


Adriana Vilarinho1; Alessandra Haddad2,3; Cintia Cunha4; Fernanda Nunes1; Maria Paula Del Nero1; Taciana Dal'Forno5
Funding: Galderma provided support for the board formation and manuscript writing.
Conflict of interest: Dr. Dal’Forno, Dr. Nunes, and Dr. Cunha report serving as consultants for Galderma. Dr. Del Nero reports serving as a speaker, advisor, and consultant for Galderma. Dr. Haddad reports serving as a speaker, consultant, advisor, and researcher for Galderma. *Dr. Vilarinho is a dermatologist who contributed to this manuscript solely for educational purposes, based on her professional expertise. She declares no conflicts of interest and no institutional relationship with Galderma. No author received financial compensation or any form of remuneration for participation in the preparation of this manuscript.
Submitted on: 03/07/2024
Final decision: 07/07/2025
How to cite this article: Vilarinho A, Haddad A, Cunha C, Nunes F, Del Nero MP, Dal'Forno T. Synergistic approaches in facial aesthetic rejuvenation: guidelines for combining hyaluronic acid fillers and laser/energy-based technologies. Surg Cosmet Dermatol. 2025;17:e20250385.
This article presents practical guidelines for the synergistic use of HA and laser/energy-based technologies in facial rejuvenation. These recommendations originate from the collaborative interaction of a multidisciplinary group of physicians with experience in dermatology and plastic surgery, and can potentially be extended to treat other areas of the body, including neck and hands. The synergy between HA and lasers/intense pulsed light was recognized, emphasizing patient-tailored treatments and post-treatment care. These recommendations represent valuable guidelines, which can be adapted according to individual patient needs and to the continuous advancement of dermatological technologies.
Keywords: Lasers; Light; Rejuvenation; Hyaluronic Acid; Laser Therapy; Intense Pulsed Light Therapy.
The landscape of facial rejuvenation techniques has transformed substantially over the years, marked by the pursuit of a revitalized and youthful appearance. The realm of modern non-surgical cosmetic procedures now offers a wide range of solutions tailored to enhance the nuances of facial aesthetics while preserving the integrity of natural harmony and expressions.1-4 Hyaluronic acid (HA)-based dermal fillers have emerged as a cornerstone of this paradigm of minimally invasive aesthetic procedures.4,5 These fillers not only restore volume but also lift tissues to reduce the effects of fine lines, folds, hollowing, and wrinkles. Their strategic placement, including regions such as the forehead lines, temple, glabellar lines, lateral canthal lines, nasolabial folds, lips, jawline, marionette lines, chin, and tear troughs, leads to a contoured and rejuvenated aspect.3,5-7 In the context of HA for facial aesthetic rejuvenation, comprehensive characterization of the product holds pivotal clinical significance. Notably, NASHA® crosslinking technology provides HA with prolonged stability and bioavailability, enhancing its clinical utility. In addition, OBTTM technology8,9 finely regulates the physicochemical properties of HA, optimizing its integration within dermal tissues for superior outcomes.10,11 At the same time, lasers and energy-based treatments, exemplified by fractional laser resurfacing and radiofrequency devices, and intense pulsed light (IPL) therapy, have taken center stage. Their capacity to stimulate collagen production, tighten skin, and refine texture and tone has propelled them to the forefront of non-invasive modalities, amenable to individual or combined applications.7,12,13 As technological progress accelerates, the palette of non-surgical interventions for achieving facial rejuvenation is evolving with increasing diversity and efficacy. Yet, within this dynamic backdrop, the pursuit of facial rejuvenation is a nuanced process demanding comprehensive knowledge of individual patient demands, the complexities of aging physiology, facial anatomy, aesthetic principles, product characteristics, optimal technological choices, and the expertise of proficient practitioners3,6,12,14. Considering this multi-dimensional understanding, the aim of the present study is to create practical guidelines for HA treatment with laser/energy-based technologies while meeting evolving clinical needs for optimized outcomes, enhanced safety, and business viability within the particular context of minimally invasive aesthetic interventions of facial and non-facial areas.
A multidisciplinary group of nine medical experts with relevant knowledge and extensive clinical experience in HA treatment combined with laser/energy-based technologies convened in August 2023. The expert group included physicians specializing in dermatology and plastic surgery. The aim of this group was to provide insights and discuss best practices in facial treatments involving these modalities.
