


Gabriele Harumi Seko1; Jéssica Pagan Faria1; Eldislei Mioto1; Luan Yudi Prando Kasuga2; Melissa Caroline Godoi Prestes2; Rogerio Nabor Kondo1
Funding: None
Conflict of interest: None
Submitted on: 03/04/2025
Final decision: 04/14/2025
Acknowledgments: We would like to thank Ricardo Kazuhito Yamamoto, ophthalmologist and member of the Brazilian Society of Ophthalmology, for the guidance he provided to the study from the point of view of ophthalmology.
How to cite this article: Seko GH, Faria JP, Mioto E, Kasuga LYP, Prestes MCG, Kondo RN. Quantitative and qualitative evaluation of upper blepharoplasty: a retrospective longitudinal study. Surg Cosmet Dermatol. 2025;17:e20250446.
INTRODUCTION: The eyelids have specific functions, such as eye protection. Aging can lead to excess upper eyelid skin (upper dermatochalasis), causing functional and aesthetic impairment. Subjective assessments of improvement pre- and post-blepharoplasty may be underestimated, since even small increases in palpebral fissure height (PFH) can improve the visual field.
OBJECTIVE: To measure PFH to check for improvements in dermatochalasis after upper blepharoplasty performed by dermatologists and compare the subjective assessments of independent dermatologists and patients.
METHODS: Medical record review of patients who underwent upper blepharoplasty. Photographs taken before and two months after the procedure were compared. Independent dermatologists evaluated the photographs (subjective assessment). Patients' subjective perception was also assessed. PFH before and after the procedure was calculated in millimeters (mm).
RESULTS: A total of 170 eyelids were analyzed. There were significant differences in mean PFH values before and after the procedure (7.088 vs. 8.618 mm; p < 0.001) and in patient self-assessment
(p = 0.001), but no differences between the subjective assessments by independent dermatologists (p = 0.665).
CONCLUSION: There was an improvement in mean PFH after blepharoplasty, which probably resulted in improved visual field. Dermatology is a specialty qualified to perform the procedure.
Keywords: Blepharoplasty; Eyelids; Skin Aging; Eye.
The eyelids are complex structures with specific functions, such as protecting the eyeball from trauma, shielding it from excessive light, and executing movements towards the tear drainage system, in addition to contributing to the eye's beauty and expression.1,2 Some factors, primarily chronological skin aging, may lead to loss of elasticity and excess upper eyelid skin (upper dermatochalasis), causing visual impairment and impacting periocular aesthetics.3 Lower dermatochalasis has greater impact on cosmetic appearance.4 Laser and radiofrequency may be used to treat dermatochalasis,5 but a surgical procedure (blepharoplasty) is still the most widely used technique, given its low cost and low invasiveness.3 Traditionally, ophthalmology and plastic surgery are the two medical specialties that perform blepharoplasties.3,4,6 However, given the current public health care scenario, both specialties are in high demand, leading to extremely long waiting lists for blepharoplasty. Dermatology, as a medical-surgical specialty, can also perform the procedure, and having dermatologists perform blepharoplasties is an alternative to help reduce waiting times.7 In addition, it would be important to assess whether dermatology is able to achieve satisfactory postoperative outcomes. However, considering the subjective assessment of primary surgeons themselves alone would be suboptimal, and including the assessment of other physicians, combined with objective evaluation, would lower potential performance biases.3,6 A previous study proposed assessing the surgical outcomes of upper blepharoplasty performed by dermatologists objectively by comparing pre- and postoperative measures of palpebral fissure height (PFH).3 However, that study had a limited sample size (only nine patients) and suggested additional studies should be conducted.3 The aim of the present study was to determine if there was any improvement in dermatochalasis after upper blepharoplasty performed by a local dermatology service, thus investigating the qualification of that specialty to perform the procedure. The improvement was assessed both quantitatively, by comparing pre- and postoperative PFH measures, and qualitatively, based on the pre- and postoperative subjective assessments by independent dermatologists and the patients themselves.
A retrospective longitudinal study reviewed the medical records and photographs of patients who underwent upper blepharoplasty performed at the dermatology service of the university where the study was conducted.
The patient inclusion criteria for this study were having undergone upper blepharoplasty at the dermatology service between April 1, 2014, and March 31, 2023. The exclusion criteria, in turn, were absence of return after surgical procedure, lack of data that could not be obtained through invitations or by telephone, photographs taken by professionals other than the lead investigator, and use of cameras other than a Canon T3i.
