


Marina Soares Silverio; Daniel Simão de Andrade; Carolina Malavassi Murari; Rossana Cantanhede Farias de Vasconcelos; Fernanda Rytenband
Funding: None.
Conflict of interest: None.
Submitted on: 11/27/2024
Final decision: 04/10/2025
How to cite this article: Silverio MS, Andrade DS, Murari CM, Vasconcelos RCF, Rytenband F. Combination of chemical peels and oral isotretinoin in the treatment of acne scars. Surg Cosmet Dermatol. 2025;17:e20250427.
INTRODUCTION: Acne is a prevalent chronic disease that can cause physical, emotional, and social effects. Isotretinoin and chemical peels are available as treatment, but their combination has historically been avoided due to reports of abnormal healing. Recent studies suggest that the combination with superficial or medium-depth peels is safe, but there are no studies considering the specific characteristics of the Brazilian population.
OBJECTIVE: To evaluate the safety and efficacy of combining isotretinoin and chemical peels in the treatment of
acne scars.
METHODS: A clinical trial was conducted with patients aged 15 to 25 years undergoing acne treatment with isotretinoin. The intervention group underwent three Jessner's peels during isotretinoin use, while the control group underwent the same peels after treatment with isotretinoin was completed. Outcomes were assessed using the QGSGS and IGA scales by two blinded evaluators.
RESULTS: Peels performed concomitantly with isotretinoin did not result in worse outcomes on the QGSGS and IGA scales compared to the control group.
CONCLUSION: The combination of isotretinoin and chemical peels proved to be safe, but further studies with larger samples are needed to establish recommendations.
Keywords: Acne Vulgaris; Isotretinoin; Chemexfoliation.
Acne vulgaris is the eighth most common disease globally, affecting over 0.5 billion people,1 and it is estimated that 50% to 95% of adolescents have some degree of the disease. It is classified as a chronic inflammatory disorder of the pilosebaceous unit, and its pathogenic basis involves the following mechanisms: increased and abnormal sebum production under androgenic influence; altered keratinization leading to comedone formation; follicular colonization by Cutibacterium acnes (C. acnes); and the release of inflammatory mediators in the skin such as interleukin-1 alpha and TNF-alpha.2 In addition to acne vulgaris, there is also adult female acne, characterized by acne affecting women aged 25 years and older and which may persist from adolescence or begin in adulthood.
With regard to etiopathogenesis, this condition differs from acne vulgaris in its strong hormonal influence, involving alterations in androgen metabolism, worsening during the premenstrual period, and greater association with endocrinological disorders such as polycystic ovary syndrome, late-onset congenital adrenal hyperplasia, hyperinsulinism, and peripheral insulin resistance. In addition, it presents a tendency to relapse, requiring a different therapeutic approach compared to acne vulgaris as well as making maintenance treatment essential.3 The condition causes painful lesions and may lead to scarring in up to 95% of patients with the disease,4 leading to physical, emotional, and social impairment. It carries a high global disease burden and, among dermatological diagnoses, accounts for the second highest impact on DALYs (disability-adjusted life years, or the number of years of life lost due to premature death and disability), behind only eczema, and surpassing conditions such as urticaria, psoriasis, and a number of infections.5
To prevent unfavorable outcomes, it is important that effective treatments be initiated promptly. The main treatments for mild acne vulgaris include topical retinoids, benzoyl peroxide, topical antibiotics, salicylic acid, and azelaic acid. Isotretinoin, systemic antibiotics, and hormonal agents such as oral contraceptives and spironolactone may be used to treat moderate to severe acne. Even recent guidelines such as the American Academy of Dermatology's "Guidelines of care for the management of acne vulgaris"6 describe the current evidence for other forms of treatment, such as chemical peels, photodynamic therapy, lasers, and mechanical extraction, as insufficient to warrant a recommendation.
Isotretinoin (13-cis-retinoic acid), a vitamin A derivative, approved for use in the United States in 1982 and in Brazil in 1990, stands out as one of the main forms of treatment. It has been widely used since then, and is currently indicated for nodulocystic acne, moderate papulopustulosa acne resistant to other treatments, acne with a tendency to scarring, and cases associated with social and emotional impairment. As monotherapy, it can induce remission in approximately 80% of patients.7 The mechanisms of action against acne include the involution of the pilosebaceous unit,8 normalization of infundibular hyperkeratinization,7 immunomodulation with decreases in TNF-alpha, interleukin-4, interleukin-17, and interferon gamma levels,9 and decreases in populations of C. acnes.7 Isotretinoin is thus considered a first-line treatment, as it can treat acne effectively, prevent scarring, and promote rapid improvements in patient quality of life.