Prior to the meeting, the members of the expert group were asked to answer a pre-meeting questionnaire consisting of 17 components relating to various aspects of the treatments:
1. Patient selection criteria
2. Clinical recommendations
3. Contraindications
4. Preoperative preparations
5. Varieties of hyaluronic acid products
6. Techniques of hyaluronic acid injection
7. Number of hyaluronic acid sessions
8. Interval between hyaluronic acid sessions
9. Laser/energy-based technologies used
10. Approaches in laser/energy-based techniques
11. Frequency of laser/energy-based sessions
12. Interval between laser/energy-based sessions
13. Sequencing of technology application
14. Guidelines for intraoperative care
15. Protocols for postoperative care
16. Potential adverse effects
17. Post-treatment follow-up strategies
During the meeting, organized by a neutral and trained medical facilitator (RT), discussions based on the responses to the questionnaire were captured on video. The facilitator steered the conversation, summarized key points, and facilitated clarifications to ensure equitable engagement and contribution from all participants. The discussions focused on comprehensive explanations of different treatment methods, the rationale underlying particular sequences, safety, and synergistic effects of combined treatments for facial aesthetic rejuvenation.
Open debates and dialogues were used to reach an agreement on potentially controversial topics. Participants drew from available evidence, their individual clinical experiences, and their concerns to identify high-relevance principles. These discussions, complemented by a review of current literature, formed the basis of a practical guideline encompassing facial aesthetic rejuvenation treatments.
Panel observations and suggestions from the discussions were assessed, resulting in the development of a manuscript. This manuscript was subsequently subjected to iterative revisions by all the authors, progressively refining its content. The culmination of this collaborative process led to unanimous agreement on the result. The final recommendations presented in this study represent the distilled expertise of the panel, grounded in clinical experience, and substantiated by previously published data pertaining to the intersection of HA and laser/energy-based technologies in the field of facial aesthetic medicine focused on rejuvenation.
The average age of the experts in the group was 48 years old, with an average of 25 years of medical practice, enhanced by advanced training acquired in residencies, master's programs, and doctoral degrees within the specialized domains of general surgery, plastic surgery, dermatology, and internal medicine. After thorough discussions, the following recommendations were formulated based on a combination of scientific evidence and the collective clinical expertise of leading dermatologists, plastic surgeons, and researchers.
The group emphasized the significance of patient selection and assessment, highlighting the importance of considering medical history. Pre-treatment evaluations should encompass detailed skin analysis to determine the most suitable HA formulation and laser/energy-based treatment for each patient. Sequential planning was recommended, with laser/IPL intervention typically preceding HA treatments, in the same session, to optimize skin response. A key aspect of the recommendations was determining the appropriate interval between laser/energy-based treatment and HA administration. The group recognized the potential for synergistic effects through the combination of HA and various laser modalities/IPL therapy within the same appointment to offer improvements in skin rejuvenation and overall aesthetic outcomes without requiring a minimum interval between procedures, unless the laser results in considerable swelling or heightened susceptibility to infection, in which case a 7-day interval between laser treatment and HA administration is advisable. The statements underscored the versatility of laser technologies that can be combined with HA, including fractional lasers, ablative technologies, nonablative lasers, and non-laser technologies, such as IPL therapy, tailored to each patient's needs and manufacturer's specifications. The optimal timing for laser/IPL procedures before administering HA treatments was also debated, culminating in the conclusion that the time between the two interventions does not impact the aesthetic or safety outcomes of the procedure, as laser/IPL application can be immediately followed by the HA injection in the same session, though still accounting for exceptional circumstances related to technologies prone to significant edema or contamination, which can be seen in lasers with ablative potential, such as Er:YAG or CO2. In these cases, it may be necessary to delay HA application by 7 days. Customization emerged as a recurring theme in the recommendations, encouraging practitioners to tailor treatment plans based on individual patient characteristics and desired outcomes, while also accounting for specific laser/energy-based and HA formulations (considering the use of Restylane® NASHA and/or OBT fillers for vertical projection and volume effect, alongside the incorporation of Restylane® SkinboostersTM for skin quality improvement, is advisable). Furthermore, the group emphasized post-treatment care as a pivotal element in minimizing downtime and adverse effects. The recommendations acknowledged that the combination of laser technologies, or IPL therapy, and HA is generally safe when administered by experienced practitioners. However, careful monitoring for potential adverse reactions and thorough patient education were considered essential. The expert group acknowledged the importance of maintaining comprehensive documentation and highlighted the need for further research to fully understand the long-term effects and potential advantages of combining laser/energy-based treatments and HA.