Photographs taken at a standardized distance of 50 cm with a Canon® T3i camera and 55 mm macro lens, before the procedure and 2 months after, were compared using the Scion Image 4.0 software. PFH, defined as the distance from the upper eyelid to the lower eyelid passing through the pupil, was calculated based on the stored photographs (Figure 1). The Pixel Converter software application was used to convert pixels into millimeters, using decimal thousandths to assign the PFH values in millimeters.
The photographs taken before and after the procedures were distributed to three independent dermatologists for assessment, without telling the specialists which had been taken before and which after the procedure (photograph A vs. photograph B). Next, the professionals assigned a numerical score comparing the evolution of photograph A to B and of photograph B to A, according to the following scale developed by the researchers: significant worsening (-3), moderate worsening (-2); mild worsening (-1), no change or no improvement (0), mild improvement (+1), moderate improvement (+2), and significant improvement (+3). Only the researchers knew that, for instance, a -3 score might actually indicate a +3 improvement. Patients' subjective assessments were also scored based on functional (visual field) and/or aesthetic improvement, using the following scale: improvement (+1), no improvement (0), and worsening (-1).
The data were provided via survey forms developed by the researchers themselves. The information collected was compiled into a Microsoft Excel spreadsheet for statistical analysis using the Stata® (version 13.0, StataCorp, Texas) and Jamovi software applications. Fisher's exact test was used to compare categorical variables and the chi-square test for trends. Continuous variables were analyzed using the Wilcoxon-Mann-Whitney test. After checking the normality of quantitative variables using the Shapiro-Wilk test, nonparametric Mann-Whitney and Kruskal-Wallis tests were used to compare the results. Statistical significance was set at p < 0.05, with a 95% confidence interval. The minimum sample size calculation resulted in 170 eyelids (85 patients), considering a significant difference of at least 0.900 mm in PFH between pre- and post-blepharoplasty measurements, with a significance level of 5%, power of 80%, and a standard deviation of 0.300 mm.
The study was approved by the Human Research Ethics Committee of the hospital where the study was conducted, and received Certificate of Presentation for Ethical Evaluation number 69513623.0.0000.5231.
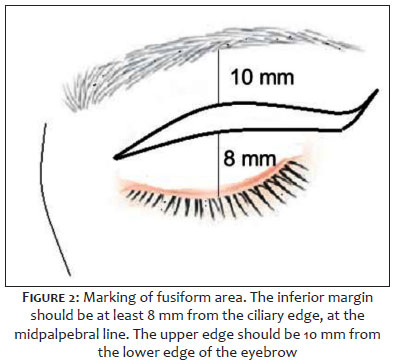
a) With the patient in horizontal supine position and eyes closed, a fusiform marking of the skin to be excised was made using a surgical marking pen or methylene blue. The lower limit was drawn at a distance greater than 8 mm from the lash line, and the upper limit of the fusiform area was marked more than 10 mm from the lower edge of the eyebrow (measures adopted to avoid lagophthalmos).1 At the lateral ends, a slight arching was performed. (Figure 2)
B) Antisepsis with topical 10% polyvinyl-iodine solution;
C) Subcutaneous infiltration of upper eyelid with 2% lidocaine and vasoconstrictor;
D) Incision of the marked area with a 15 blade and excision of tissue to subcutaneous depth;
E) Hemostasis;
F) Sutures with 6-0 Mononylon, single stitches;
G) Cleaning and dressing with sterile Micropore tape.