The most common adverse effects of isotretinoin are cheilitis, occurring in 94% to 100% of users, and xeroderma, or mucosal dryness, in 47% of cases. In general, neither requires the medication be discontinued, and both can be easily managed with topical moisturizers and ocular or nasal lubricants. Less frequent events include conjunctivitis, hair loss, brittle nails, pyogenic granulomas, headache, and myalgia.10 Laboratory abnormalities occurred in 2% of patients, primarily hypertriglyceridemia, elevated cholesterol, and elevated transaminases.11
However, all these adverse effects are dose-dependent and tend to normalize after treatment is discontinued. The most serious risk, which is dose-independent, is teratogenicity; pregnancies may result in miscarriage in up to 20% of cases and embryopathies in up to 28%.7 Therefore, the drug is contraindicated in pregnant women, and requires effective contraception and testing to rule out pregnancy in women of childbearing age. Another reported adverse effect is a potential increase in the risk of depression and suicide. However, a 2007 systematic review found no evidence to support this theory,12 and some studies have even observed a trend toward a reduction in depressive symptoms during treatment with isotretinoin.2 The literature also discusses the possibility of abnormal scarring after surgical or cosmetic procedures.
Currently, the isotretinoin label contraindicates aggressive dermabrasion, chemical peels, and laser skin treatments for 5 to 6 months after completing treatment. This recommendation is due to the risk of hypertrophic scarring in atypical areas, as well as hyper or hypopigmentation in treated areas.13 The change to the label was based on three small case series published in the 1980s, which reported keloid formation and delayed healing in a total of 11 patients following dermabrasion and argon laser treatment.14 The hypotheses suggested for this alteration in healing were that angiogenesis stimulation or the production of collagenase inhibitors would result in collagen accumulation.15 However, since then, several animal studies have shown similar wound healing rates between intervention and control groups.8
In support of the idea that wound healing occurs normally in patients undergoing isotretinoin treatment, a Brazilian retrospective observational study concluded that: (1) no significant differences in the prevalence of keloids or hypertrophic scars were observed between isotretinoin users and non-users; (2) there was no worsening of preexisting keloids in patients on the medication; and (3) a retrospective analysis of patients with keloids found a low prevalence of prior isotretinoin use.16 The contraindication against performing certain adjuvant procedures during isotretinoin treatment runs counter to excellence in care, since patients with acne severe enough to require isotretinoin are precisely those who could benefit most from cosmetic procedures.8
Given the current availability of minimally invasive procedures such as microdermabrasion, microneedling, fractional lasers, and superficial peels, it is necessary to revisit old recommendations. Among adjuvant therapies for acne, chemical peels stand out due to their advantages; they are relatively affordable compared to new technologies, can be performed at the physician's office, and involve minimal downtime.17
Several formulations may be used as chemical peels, aiming to induce controlled therapeutic exfoliation of the skin. This results in partial or complete renewal of the epidermis, and may or may not reach the dermis, and is thus indicated for the treatment of pigmentation disorders and skin irregularities. In acne-prone skin, peels may be used both during the active phase of the disease, targeting comedones and inflammatory lesions, and during the healing phase, to reduce hyperchromias and scarring.
Because it works during both phases, Jessner's peel, consisting of a solution of 14% salicylic acid, 14% resorcinol, and 14% lactic acid in 95% ethanol, is widely used. Salicylic acid has a sebosuppressive, keratolytic, and anti-inflammatory effect18; resorcinol is keratolytic; and lactic acid reduces hyperchromias, being safe even for darker skin.19 It can act as superficial to medium-depth peels depending on the number of applied layers, and the main adverse effects are the risk of contact dermatitis from resorcinol, with consequent post-inflammatory hyperpigmentation. Thus, its use requires caution in patients with higher Fitzpatrick skin phototypes.17
Some studies have analyzed the safety of chemical peels during oral isotretinoin therapy and found similar or even better aesthetic outcomes when both treatments were combined.8,18,20-22 This has led to the inclusion of superficial chemical peels among therapeutic options for isotretinoin users in major guidelines such as the 2017 Consensus of the American Society for Dermatologic Surgery (ASDS)8 and the 2019 Brazilian Consensus on isotretinoin use.7 However, there is still a lack of studies in the Brazilian population, which has unique skin characteristics. In addition, some recent guidelines, such as the "Guidelines of care for the management of acne vulgaris" from the American Academy of Dermatology,6 state that while there is no evidence in the literature to contraindicate chemical peels in patients with acne, there is also no evidence to recommend them. Therefore, further studies are needed on the subject.
