inflammatory reaction to an antigen, characterized by the aggregation of macrophages and foreign body giant cells.3
Under normal circumstances, HA integrates into tissues without inflammatory infiltrates or epidermal or dermal alterations.4 With few reports and studies available, HA-induced FBG appears to be rare, with an estimated frequency of 0.02%-0.4% in retrospective reviews.5 However, biopsies required for histological confirmation are rarely performed because of concerns regarding the cosmetic outcomes of aesthetic procedure complications. Underdiagnosis is therefore suspected, and whether histological findings correlate with current clinical and imaging diagnoses remains uncertain.
As a result, few studies are available, and empirical treatment remains the norm, with variable outcomes. We aim to review case reports and case series in the literature to improve understanding, explore alternative diagnostic methods, and propose more accurate and effective treatment approaches.
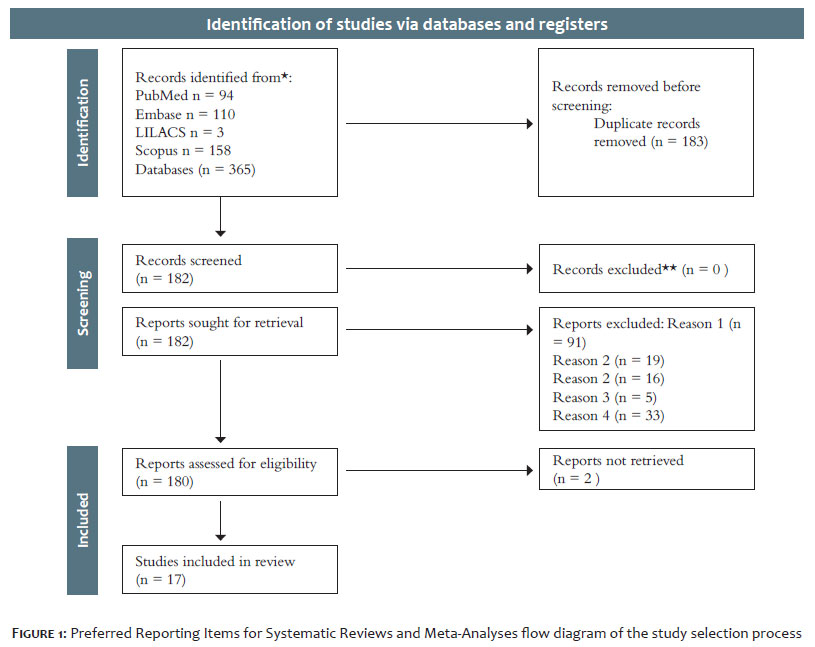
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement in January 2025. A natural language search was performed to identify potentially relevant articles. The search terms used were "hyaluronic acid" and "granuloma," combined with the Boolean operator "AND." The Title/Abstract field tag was applied in PubMed, Embase, Scopus, and LILACS.
Inclusion criteria were primary studies, case reports, or case series describing HA filler-induced FBG. Exclusion criteria were failure to meet inclusion criteria (reason 1); absence of histopathological confirmation of FBG (reason 2); combination with other fillers (reason 2); genitourinary applications (reason 3); and animal studies (reason 4). No language or time restrictions were applied. After screening, 17 studies were included (Figure 1). Articles were manually reviewed, and data were extracted into Excel forms. The included studies are presented in the results.