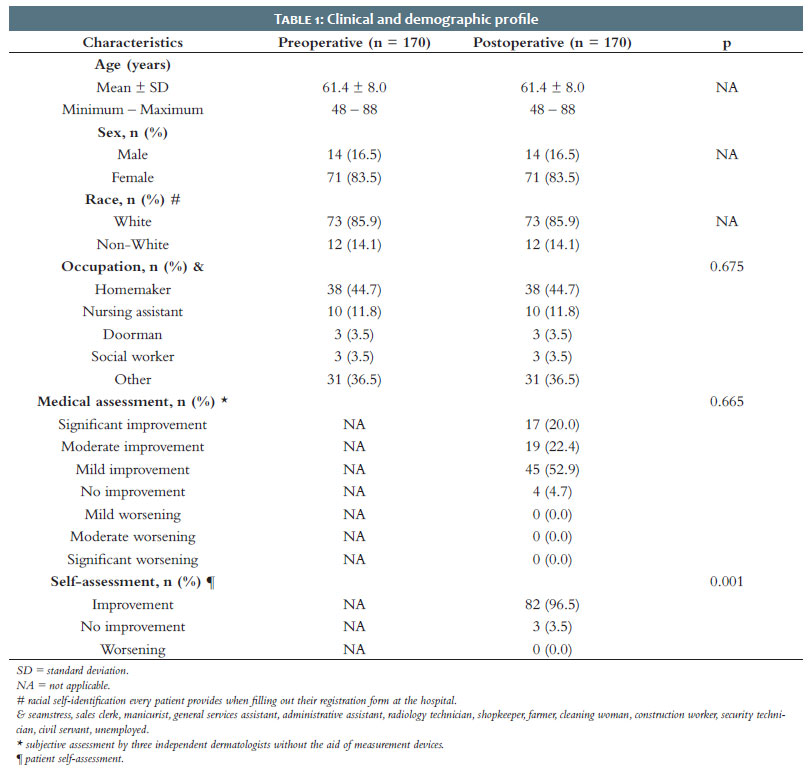
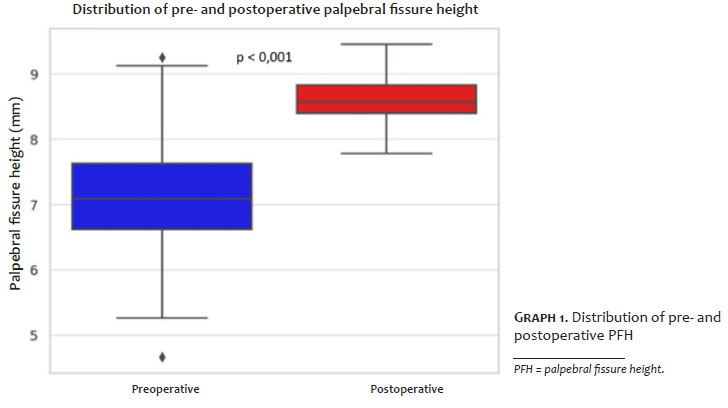
Table 1 lists the main findings of the present study. The study analyzed 170 eyelids of 85 individuals, with mean age of 61.4 years, predominantly female (83.5%) and White (85.9%). There was a significant difference in mean pre- and post-blepharoplasty PFH (7.088 vs. 8.618 mm; p < 0.001). Graph 1 compares pre- and postoperative PFH measurements.
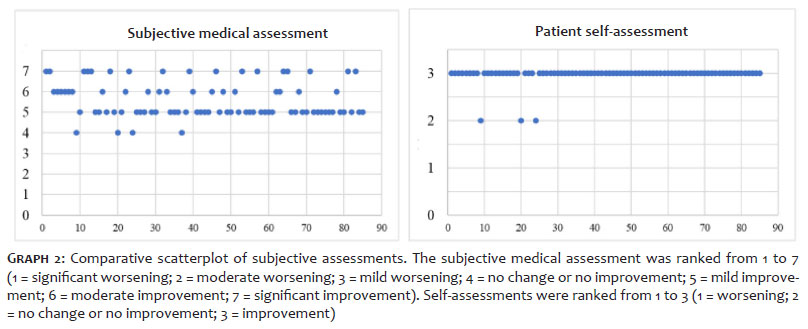
For dermatologists, a subjective assessment of mild improvement (52.9%) predominated over all other findings (47.2%) (p = 0.665). Comparing rates of improvement vs. non-improvement, the post-blepharoplasty outcome was significant (94.3 vs. 4.7%; p = 0.001). In patient self-assessments, however, a significant improvement was found (96.5 vs. 3.5%; p = 0.001). Graph 2 shows the assessments of dermatologists and patients.
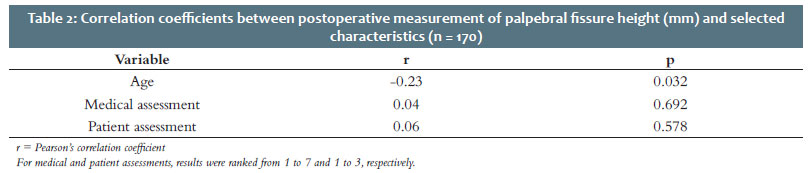
Regarding PFH correlations after blepharoplasty, there was an inverse correlation with patient age (r = -0.230; p = 0.032). Dermatologists' assessments and patient self-assessments were not significantly correlated with post-blepharoplasty PFH (p > 0.05) (Table 2). However, comparing dermatologists' assessments to patient self-assessments (disregarding PFH measurements), the result was statistically significant (r = 0.351; p < 0.001).