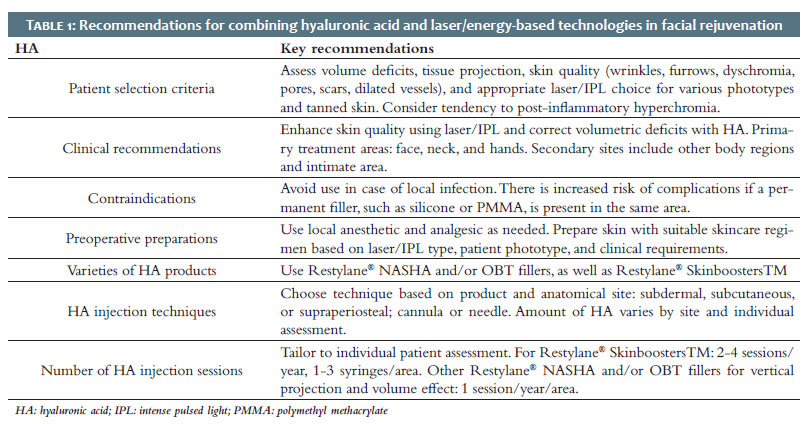
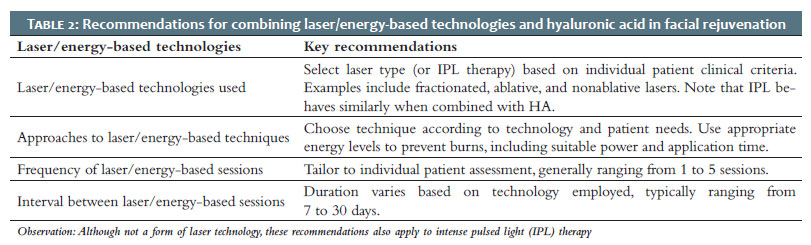
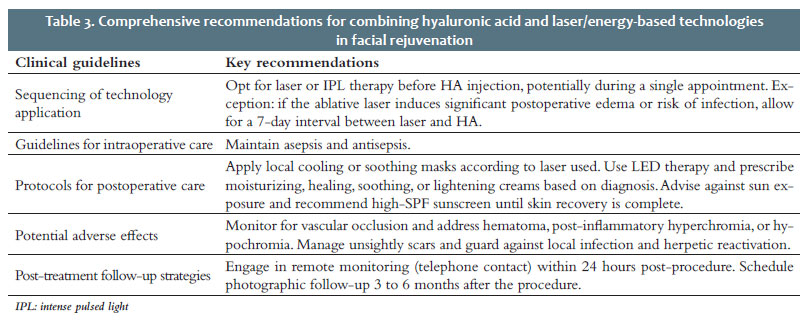
The guidelines present the results for each of the 17 domains discussed by the expert group related to various aspects of the combination of treatments with laser/energy-based technologies and HA. It is important to note that these recommendations serve as guidelines and should be adapted to the specific needs of each patient and the evolving landscape of dermatological technologies. Clinicians are encouraged to keep up-to-date on the latest research and developments in the field to provide the highest standard of care when combining laser/energy-based technologies and HA for facial rejuvenation interventions. Table 1 presents recommendations for the optimal use of HA combined with laser/energy-based technologies for effective facial rejuvenation, Table 2 provides guidelines on the effective use of laser/energy-based technologies combined with HA for enhanced facial rejuvenation outcomes, and Table 3 provides comprehensive recommendations for an integrated approach to optimizing outcomes when combining laser/energy-based technologies and HA for facial rejuvenation.