In summary, acne is a chronic and disfiguring disease with a major impact on patients' lives. It is therefore crucial to initiate effective treatments promptly and not postpone adjuvant procedures that can prevent scarring, which means chemical peels represent a valuable addition to the therapeutic arsenal alongside isotretinoin. However, due to previous recommendations against using both treatments concurrently, many physicians still postpone peels until after the disease has resolved. Given the paucity of literature on the subject, this study aims to gather evidence to support the use of peels in combination with isotretinoin, taking into account the specific skin characteristics of the Brazilian population.
This research project involving human subjects was submitted to the Research Ethics Committee of Universidade Santo Amaro and approved under protocol no. 7.004.647. It is a controlled, open-label clinical trial with blinded evaluators, to be conducted during 2024 at Complexo de Saúde Dr. Wladimir de Arruda, located at Rua Cássio de Campos Nogueira, 2031, in São Paulo (SP), Brazil. Participants were randomly assigned to two groups: one group underwent three Jessner's peels concomitantly with isotretinoin use, at a frequency of one peel per month for three months (4th, 5th, and 6th months of treatment); the other group underwent three Jessner's peels after completing isotretinoin treatment, on the 3rd, 4th, and 5th months following discontinuation of the medication. Throughout the isotretinoin and peeling treatment period, patients were instructed to use sunscreen (SPF 50 or higher) every day. If patients did not already have a preferred product, sunscreen was provided by the study. Peels were performed in the following steps:
Photographic documentation;
Skin degreasing with alcohol;
Application of three layers of Jessner's solution using gauze, with a three-minute interval between each application;
Removal with water after three minutes.
Throughout the study, patients were able to contact the investigators in case of complications. All patients at the service were photographed before initiation of treatment; images were archived in electronic medical records and made available for research purposes with patient consent. At the end of treatment, additional photographs were taken using the following standard views: frontal face, full right profile, full left profile, right semi-profile, and left semi-profile. After the interventions, patients' before and after photographs were scored by two blinded evaluators using the Quantitative Global Scarring Grading System for Post-acne Scarring (QGSGS) and Investigator Global Assessment (IGA) scales.23 Both evaluators were dermatologists with no access to patient identification data or to which group patients were assigned. Finally, scores were analyzed statistically to determine which group attained greater improvement in facial acne scars.
The product used in the procedures was:
Jessner's peel: 14% salicylic acid, 14% resorcinol, 14% lactic acid, 95% ethanol. Compounded formulation – Farmácia Drogaderma (CNPJ 43.342.542/0002-36); Application: 546095; Registration: 1656844. Pharmacist in charge: Dr. Marcio Nogueira Garcia (CRF-SP: 39016). Prescribing physician: Marina Soares Silvério (CRM-SP: 231.782).
INCLUSION CRITERIA
All patients aged 15 to 24 years seen at the Dermatology Service of Universidade Santo Amaro, diagnosed with grade 2 or 3 acne, and already receiving oral isotretinoin treatment independently of this study were invited to participate. In addition, participants were required to read and sign both the Informed Consent Form and the Image Use Authorization Form.
Pregnant patients or those planning to get pregnant during the study or within the subsequent 6 months, patients younger than 15 years or aged 25 years and older, and individuals who did not agree to sign the Informed Consent Form or the Image Use Authorization Form were excluded from the study. During the study, patients who failed to attend scheduled appointments or who did not adhere to isotretinoin treatment as prescribed were also excluded.
The QGSGS and IGA scales were applied to photographs taken of each patient at the beginning of treatment and upon completion. Assessments were performed by blinded evaluators, two dermatologists who did not take part in the intervention stages and were not informed about to which group each patient had been assigned. Scores were then analyzed statistically to compare patients in the intervention and control groups. The Mann–Whitney test24 was used to compare variables between intervention and control groups, and the Wilcoxon signed-rank test24 to compare the periods before and after treatment.