The sample was predominantly comprised of female patients, with mean age higher than 60 years, consistent with the literature.8,9 Mean preoperative PFH was 7.088 mm and mean postoperative PFH was 8.618 mm (p < 0.001), values close to those found by Schellini et al.3 Mean PFH without dermatochalasis, ie, in the young adult population, can vary by race, country, and sex. A Turkish study found an average of 10.4 mm for females and 10.3 mm for males.10 There are no consolidated data on mean post-blepharoplasty PFH. However, Schellini et al.3 report a postoperative mean PFH of 7.92 mm for nine patients, also smaller than the mean average observed in individuals without dermatochalasis, and similar to the results of the present study. Subjective assessments by dermatologists and patient self-assessments were not correlated with postoperative PFH (p > 0.05). The authors considered the hypothesis that pre- and post-blepharoplasty comparisons are barely perceptible to the naked eye, given that no assessment indicated a worsening (p < 0.05). That finding might suggest that even small improvements in PFH, measured in millimeters, would favor visual acuity. Visual field tests are the standard examination to assess the visual field before and after a blepharoplasty. However, that test depends on information provided by the patient and is also a subjective parameter.8 This test was not performed in our study, as was also the case in the work of Schellini et al. Surgical indication was based on the patient's complaint and the physical examination of excess upper eyelid skin. To date, there are no studies in the plastic surgery literature that employ PFH or some other objective measurement to assess upper blepharoplasty. Furthermore, no study has concomitantly applied three methods of assessing surgical outcomes (PFH, assessment by independent specialists, and patient self-assessment). Study limitations include the absence of visual field tests, which could have provided additional information, and the fact that it was conducted in a single referral center. In addition, 10 patients had to be excluded due to information bias, with 10 others from the consecutive listing included to maintain the sample size. Despite these limitations, the authors replicated a quantitative assessment (PFH)3 and compared it to qualitative parameters, finding superior postoperative outcomes in a more objective manner, evidence that dermatology may also be qualified to perform upper blepharoplasty.
By analyzing a quantitative parameter (PFH), the present study found a significant improvement in patients who underwent upper blepharoplasty performed at a dermatology service, indicating that the specialty may also be qualified to perform this type of procedure.
Gabriele Harumi Seko
ORCID: 0000-0001-6661-4070
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature; Critical revision of the manuscript.
Jéssica Pagan Faria
ORCID: 0000-0001-8727-2348
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Eldislei Mioto
ORCID: 0000-0001-5376-9292
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Luan Yudi Prando Kasuga
ORCID: 0009-0006-3724-0034
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Melissa Caroline Godoi Prestes
ORCID: 0009-0005-3710-9995
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
1. Kondo RN, Singh BS, Ferreira VP, Araújo MCP. Upper eyelid transposition flap for reconstruction of a lower eyelid defect: a case report. Surg Cosmetic Dermatol. 2022;14:e20220156.
2. Zhou J, Ding J, Li D. Blepharochalasis: clinical and epidemiological characteristics, surgical strategy and prognosis -- a retrospective cohort study with 93 cases. BMC Ophthalmol. 2021;21(1):313.
3. Schellini SA, Preti RC, Yamamoto RK, Padovani CR, Padovan CR. Eyelid measures before and after upper blepharoplasty -- quantitative evaluation. Arq Bras Oftalmol. 2005;68(1):85-8.
4. Fagien S. Advanced rejuvenative upper blepharoplasty: enhancing aesthetics of the upper periorbita. Plast Reconstr Surg. 2002;110(1):278-91.
5. Biesman BS. Blepharoplasty: laser or cold steel? Skin Therapy Lett. 2003;8(7):5-7.
6. Lima CG, Siqueira GB, Cardoso IH, Sant'Anna AE, Osaki MH. Evaluation of dry eye in the preoperative and postoperative period of blepharoplasty. Arq Bras Oftalmol. 2006;69(3):377-82.
7. Scawn R, Gore S, Joshi N. Blepharoplasty basics for the dermatologist. J Cutan Aesthet Surg. 2016;9(2):80-4.
8. Pemberton JD, Salter M, Fay A, Thuro B, Spencer H, Dajani O. Investigation of goldmann perimetry in evaluation of patients for upper eyelid blepharoplasty. Orbit. 2018;37(1):48-52.
9. Homer NA, Zhou S, Watson AH, Durairaj VD, Nakra T. Wound dehiscence following upper blepharoplasty: a review of 2,376 cases. Ophthalmic Plast Reconstr Surg. 2021;37(3S):S66-9.
10. Bozkir MG, Karakaş P, Oĝuz O. Measurements of soft tissue orbits in Turkish young adults. Surg Radiol Anat. 2003;25(1):54-7.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}