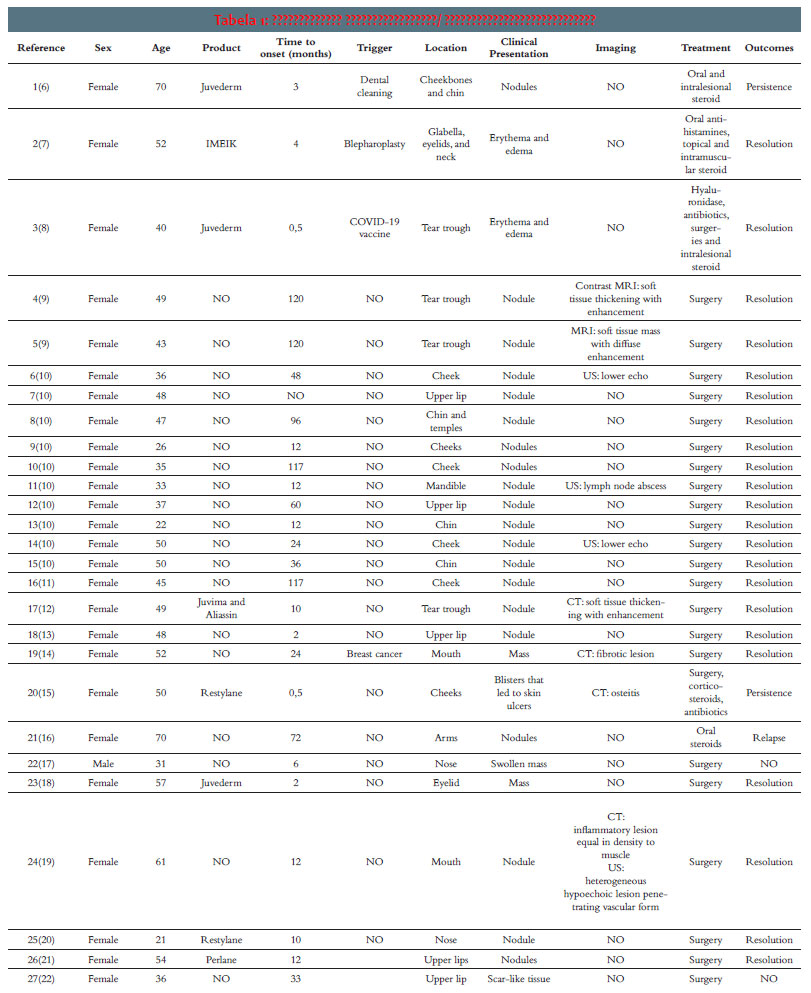
We identified 17 case reports or case series of HA-induced FBG, comprising 32 patients. All patients were female, with the exception of 1 male. A histology-focused study reported 5 cases of HA filler-induced FBG among other dermal fillers; however, because clinical data were presented only as means and modes that included other fillers, it was not included in the subsequent analysis. The cases are summarized in Table 1.
Table 1. Summary of reported cases. Magnetic resonance imaging (MRI), computed tomography (CT), and ultrasound (US). The mean age of patients was 44 years (range, 21–70), and the mean time to onset was 35 months (range, 0.5-120). Juvederm was the most frequently reported product; however, in most cases, the product used was unknown or not reported. A total of 4 cases described relevant background factors months before onset, including dental cleaning, blepharoplasty, COVID-19 vaccination, and breast cancer diagnosis and treatment. Nodules and masses, either inflammatory or noninflammatory, were the most common clinical presentations, but inflammatory plaques, papules, scar-like lesions, and blisters that progressed to ulcerative or fibrotic manifestations were also reported. The most frequently affected sites were perioral (n = 8), cheeks (n = 7), periocular (n = 5), and nose (n = 2), among others. Imaging modalities included MRI, CT, and US. Surgery was the most common treatment, generally with favorable outcomes, although corticosteroids, antibiotics, and hyaluronidase were also used.
Approximately 15 years ago, the frequency of HA-induced FBG was estimated at 0.02%-0.4% in retrospective reviews.5 A more recent meta-analysis of 1,496 participants who underwent HA lip augmentation reported a frequency of 0.6%.23 In contrast, a retrospective analysis of 492 patients who underwent nonsurgical rhinoplasty with HA found no cases of FBG.24
This variability is likely related to multiple factors, as discussed later in pathogenesis and etiology. However, discrepancies in terminology (ie, delayed-onset nodules [DONs], inflammatory nodules, noninflammatory nodules, granulomas) and diagnostic methodology also contribute, as further discussed.
When considering DONs, the Manufacturer and User Facility Device Experience (MAUDE) database of the US Food and Drug Administration (FDA) showed that 71.8% of delayed-onset reactions were nodules (42.1% inflammatory and 29.7% noninflammatory), whereas 6.7% were granulomas, without a distinct classification.25 Another retrospective study found an overall incidence of DONs of 0.33% in 2,139 patients who underwent HA injections. Of these, 7 patients presented with DONs, but only 1 biopsy was performed, confirming FBG.6
These findings suggest that HA-induced FBG may be underdiagnosed, since biopsies are rarely performed owing to concerns about unfavorable cosmetic outcomes after aesthetic procedures.26
Although HA is generally thought to integrate into tissues without inflammation,4 some studies suggest the presence of a mild inflammatory reaction that goes unnoticed, characterized by a discrete population of macrophages with vacuolated cytoplasm and rare small giant cells, reflecting normal resorption.27 In contrast, FBGs, characterized by the aggregation of macrophages and foreign body giant cells, are formed through 4 phases3:
Recognition and inflammation: Implantation of the foreign material is followed by an innate immune response involving polymorphonuclear leukocytes — mainly neutrophils — along with complement activation and cytokine release.