The use of integrated therapeutic strategies for facial rejuvenation through protocols combining HA injection with laser/energy-based application is known to enhance patient satisfaction and achieve sustained efficacy.15 Nonetheless, the present article seems to represent a pioneering effort to establish practical guidelines for concurrent use of injectable HA treatments and laser/energy-based technologies. While attending to the growing worldwide interest in aesthetic medicine in the area of facial rejuvenation, it also emphasizes improved treatment results and the enhanced sustainability of clinical practice.7,12,16 Following prior findings,17 the expert group suggests that determining the most suitable approach depends on patient preferences, time constraints, anatomical factors, and financial considerations. Nevertheless, the core challenges of determining the extent of the intervention and the sequencing of its components remain a matter of dispute and are scarcely explored in clinical studies. Expert opinions have a key role in steering evidence-based practice and the advancement of aesthetic medicine, particularly within clinical contexts such as the current one which is marked by the limitations of the literature.18,19 In this scenario, practical guidelines developed by unanimous agreement and addressing core clinical topics such as those covered by the present recommendations (patient assessment, emerging technologies, personalized treatment, safety issues, and long-term results, among others) may serve as a valuable resource for both practitioners and patients seeking guidance to fully understand the field, its challenges, and the dynamic landscape of treatments.20,21 From a comprehensive standpoint, the present practical guidelines encompass patient preferences, volume deficits, and skin quality assessment, coupled with the selection of suitable lasers based on phototypes. The clinical emphasis lies in enhancing skin quality via lasers (or IPL therapy) and addressing volume deficits with HA. The integration of HA with lasers/energy-based interventions in the same session involves sequencing technologies before HA, with exceptions for a 7-day interval due to edema or infection risks. Preoperative measures involve skincare preparation and local anesthesia. The use of Restylane® NASHA and/or OBT fillers, alongside the incorporation of Restylane® SkinboostersTM, follows techniques tailored to specific sites. The number of sessions depends on patient assessment, with intervals ranging from 7 to 30 days. Intraoperative care requires asepsis, while postoperative care involves soothing masks, LED therapy, and sun protection. Monitoring adverse effects including vascular occlusion, hematoma, pigmentation, scars, and infection is vital, and management strategies should be guided by the diagnosis. Follow-up requires remote monitoring within 24 hours and photographic documentation 3 to 6 months after the procedure. The recommendations also apply to IPL therapy, which, although not technically a form of laser technology, parallels the findings of Fodor et al. (2004), demonstrating its pivotal role in facial aesthetic rejuvenation. IPL effectively addresses various concerns raised by medical experts, including pigmentation irregularities, vascular anomalies, signs of aging, acne, and unwanted hair growth. This non-invasive modality boasts a favorable safety profile and minimal interruption, making it a versatile and effective solution for comprehensive facial enhancement and rejuvenation.22 Given the predilection of contemporary patients for achieving facial rejuvenation swiftly and cost-effectively, one should consider comprehensive treatments in a single session,17 following the recommendations outlined in the present practical guidelines, which start patients with medical-grade skincare to create more favorable responses to various interventions, including minimal filler augmentation. Following the protocol, laser/IPL procedures before HA injection are endorsed because this sequence facilitates the modulation of skin texture with minimal edema, thereby enabling subsequent volumization with HA.17 The rationale behind this clinical sequencing is the physiological response of the skin induced by laser/IPL treatment. This response encompasses augmented dermal thickness, decreased skin anisotropy, and discernible clinical enhancement characterized by improved texture, diminished pore size, improved wrinkles, and enhanced skin laxity, collectively extending the retention period of HA filler in the treated area.22-26 The proposed guidelines on the volume of HA to be administered and the periodicity of treatment in the context of laser/IPL-filler synergy are grounded on the evidence that diminished dermal thickness attributed to the reorganization of newly formed collagen fibers, a phenomenon known to develop over time, may lead to a discernible aesthetic compromise.15,27 However, it is important to highlight that the persistent impact of laser/IPL treatment, combined with the effects of HA, especially when based on NASHA28 and/or OBT technologies,29 remains effective over up to 12 months.30
The practical guidelines in this article are rooted in the real-world experience of experts, though this approach has limitations due to subjectivity and lack of standardization. However, the elective nature of aesthetic procedures makes the design of comprehensive long-term studies challenging. Thus, the current understanding of emerging facial rejuvenation methods comes mainly from the collective experiences of individual practitioners.17 Therefore, these recommendations would benefit from future controlled clinical trials.19,21
Best practices for synergistic approaches in facial rejuvenation interventions involve the direct sequence of lasers/IPL before HA if administered in the same session. A 7-day interval due to edema or infection risks is advisable when using lasers with ablative potential. Application of Restylane® NASHA and/or OBT fillers combined with technologies follows techniques tailored to specific sites and products while the number of sessions depends on patient assessment. Intraoperative care requires asepsis, while postoperative care involves soothing masks, LED therapy, sun protection, and customized topical treatment. Monitoring and management of adverse effects are key. Follow-up is based on remote monitoring within 24 hours and photographic documentation at 3 to 6 months post-procedure. Furthermore, strategically performing laser/energy-based interventions before HA treatments in the same session to optimize synergistic effects and consequently enhance treatment outcomes during a single session can also be consistent with contemporary patient preferences while enhancing business prospects in the field of facial aesthetics. Based on their expertise, the expert group emphasizes that the combination of Restylane® NASHA and/or OBT fillers with lasers or IPL is an effective and safe strategy for optimizing clinical outcomes in Aesthetic Medicine. l
Adriana Vilarinho
ORCID: 0009-0006-7381-6299
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Alessandra Haddad
ORCID: 0000-0002-5552-7251
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Cintia Cunha
ORCID: 0009-0009-4919-4882
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Fernanda Nunes
ORCID: 0009-0002-2057-7344
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Maria Paula Del Nero
ORCID: 0000-0002-5369-3504
Author's contribution: Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Taciana Dal'Forno
ORCID: 0000-0003-0848-9042
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Sadick NS, Manhas-Bhutani S, Krueger N. A novel approach to structural facial volume replacement. Aesthetic Plast Surg. 2013;37(2):266-76.