During the recruitment stage, a total of 46 patients agreed to take part in the study. Of these, 21 patients completed all study stages: 12 in the intervention group (4 male and 8 female; 9 aged 15–19 years and 3 aged 20–25 years) and 9 in the control group (7 male and 2 female; 6 aged 15–19 years and 3 aged 20–25 years). Discontinuing treatment due to severe adverse events related to either the peels or isotretinoin use was not necessary for any patient. The main reasons for patient exclusion were discontinuation of isotretinoin treatment (8 patients across both groups); missing scheduled appointments (9 patients across both groups); completion of isotretinoin treatment but unwillingness to undergo peels afterward (3 patients in the control group); undergoing other aesthetic facial procedures concurrent with the study (3 patients across both groups); and continued isotretinoin use at the time of study completion (2 patients in the control group). In addition to statistical analysis, representative patient photographs from each group were included, standardized before and after treatment, to illustrate the clinical progression observed (Figures 1 and 2).
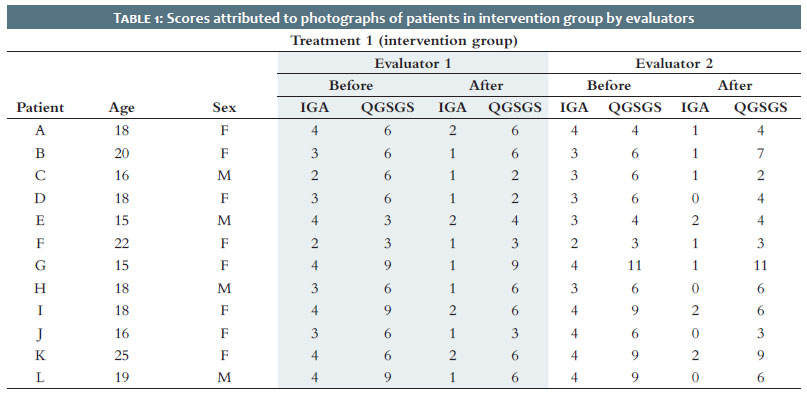
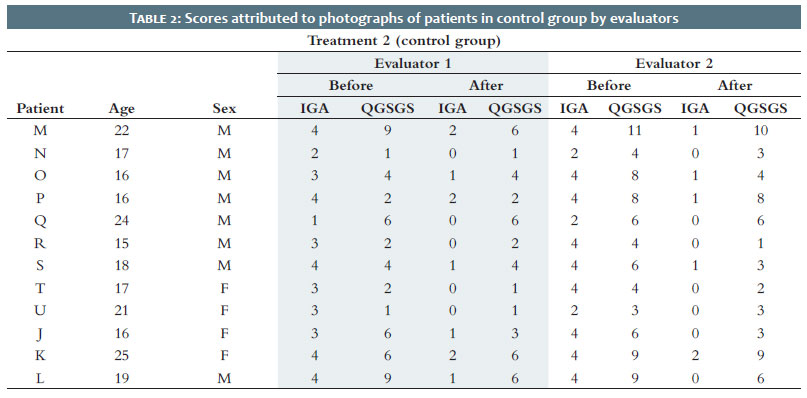
The scores for before and after photographs for both groups as assessed using the IGA and QGSGS scales by the evaluators (Evaluator 1 and Evaluator 2) can be found in Table 1 and Table 2.