Macrophage adhesion: The progression of inflammation directs monocytes, through cytokine signaling, to migrate into tissues and differentiate into macrophages.
Macrophage fusion: Aggregation and fusion of macrophages, mediated by interleukin-4 and interleukin-13, likely occur in response to particle size, leading to the formation of foreign body giant cells.
Crosstalk between macrophages and foreign body giant cells: Both cell types secrete cytokines that recruit and activate fibroblasts, leading to the formation of a fibrous capsule around the foreign material.
HA-induced FBGs are considered an abnormal or exaggerated reaction to exogenous stimuli, often described as allergy or hypersensitivity. Although the central role of macrophages is well established, a type IVa hypersensitivity reaction has been inferred.28 However, this reaction is a T cell-mediated response, and the extent to which the adaptive immune system participates remains controversial. T cells have been identified in case reports of HA-induced FBG and are hypothesized to perpetuate ongoing macrophage activation around the granuloma.9,12,15,20,22,29 In contrast, a series of 18 biopsies from patients with late-onset inflammatory adverse events to different fillers, including HA, showed no CD3-positive immune cells corresponding to T cell populations.30
Moreover, some authors have reported no adverse effects after HA re-exposure, leading to the hypothesis that HA-induced FBG may not represent a type IVa hypersensitivity reaction.5,6 Nonetheless, diagnostic tests for type IV hypersensitivity reactions have limited sensitivity and specificity.31 Patch testing is considered the gold standard for diagnosing type IV hypersensitivity,32 yet its sensitivity and specificity for delayed hypersensitivity drug eruptions are 32% and 92%, respectively,33 indicating a high rate of false-negative results. Another factor less frequently considered is the potential role of HA as an adjuvant in immune responses.34
HA is a glycosaminoglycan naturally present in the human body and, therefore, should not normally be recognized as foreign by the immune system. Nonetheless, HA functions as an extracellular matrix component and serves as an adhesive substrate for cellular migration, which may enhance immune responses.34 Several mechanisms have been proposed as potential antigenic triggers of HA-induced FBG10,35,36:
Cross-linker: Agents such as 1,4-butanediol diglycidyl ether (BDDE), methacrylamide, hydrazide, carbodiimide, divinyl sulfone, and poly(ethylene glycol) diglycidyl ether are used to delay HA degradation by endogenous hyaluronidases. This effect is achieved through covalent bonding between HA molecules, reducing enzymatic exposure. BDDE is currently the most commonly used cross-linker due to its stability, biodegradability, and long safety record. Residual unreacted BDDE at levels < 2 ppm is considered safe; however, byproducts are not always adequately evaluated.37
Impurities: During production, HA may come into contact with unintended molecules. Traces of stainless steel, aluminum, silicone, sodium hydroxide, and streptococcal endotoxins have been identified. Threshold limits for particulate matter in prefilled syringes are 6,000 and 600 per container for particles ≥ 10 µm and ≥ 25 µm, respectively.35,38
Infection: Delayed-onset reactions, including FBG, have been reported after infections, likely due to inoculation into previously implanted dermal fillers and subsequent inflammatory responses.39 Several authors have associated granuloma formation with biofilm development.13 Biofilms on HA surfaces may enable persistent infection with minimal host immune response.10
Immune system: FBG has frequently been reported following immune challenges such as vaccination, infections, and dental procedures. Cases of delayed hypersensitivity to HA after influenza-like illness have been described.31 In a study of 2,139 patients treated with HA, 7 developed DONs, 6 of whom had undergone dental procedures 1-168 days before nodule formation. A seasonal pattern was also noted, with most cases (71%) occurring between September and December.6 Another study of 3,255 patients receiving 8,067 filler syringes reported higher granuloma rates in the post-COVID-19 period (0.3% vs 0.0%, P = .009).40 Both COVID-19 infection and vaccination have been implicated, as reexposure appears to trigger faster responses.41,42 The SARS-CoV-2 spike protein, which binds angiotensin-converting enzyme 2 (ACE2) receptors, favors a proinflammatory local Th1 cascade, promoting CD8+ T cell–mediated reactions to incipient granulomas.43 A heightened immune state may enable recognition of previously undetected antigens, thereby triggering granulomatous inflammation.35
HA molecular weight: Low-molecular weight HA (< 1,000 kDa) has been shown to be proinflammatory, whereas high-molecular weight HA is generally considered anti-inflammatory.44 Vycross technology has been associated with higher rates of DONs,6,25 although this remains controversial, as HA degradation would inherently release low-molecular weight fragments.35
Injection volume and technique: In a study of 4,500 patients, those who developed DONs had received a higher cumulative injection volume (5.0 mL) compared with those without nodules (0.5-1.5 mL lower cumulative volume), suggesting volume as a risk factor.45 Other studies, however, did not replicate this finding.6 Expert consensus nonetheless suggests that larger bolus volumes may increase the risk of FBG and other complications.46 Repeated injections using the droplet technique and incorrect injection depth have also been implicated,36 consistent with the heightened immune surveillance in dermal tissues compared with subcutaneous fat and deeper planes.