2. Hart DR, Fabi SG, White WM, Fitzgerald R, Goldman MP. Current concepts in the use of PLLA: clinical synergy noted with combined use of microfocused ultrasound and poly-l-lactic acid on the face, neck, and décolletage. Plast Reconstr Surg. 2015;136(5 Suppl):180S-7S.
3. Urdiales-Gálvez F, Martín-Sánchez S, Maíz-Jiménez M, Castellano-Miralla A, Lionetti- Leone L. Concomitant use of hyaluronic acid and laser in facial rejuvenation. Aesthetic Plast Surg. 2019;43(4):1061-70. Erratum in: Aesthetic Plast Surg. 2019 Sep 17.
4. Melo F, Carrijo A, Hong K, Trumbic B, Vercesi F, Waldorf HA, et al. Minimally invasive aesthetic treatment of the face and neck using combinations of a PCL-based collagen stimulator, plla/plga suspension sutures, and cross-linked hyaluronic acid. Clin Cosmet Investig Dermatol. 2020;13:333-44.
5. Bertossi D, Giampaoli G, Lucchese A, Manuelli M, Albanese M, Nocini R, et al. The skin rejuvenation associated treatment-fraxel laser, Microbotox, and low G prime hyaluronic acid: preliminary results. Lasers Med Sci. 2019;34(7):1449-55.
6. Langelier N, Beleznay K, Woodward J. Rejuvenation of the upper face and periocular region: combining neuromodulator, facial filler, laser, light, and energy-based therapies for optimal results. Dermatol Surg. 2016;42(Suppl 2):S77-82.
7. Goldman MP, Alster TS, Weiss R. A randomized trial to determine the influence of laser therapy, monopolar radiofrequency treatment, and intense pulsed light therapy administered immediately after hyaluronic acid gel implantation. Dermatol Surg. 2007;33(5):535-42.
8. Rzany B, Cartier H, Kestemont P, Trevidic P, Sattler G, Kerrouche N, et al. Full-face rejuvenation using a range of hyaluronic acid fillers: efficacy, safety, and patient satisfaction over 6 months. Dermatol Surg. 2012;38(7 Pt 2):1153-61.
9. Philipp-Dormston WG, Schuster B, Podda M. Perceived naturalness of facial expression after hyaluronic acid filler injection in nasolabial folds and lower face. J Cosmet Dermatol. 2020;19(7):1600-6.
10. Weiss RA, Moradi A, Bank D, Few J, Joseph J, Dover J, et al. Effectiveness and safety of large gel particle hyaluronic acid with lidocaine for correction of midface volume deficit or contour deficiency. Dermatol Surg. 2016;42(6):699-709. Erratum in: Dermatol Surg. 2016;42(10):1233.
11. Jones DH, Hessler J, Chapas A, Jonas B, Crider J, Chopra R. Microcannula injection of large gel particle hyaluronic acid for cheek augmentation and the correction of age- related midface contour deficiencies. Dermatol Surg. 2020;46(4):465-72.
12. Kim H, Park KY, Choi SY, Koh HJ, Park SY, Park WS, et al. The efficacy, longevity, and safety of combined radiofrequency treatment and hyaluronic acid filler for skin rejuvenation. Ann Dermatol. 2014;26(4):447-56.
13. Akerman L, Mimouni D, Nosrati A, Hilewitz D, Solomon-Cohen E. A Combination of non-ablative laser and hyaluronic acid injectable for postacne scars: a novel treatment protocol. J Clin Aesthet Dermatol. 2022;15(3):53-6.
14. Hsu SH, Chung HJ, Weiss RA. Histologic effects of fractional laser and radiofrequency devices on hyaluronic acid filler. Dermatol Surg. 2019;45(4):552-6.