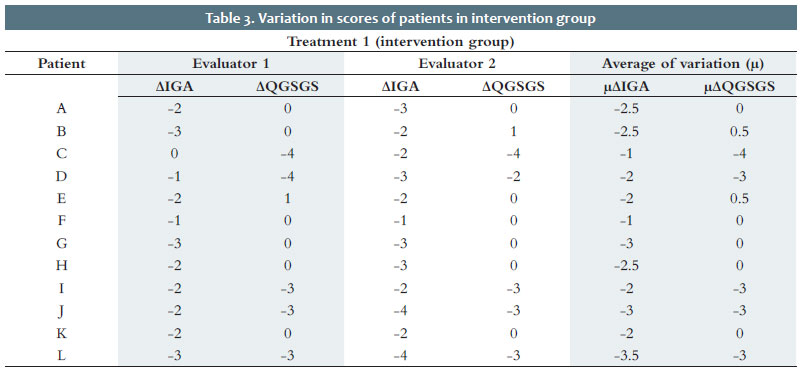
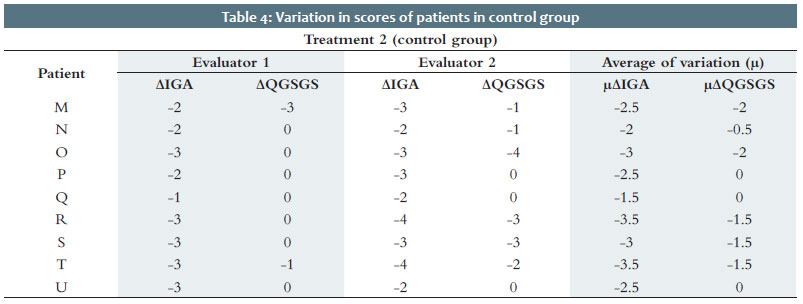
Regarding the characteristics of the study groups, the difference in sample size (n) between groups stands out, as well as the heterogeneity of its composition in terms of sex: the intervention group included 4 male and 8 female patients, while the control group included 7 male and 2 female patients. This discrepancy between the two groups resulted from simple randomization but also mainly from the need to exclude individuals who chose to withdraw from the study or who did not meet project requirements (missed appointments, failure to complete the tests required to maintain isotretinoin use, undergoing other treatments that could interfere with outcomes, among others). Therefore, the composition of the sample can be considered a potential source of bias. Based on these scores, the variation in IGA and QGSGS scores before and after treatment was also calculated for each patient, resulting in ∆IGA and ∆QGSGS values, quantifying the degree of improvement or worsening of acne lesions and scars for each patient. From these data, the average of variations in scores (μ) was calculated using the scores from both evaluators, resulting in μ∆IGA and μ∆QGSGS, as shown in Table 3 and Table 4.
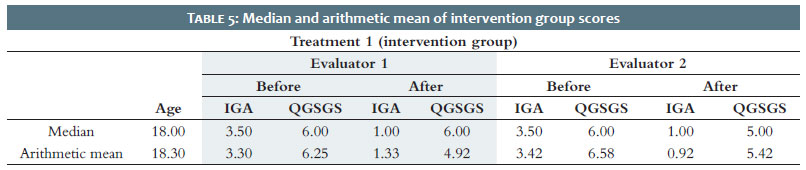
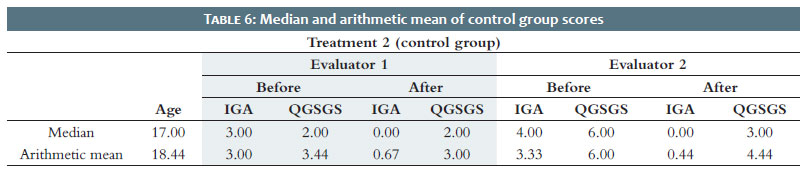
A preliminary analysis indicated that most scores had neutral or negative results. This means there was a decrease in the number of lesions (measured by IGA) and scars (measured by QGSGS) for both intervention and control group patients. Exceptionally, Patient E showed an increase in QGSGS assigned by Evaluator 1, and Patient B showed an increase in QGSGS assigned by Evaluator 2. A possible explanation for the increases in QGSGS for these two outliers is that active acne lesions may interfere with the initial assessment of preexisting scars, leading to an artificially low initial QGSGS score. The median and arithmetic mean of scores are shown in Table 5 and Table 6.
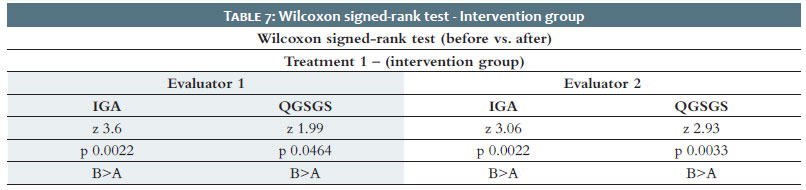
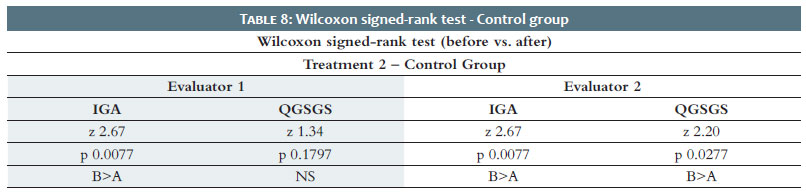
Initially, the Wilcoxon signed-rank test was applied to compare the before and after treatment datasets, as shown in Table 7 and Table 8.