Reports have documented HA-induced FBGs as early as a few weeks after injection and as late as 10 years post-procedure. This variability challenges the clinical value of categorizing HA-induced complications into early, late, or delayed presentations.2 Patient history is often unremarkable, and clinicians may be unaware of prior cosmetic procedures.47
HA-induced FBG appears more common in periorificial areas, similar to DONs. The most frequently affected sites are the lips (41.1%), followed by the nasolabial folds (23.6%), marionette lines (22.1%), perioral region (19.3%), and tear troughs (12.1%).25 Similar patterns have been observed with other dermal fillers.48 These regions may be more susceptible to complications due to repetitive movement and fixed points of origin and insertion, which facilitate filler deposition and increase the risk of FBG formation.
In a review of 11 cases of orofacial FBG following HA injection, the most common presentation was noninflammatory nodules,10 consistent with findings in the present report. However, atypical manifestations have also been described, including maculopapular lesions,7 papules, plaques,49 scar-like lesions,22 and blisters progressing to ulcerative-fibrotic changes,15 sometimes associated with inflammatory signs such as erythema and/or edema.50 Consequently, categorizing FBG solely under broader clinical groups such as "DONs," "inflammatory nodules," or "noninflammatory nodules"26 is imprecise and not diagnostic.
In a retrospective review of 6 patients who underwent biopsy for facial nodules persisting > 3 months after HA injection, 4 cases were classified as "nongranulomatous" nodules containing only HA, while 2 were identified as granulomatous nodules.51 Normal resorption is characterized by discrete populations of macrophages with vacuolated cytoplasm and occasional small giant cells.27
In a histopathologic review of 15 cases, foreign body granulomatous reactions to HA filler were predominantly characterized by vacuoles of basophilic material surrounded by palisading histiocytes, with variable numbers of eosinophils and foreign body giant cells.52 Multiple stains can be used to identify HA deposits. Hematoxylin-eosin reveals HA as gray to pale blue, while Alcian blue and colloidal iron stains demonstrate HA as bright blue to green-blue. Although the latter provide improved visualization, they are not mandatory.53 Morphologically, biphasic HA fillers typically appear granular, filamentous, or wispy, whereas monophasic HA is usually amorphous.10
Imaging studies can support the diagnostic work-up of HA-induced FBG. US findings typically include hypoechoic lesions with internal particulate echoes, peripheral hypoechogenicity, increased vascularity within and around the deposits, and increased echogenicity and thickness of the subcutaneous tissue.54–56 Conversely, some deposits are described as anechoic areas with sharp, regular borders.57 Magnetic resonance imaging and computed tomography have also been used to evaluate nonvascular complications of HA, one of which is FBG.56 Nevertheless, FBG remains primarily a histological diagnosis, and no studies have established diagnostic accuracy. Despite this, imaging techniques are promising as complementary evaluation tools.
Current guidelines are limited by reliance on clinical diagnosis, typically distinguishing between inflammatory and noninflammatory nodules. Granulomas are often grouped with the latter,58 even though, as noted, they may present with diverse clinical features distinct from noninflammatory nodules. The absence of a definitive diagnosis has led to a "scatter-gun" polypharmacy approach, which carries risks of adverse effects and suboptimal outcomes.26 The reluctance to perform biopsies in aesthetic complications, due to concerns about scarring, further limits histological confirmation. In this context, US emerges as a noninvasive tool that can aid more accurate evaluation.