15. Leheta T, El Garem Y, Hegazy R, Abdel Hay RM, Abdel Halim D. Non-ablative 1540 fractional laser: how far could it help injection lipolysis and dermal fillers in lower-face rejuvenation? A randomized controlled trial. J Cosmet Laser Ther. 2013;15(1):13-20.
16. Kim JE, Hong JY, Lee HJ, Lee SY, Kim HJ. Picosecond-domain fractional laser treatment over hyaluronic acid fillers: in vivo and clinical studies. Lasers Surg Med. 2020;52(10):928-34.
17. Kontis TC, Bunin L, Fitzgerald R. Injectable fillers: panel discussion, controversies, and techniques. Facial Plast Surg Clin North Am. 2018;26(2):225-36.
18. Carruthers J, Burgess C, Day D, Fabi SG, Goldie K, Kerscher M, et al. Consensus recommendations for combined aesthetic interventions in the face using botulinum toxin, fillers, and energy-based devices. Dermatol Surg. 2016;42(5):586-97.
19. Signorini M, Liew S, Sundaram H, De Boulle KL, Goodman GJ, Monheit G, et al. Global aesthetics consensus: avoidance and management of complications from hyaluronic acid fillers-evidence- and opinion-based review and consensus recommendations. Plast Reconstr Surg. 2016;137(6):961e-71e.
20. Philipp-Dormston WG, Bergfeld D, Sommer BM, Sattler G, Cotofana S, Snozzi P, et al. Consensus statement on prevention and management of adverse effects following rejuvenation procedures with hyaluronic acid-based fillers. J Eur Acad Dermatol Venereol. 2017;31(7):1088-95.
21. Urdiales-Gálvez F, Delgado NE, Figueiredo V, Lajo-Plaza JV, Mira M, Ortíz-Martí F, et al. Preventing the complications associated with the use of dermal fillers in facial aesthetic procedures: an expert group consensus report. Aesthetic Plast Surg. 2017;41(3):667-77.
22. Fodor L, Peled IJ, Rissin Y, Ramon Y, Shoshani O, Eldor L, et al. Using intense pulsed light for cosmetic purposes: our experience. Plast Reconstr Surg. 2004;113(6):1789-95.
23. Ross EV, Sajben FP, Hsia J, Barnette D, Miller CH, McKinlay JR. Nonablative skin remodeling: selective dermal heating with a mid-infrared laser and contact cooling combination. Lasers Surg Med. 2000;26(2):186-95.
24. Fournier N, Dahan S, Barneon G, Diridollou S, Lagarde JM, Gall Y, et al. Nonablative remodeling: clinical, histologic, ultrasound imaging, and profilometric evaluation of a 1540 nm Er:glass laser. Dermatol Surg. 2001;27(9):799-806.
25. Fournier N, Dahan S, Barneon G, Rouvrais C, Diridollou S, Lagarde JM, et al. Nonablative remodeling: a 14-month clinical ultrasound imaging and profilometric evaluation of a 1540 nm Er:glass laser. Dermatol Surg. 2002;28(10):926-31.
26. Lupton JR, Williams CM, Alster TS. Nonablative laser skin resurfacing using a 1540 nm erbium glass laser: a clinical and histologic analysis. Dermatol Surg. 2002;28(9):833-5.
27. Imayama S, Braverman IM. A hypothetical explanation for the aging of skin. Chronologic alteration of the three-dimensional arrangement of collagen and elastic fibers in connective tissue. Am J Pathol. 1989;134(5):1019-25.
28. Cartier H, Hedén P, Delmar H, Bergentz P, Skoglund C, Edwartz C, et al. Repeated full- face aesthetic combination treatment with abobotulinumtoxinA, hyaluronic acid filler, and skin-boosting hyaluronic acid after monotherapy with abobotulinumtoxinA or hyaluronic acid filler. Dermatol Surg. 2020;46(4):475-82.
29. Hedén P, Hexsel D, Cartier H, Bergentz P, Delmar H, Camozzato F, et al. Effective and safe repeated full-face treatments with abobotulinumtoxinA, hyaluronic acid filler, and skin boosting hyaluronic acid. J Drugs Dermatol. 2019;18(7):682-9.
30. Carruthers JDA, Glogau RG, Blitzer A; Facial Aesthetics Consensus Group Faculty. Advances in facial rejuvenation: botulinum toxin type A, hyaluronic acid dermal fillers, and combination therapies--consensus recommendations. Plast Reconstr Surg. 2008;121(5 Suppl):5S-30S.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}