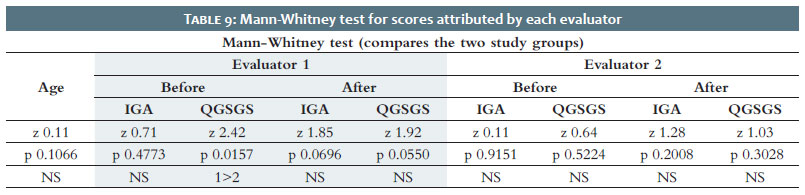
The test showed that IGA and QGSGS values were higher before treatment than after for both groups and for both evaluators, with statistical significance, except for QGSGS in the control group according to Evaluator 1. The data confirm the expected hypothesis that both treatments promoted improvements in skin quality for patients, resulting in fewer acne lesions (measured by IGA) and fewer scars (measured by QGSGS). Although this outcome was anticipated, it is worth emphasizing that the peels were not harmful to patients and may have had a neutral or beneficial effect. The Mann-Whitney test was also applied, resulting in the comparative analysis shown in Table 9.
The first piece of data shown in Table 9 is that participants in both groups had similar ages. It can also be observed that when comparing the intervention and control group scores, there were no statistically significant differences for the following parameters: IGA before (Evaluator 1), IGA after (Evaluator 1), QGSGS after (Evaluator 1), IGA before (Evaluator 2), QGSGS before (Evaluator 2), IGA after (Evaluator 2), and QGSGS after (Evaluator 2). This enables us to infer that performing Jessner's peels during isotretinoin treatment likely did not significantly influence the variation in patient IGA and QGSGS scores. A single statistically significant difference was observed when comparing QGSGS before values according to Evaluator 1, with higher scores in the intervention group. This may indicate a selection bias, with patients randomized to the intervention group having more severe scarring before starting treatment. However, the scores assigned by Evaluator 2 did not corroborate these data.
It is also worth noting that the number of participants in this study was small. With larger groups, results might have been statistically significant. When the Mann-Whitney test was applied to the average of variations in scores between before and after photographs, no significant differences were found between groups either, as shown in Table 10.
This study allows us to conclude that the use of Jessner's chemical peel as an adjuvant to isotretinoin therapy for acne at different moments (during or after isotretinoin treatment) did not have harmful effects. Both the intervention and control groups showed statistically significant improvements in acne and scar reduction at the end of the study. The peels may have had neutral or beneficial effects. Therefore, there is no reason Jessner's peels should be contraindicated during isotretinoin therapy. However, it was not possible to determine when peels should be performed, as no statistically significant differences were found between study groups. Further studies are required to establish a solid base to support recommending the use of Jessner's peels as part of standard treatment.
Marina Soares Silverio
ORCID: 0009-0005-0039-1667
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Daniel Simão de Andrade
ORCID: 0009-0003-4002-5288
Approval of the final version of the manuscript; Acquisition, analysis and interpretation of data; Critical revision of the manuscript.
Carolina Malavassi Murari
ORCID: 0000-0001-6688-5145
Approval of the final version of the manuscript; Acquisition, analysis and interpretation of data; Critical revision of the manuscript.
Rossana Cantanhede Farias de Vasconcelos
ORCID: 0000-0002-6185-1840
Approval of the final version of the manuscript; Critical revision of the manuscript.
Fernanda Rytenband
ORCID: 0000-0002-2882-1658
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
1. Mavranezouli I, Daly CH, Welton NJ, Deshpande S, Laura B, Bromham N, et al. A systematic review and network meta-analysis of topical pharmacological, oral pharmacological, physical and combined treatments for acne vulgaris. Brit J Dermatol. 2022;187(5):639-49.
2. Simonart T. Newer approaches to the treatment of acne vulgaris. Am J Clin Dermatol. 2012;13(6):357-64.
3. Bagatin E, Freitas THP, Machado MCR, Ribeiro BM, Nunes S, Rocha MAD. Adult female acne: a guide to clinical practice. An Bras Dermatol. 2019;94(1):62-75.
4. Cachafeiro TH, Escobar GF, Maldonado G, Cestari TF. Translation into brazilian portuguese and validation of the "quantitative global scarring grading system for post-acne scarring". An Bras Dermatol. 2014;89(5):851-3.