Watchful waiting may be appropriate for noninflammatory nodules,46 as some granulomas resolve spontaneously within 2 years.59 Several therapeutic approaches have been described, including hyaluronidase, oral or intralesional corticosteroids, antihistamines, anti-inflammatories, antibiotics, intralesional 5-fluorouracil, and surgery.36 Consistent with prior reviews, most HA-induced FBG have been successfully managed with surgical excision.60 However, this may reflect a bias toward excision in cases selected for histological analysis, which suggests underdiagnosis in nonoperated patients.
From a treatment rationale perspective, since FBGs are composed of HA deposits, inflammatory infiltrates, fibrosis, and/or capsule formation, management with hyaluronidase, intralesional corticosteroids, and 5-fluorouracil is recommended, preferably under US guidance to ensure precise injection. Combining intralesional triamcinolone with 5-fluorouracil appears to reduce the risk of skin atrophy associated with higher triamcinolone doses.61 Oral corticosteroids may also be effective but are generally reserved due to systemic side effects.
The use of antibiotics should be limited to their anti-inflammatory properties, as alternative agents can achieve similar effects and concerns about global antibiotic resistance remain. Multiple sessions of hyaluronidase combined with triamcinolone and 5-fluorouracil may be required. US guidance not only improves injection accuracy but also helps determine whether hyaluronidase is indicated, given its activity against extracellular HA deposits but limited effect on inflammatory infiltrates, fibrosis, or capsule. Surgical excision should be considered the last resort.62
As noted, HA-induced FBG is primarily a histological diagnosis, with limited correlation to clinical presentation and uncertain correlation between histological findings and imaging studies, although imaging remains promising. The overlap among clinical, imaging, and histopathological terminology related to HA-induced FBG obscures diagnosis and consequently hampers research. Some studies cited in the discussion were not included in the results due to the absence of histopathological confirmation. Furthermore, the number of available studies is scarce, and underreporting is likely. Additional research is therefore required.
Although the exact prevalence of HA-induced FBG remains uncertain, it is undoubtedly a potential complication. The current time-based classification of complications may warrant reevaluation. To date, HA-induced FBG continues to be a histological diagnosis, underscoring the need for biopsies to ensure accurate diagnosis and appropriate treatment. US is a valuable evaluation tool and a promising diagnostic method, but further studies are needed to establish correlations between imaging and histological findings. Tailoring treatment to the presence of HA deposits, inflammatory infiltrates, fibrosis, and/or capsule formation may reduce adverse effects and optimize outcomes. More studies are also required to define effective therapeutic strategies.
Lina María Osorio Cock
ORCID: 0000-0002-5591-7954
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Jaime Alberto Rengifo Palacios
ORCID: 0009-0009-1797-4534
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
María Paulina Uribe Posada
ORCID: 0009-0002-1956-8491
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
María Alejandra Sarabia de Capozzi
ORCID: 0009-0003-0155-2544
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
María Aida Angulo Morillo
ORCID: 0009-0000-3928-3392
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Triana L, Palacios Huatuco RM, Campilgio G, Liscano E. Trends in surgical and nonsurgical aesthetic procedures: a 14-year analysis of the International Society of Aesthetic Plastic Surgery —ISAPS. Aesthetic Plast Surg. 2024;48(20):4217–27.
2. Zaccaria G, Dotti A, Benanti E, Vigliarolo C, Vaienti L. A treatment algorithm for hyaluronic acid filler related complications of the face. J Plast Reconstr Aesthet Surg. 2024;91:207–17.
3. Lee JM, Kim YJ. Foreign body granulomas after the use of dermal fillers: pathophysiology, clinical appearance, histologic features, and treatment. Arch Plast Surg. 2015;42(2):232–9.
4. Tran C, Carraux P, Micheels P, Kaya G, Salomon D. In vivo bio-integration of three hyaluronic acid fillers in human skin: a histological study. Dermatology. 2014;228(1):47–54.
5. Lemperle G, Gauthier-Hazan N, Wolters M, Eisemann-Klein M, Zimmermann U, Duffy DM. Foreign body granulomas after all injectable dermal fillers: part 1. possible causes. Plast Reconstr Surg. 2009;123(6):1842–63.
6. Rivers JK. Incidence and treatment of delayed-onset nodules after VYC filler injections to 2139 patients at a single canadian clinic. J Cosmet Dermatol. 2022;21(6):2379–86.
7. Lai D, Liu H, Kong L, Cheng S. Delayed complication of botulinum toxin and hyaluronic acid filler injections: a case report. J Cosmet Dermatol. 2022;21(6):2374–8.
8. Denkova R, Georgieva I, Kantardjiev V. Immune system triggers as a factor for the formation of foreign body granuloma after hyaluronic acid fillers treatment: a case report and treatment protocol. J Appl Cosmetol. 2024;42(2).
9. Arici C, Tosuner Z. Infraorbital mass long after dermal filler injection: a report of two cases. J Cosmet Dermatol. 2023;22(4):1245–8.
10. Delayed foreign body granulomas in the orofacial region after hyaluronic acid injection. Chin J Dent Res. 2020;23(4):289–96.
11. Zhang FF, Xu ZX, Chen Y. Delayed foreign body granulomas in the orofacial region after hyaluronic acid injection. Chin J Dent Res. 2020;23(4):289–96.
12. Parulan MAA, Sundar G, Lum JH, Ramachandran U. A case report on dermal filler-related periorbital granuloma formation. Orbit. 2019;38(2):169–72.
13. Tamiolakis P, Piperi E, Christopoulos P, Sklavounou-Andrikopoulou A. Oral foreign body granuloma to soft tissue fillers. Report of two cases and review of the literature. J Clin Exp Dent. 2018;10(2):e177–84.
14. Kaczorowski M, Nelke K, Luczak K, Halon A. Filler migration and florid granulomatous reaction to hyaluronic acid mimicking a buccal tumor. J Craniofac Surg. 2020;31(1):e78–9.
15. Cecchi R, Spota A, Frati P, Muciaccia B. Migrating granulomatous chronic reaction from hyaluronic acid skin filler (restylane): review and histopathological study with histochemical stainings. Dermatology. 2014;228(1):14–7.
16. Tonin B, Colato C, Bruni M, Girolomoni G. Late granuloma formation secondary to hyaluronic acid injection. Dermatol Online J. 2020;26(7):13030.
17. Leupe P, Menger DJ. The injectable filler in rhinoplasty: not a complication-free alternative. B-ENT. 2016;12(2):137–42.
18. Dryden SC, Gabbard RD, Meador AG, Stoner AE, Klippenstein KA, Wesley RE. A case of orbital granuloma secondary to dermal filler injection. Cureus. 2021;13(12):e20606.
19. Nishimura M, Sakamoto S, Hoshino M, Miyazaki Y, Yamamoto J, Sakashita H, et al. Histological features of delayed foreign body granuloma with epithelioid histiocyte aggregation and eosinophilic reaction due to hyaluronic acid injection. Case Rep Dent. 2024;2024:5565324.
20. Kim JH, Choi JS, Yun JH, Kang HK, Baek JO, Roh JY, et al. Foreign body reaction to injectable hyaluronic acid: late granuloma formation. Ann Dermatol. 2015;27(2):224–5.
21. Alcântara CEP, Noronha MS, Cunha JF, Flores IL, Mesquita RA. Granulomatous reaction to hyaluronic acid filler material in oral and perioral region: a case report and review of literature. J Cosmet Dermatol. 2018;17(4):578–83.
22. Hwang MJ, Lee YP, Jin YT, Chiang CP. Hyaluronic acid-induced foreign body granuloma in the upper lip. J Dent Sci. 2023;18(3):1429–30.
23. Czumbel LM, Farkasdi S, Gede N, Mikó A, Csupor D, Lukács A, et al. Hyaluronic acid is an effective dermal filler for lip augmentation: a meta-analysis. Front Surg. 2021;8:681028.
24. Jalali A. Nonsurgical rhinoplasty using the hyaluronic acid filler VYC-25L: safety and patient satisfaction in a retrospective analysis of 492 patients. J Cosmet Dermatol. 2024;23(2):426–33.
25. Cohen JL, Hicks J, Nogueira A, Lane V, Andriopoulos B. Postmarket safety surveillance of delayed complications for recent fda-approved hyaluronic acid dermal fillers. Dermatol Surg. 2022;48(2):220–4.