5. Institute for Health Metrics and Evaluation (IHME). Global burden of disease 2021: findings from the GBD 2021 study. Seattle, WA: IHME; 2024.
6. Strauss JS, Krowchuk DP, Leyden JJ, Lucky AW, Shalita AR, Siegfried EC, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2007;56(4):651-63.
7. Bagatin E, Costa CS, Rocha MAD, Picosse FR, Kamamoto CSL, Pirmez R, et al. Brazilian Society of Dermatology consensus on the use of oral isotretinoin in dermatology. An Bras Dermatol. 2020;95(Suppl 1):19-38.
8. Waldman A, et al. ASDS Guidelines Task Force: consensus recommendations regarding the safety of lasers, dermabrasion, chemical peels, energy devices, and skin surgery during and after isotretinoin use. Dermatol Surg.2017;43(10):1249-62.
9. Karadag AS, Ertugrul DT, Bilgili SG, Takci Z, Akin KO, Calka O. Immunoregulatory effects of isotretinoin in patients with acne. Brit J Dermatol. 2012;167(2):433-5.
10. Brito MFM, Sant'Anna IP, Galindo JCS, Rosendo LHP, Santos JB. Evaluation of clinical adverse effects and laboratory alterations in patients with acne vulgaris treated with oral isotretinoin. An Bras Dermatol. 2010;85(3):331-7.
11. Costa CS, Bagatin E, Martimbianco ALC, Silva EMK, Lúcio MM, Magin P, et al. Oral isotretinoin for acne. Cochrane Database of Syst Rev. 2018;11(11): CD009435.
12. Marqueling AL, Zane LT. Depression and suicidal behavior in acne patients treated with isotretinoin: a systematic review. Semin Cutan Med Surg. 2007;26(4):210-20.
13. Roacutan (isotretinoína): produtos Roche Químicos e Farmacêuticos S.A: capsulas gelatinosas: 20 mg. [Bula para pacientes]. Eberbach, Alemanha: Roche; 2022.
14. Spring LK, Krakowski AC, Alam M, Bhatia A, Brauer J, Cohen J, et al. Isotretinoin and timing of procedural interventions. JAMA Dermatol. 2017;153(8):802-9.
15. Picosse FR, Yarak S, Cabral NC, Bagatin E. Early chemabrasion for acne scars after treatment with oral isotretinoin. Dermatol Surg. 2012;38(9):1521-6.
16. Guadanhim LRS, Gonçalves RG, Bagatin E. Observational retrospective study evaluating the effects of oral isotretinoin in keloids and hypertrophic scars. Int J Dermatol. 2016;55(11):1255-8.
17. Handog EB, Datuin MSL, Singzon IA. Chemical peels for acne and acne scars in asians: evidence based review. J Cutan Aesthet Surg. 2012;5(4):239-46.
18. Chandrashekar BS, Vadlamudi SR, Shenoy C. Safety of performing superficial chemical peels in patients on oral isotretinoin for acne and acne-induced pigmentation. J Clin Aesthetic Dermatol. 2021;14(11):41-3.
19. Yokomizo VMF, Benemond TMH, Chisaki C, Benemond PH. Chemical peels: review and practical applications. Surg Cosmet Dermatol. 2013;5(1):58-68.
20. Mysore V, Mahadevappa OH, Barua S, Majid I, Viswanath V, Bhat RM, et al. Standard guidelines of care: performing procedures in patients on or recently administered with isotretinoin. J Cutan Aesthet Surg. 2017;10(4):186-94.
21. Mahadevappa OH, Mysore V, Viswanath V, Thurakkal S, Majid I, Talwar S, et al. Surgical outcome in patients taking concomitant or recent intake of oral isotretinoin: a multicentric study-iso-aims study. J Cutan Aesthet Surg. 2016;9(2):106-14.
22. Kar BR, Tripathy S, Panda M. Comparative study of oral isotretinoin versus oral isotretinoin + 20% salicylic acid peel in the treatment of active acne. J Cutan Aesthet Surg. 2013;6(4):204-8.
23. Bae IH, Kwak JH, Kim MS, Shin BS, Choi H.Comprehensive review of the acne grading scale in 2023. Ann Dermatol. 2024;36(2):65-73.
24. Siegel S, Castellan Jr NJ. Estatística não-paramétrica para ciências do comportamento. 2nd. ed. Porto Alegre: Artmed; 2006. 448 p.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}