26. Convery C, Davies E, Murray G, Walker L. Delayed-onset nodules (dons) and considering their treatment following use of hyaluronic acid (ha) fillers. J Clin Aesthetic Dermatol. 2021;14(7):E59–67.
27. Plantier F. Lessons on reactions to aesthetic fillers. Ann Pathol. 2024;44(6):491– 7. [French]
28. Jutel M, Agache I, Zemelka-Wiacek M, Akdis M, Chivato T, Del Giacco S, et al. Nomenclature of allergic diseases and hypersensitivity reactions: adapted to modern needs: an eaaci position paper. Allergy. 2023;78(11):2851–74.
29. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, immune-mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241–58.
30. Decates TS, Velthuis PJ, Jhingoerie R, Gibbs S, Bachour Y, Niessen FB. No association found between late-onset inflammatory adverse events after soft tissue filler injections and the adaptive immune system. J Cosmet Dermatol. 2023;22(2):458–63.
31. Turkmani MG, De Boulle K, Philipp-Dormston WG. Delayed hypersensitivity reaction to hyaluronic acid dermal filler following influenza-like illness. Clin Cosmet Investig Dermatol. 2019;12:277–83.
32. Muthupalaniappen L, Jamil A. Prick, patch or blood test? A simple guide to allergy testing. Malays Fam Physician. 2021;16(2):19–26.
33. Hassoun-Kheir N, Bergman R, Weltfriend S. The use of patch tests in the diagnosis of delayed hypersensitivity drug eruptions. Int J Dermatol. 2016;55(11):1219–24.
34. Alijotas-Reig J, Hindié M, Kandhaya-Pillai R, Miro-Mur F. Bioengineered hyaluronic acid elicited a nonantigenic T cell activation: implications from cosmetic medicine and surgery to nanomedicine. J Biomed Mater Res A. 2010;95A(1):180–90.
35. Lee W, Shah-Desai S, Rho NK, Cho J. Etiology of delayed inflammatory reaction induced by hyaluronic acid filler. Arch Plast Surg. 2024;51(1):20–6.
36. Singh K, Nooreyezdan S. Nonvascular complications of injectable fillers—prevention and management. Indian J Plast Surg. 2020;53(3):335–43.
37. Fidalgo López J, Deglesne PA, Arroyo R, Sepúlveda L, Ranneva E, Deprez P. Detection of a new reaction by-product in BDDE cross-linked autoclaved hyaluronic acid hydrogels by LC–MS analysis. Med Devices Evid Res. 2018;11:367–76.
38. Lee W, Rho NK, Yang EJ. Determination of hyaluronic acid dermal filler impurities using SEM/EDS Analysis. Polymers. 2023;15(7):1649.
39. Ibrahim O, Overman J, Arndt KA, Dover JS. Filler nodules: inflammatory or infectious? A review of biofilms and their implications on clinical practice. Dermatol Surg. 2018;44(1):53–60.
40. Michel JC, Perenack JD, Chapple AG, Christensen BJ. Are delayed dermal filler granulomas more common since COVID-19? J Oral Maxillofac Surg. 2023;81(1):42–8.
41. Witt J, Hooper D, Munavalli GG. Delayed inflammatory reaction to hyaluronic acid filler following shingrix and fluzone vaccines treated with lisinopril. JAAD Case Rep. 2022;23:133–5.
42. Alijotas-Reig J, García-GImenez V, Velthuis PJ, Niessen FB, Decates TS. Inflammatory immune-mediated adverse reactions induced by COVID -19 vaccines in previously injected patients with soft tissue fillers: a case series of 20 patients. J Cosmet Dermatol. 2022;21(8):3181–7.
43. Munavalli GG, Guthridge R, Knutsen-Larson S, Brodsky A, Matthew E, Landau M. COVID-19/SARS-CoV-2 virus spike protein-related delayed inflammatory reaction to hyaluronic acid dermal fillers: a challenging clinical conundrum in diagnosis and treatment. Arch Dermatol Res. 2022;314(1):1–15.
44. Rayahin JE, Buhrman JS, Zhang Y, Koh TJ, Gemeinhart RA. High and low molecular weight hyaluronic acid differentially influence macrophage activation. ACS Biomater Sci Eng. 2015;1(7):481–93.
45. Humphrey S, Jones DH, Carruthers JD, Carruthers A, Beleznay K, Wesley N, et al. Retrospective review of delayed adverse events secondary to treatment with a smooth, cohesive 20-mg/mL hyaluronic acid filler in 4500 patients. J Am Acad Dermatol. 2020;83(1):86–95.
46. Philipp-Dormston WG, Goodman GJ, De Boulle K, Swift A, Delorenzi C, Jones D, et al. Global approaches to the prevention and management of delayed-onset adverse reactions with hyaluronic acid-based fillers. Plast Reconstr Surg - Glob Open. 2020;8(4):e2730.
47. Cuylits N. Complications of hyaluronic acid injections in aesthetic medicine: an emerging pathology? Rev Med Brux. 2024;45(4):414–8.
48. Machado RA, Oliveira LQ, Martelli-Júnior H, Pires FR, Carvas JB, Rogerio VE, et al. Adverse reactions to the injection of face and neck aesthetic filling materials: a systematic review. Med Oral Patol Oral Cirugia Bucal. 2023;28(3):e278–84.
49. Bowles A, Ghalili S, Ojong OB, Vasile GF, Li YM, Aguilera SB. Novel management of granuloma formation secondary to dermal filler: a multi-modality approach. J Cosmet Dermatol. 2023;22(4):1233–7.
50. Rozas-Muñoz E, Gamé D, Piquero-Casals J, Mir-Bonafé JF, Ocampo-López C, Madariaga JA. Persistent nose swelling in a teenage girl: answer. Am J Dermatopathol. 2022;44(12):1003–4.
51. Modarressi A, Nizet C, Lombardi T. Granulomas and nongranulomatous nodules after filler injection: different complications require different treatments. J Plast Reconstr Aesthet Surg. 2020;73(11):2010–5.
52. Mu EW, Stokar E, Franks L, Meehan SA. Histopathologic reaction patterns to differentially cross-linked hyaluronic acid fillers: a retrospective case series. J Cutan Pathol. 2021;48(6):758–62.
53. Agosti V, Stefanini G. Granulomatous reaction to hyaluronic acid dermal filler: clinical and histological features. Aesthetic Med. 2024;10(1):e2024002.
54. Vandeputte J, Leemans G, Dhaene K, Forsyth R, Vanslembrouck J, Hatem F, et al. Spreading pattern and tissue response to hyaluronic acid gel injections in the subcutis: ultrasound videos, ultrasound measurements, and histology. Aesthet Surg J. 2021;41(2):224–41.
55. Gonzalez C, Duque-Clavijo V, Kroumpouzos G, Garcia Concha AM, Olmos Perez M. Ultrasonographic features of nonvascular complications of hyaluronic acid fillers: a retrospective study at a reference center for dermatologic ultrasonography. Clin Dermatol. 2024;42(5):538–46.
56. Mlosek RK, Migda B. The use of high-frequency ultrasonography for the diagnosis of palpable nodules after the administration of dermal fillers. J Ultrason. 2020;20(83):248–53.
57. Mlosek RK, Skrzypek E, Skrzypek DM, Malinowska S. High-frequency ultrasound-based differentiation between nodular dermal filler deposits and foreign body granulomas. Skin Res Technol. 2018;24(3):417–22.
58. Signorini M, Liew S, Sundaram H, De Boulle KL, Goodman GJ, Monheit G, et al. Global Aesthetics Consensus: avoidance and management of complications from hyaluronic acid fillers—evidence- and opinion-based review and consensus recommendations. Plast Reconstr Surg. 2016;137(6):961e–71e.
59. Zein M, Tie-Shue R, Pirakitikulr N, Lee WWL. Complications after cosmetic periocular filler: prevention and management. Plast Aesthetic Res. 2020;7:44.
60. Trinh LN, McGuigan KC, Gupta A. Delayed granulomas as a complication secondary to lip augmentation with dermal fillers: a systematic review. Surg J. 2022;8(1):e69–79.
61. Kroumpouzos G, Harris S, Bhargava S, Wortsman X. Complications of fillers in the lips and perioral area: Prevention, assessment, and management focusing on ultrasound guidance. J Plast Reconstr Aesthet Surg. 2023;84:656–69.
62. Kroumpouzos G, Treacy P. Hyaluronidase for dermal filler complications: review of applications and dosage recommendations. JMIR Dermatol. 2024;7:e50403.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}