


Rebecca Perez de Amorim; Hélio Amante Miot
Funding: None.
Conflict of interest: None.
Submitted on: 09/16/2024
Final decision: 01/28/2025
How to cite this article: Amorim RP, Miot HA. Delayed closure of a scalp surgical wound using the Figueiredo technique: a case report. Surg Cosmet Dermatol. 2025;17:e20250407.
Not all surgical wounds are amenable to primary healing, particularly on the scalp where tissue inelasticity and lesion extent, such as in skin cancers, complicate the procedure. Grafts and flaps increase complexity, recovery time, and surgical costs. The Figueiredo technique reduces costs, protects the wound during its critical phase, maintains wound moisture, and promotes the effective development of granulation tissue. This previously unpublished report demonstrates the use of the technique on the scalp of an elderly patient with systemic scleroderma and a suspected squamous cell carcinoma lesion, showing good progress and satisfactory aesthetic results.
Keywords: Surgical Oncology; Skin Neoplasms; Wound Closure Techniques; Scalp.
The Figueiredo surgical technique, published in 2017, demonstrated the use of a polypropylene prosthesis, obtained from a sterile saline solution bag, to cover traumatic fingertip injuries.1-3 The technique is based on the prior repair of the nail bed and placement of the prosthesis, shaped precisely to the surgical wound area, beneath the nail bed, fixed in place with simple or "U" stitches using nylon thread. The material temporarily replaces the nail, secured to the wound edges without exerting pressure on the nail bed as it heals.1,3 In this way, the wound heals by secondary intention while the prosthesis ensures protection of the treated area, reduces infection from local contamination, accelerates the formation of granulation tissue, and prevents dressings from adhering to the site.1,3 The first report on the use of this technique in dermatology was published in 2023. That article describes its application for lesions located in distal limb extremities, where graft take is more difficult, whether due to the extent of the surgical wound, the presence of shear forces, venous insufficiency, or peripheral edema.2 To date, there have been no reports of the use of the Figueiredo technique on the scalp. The technique may prove highly valuable in dermatological clinical practice, given limited local tissue redundancy and the frequent need for aggressive surgical approaches, depending on the extent of the tumor.
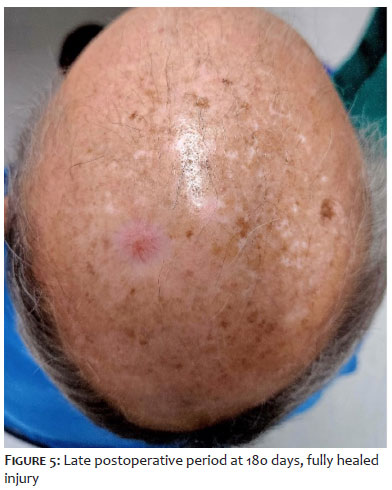
The patient, a 73-year old male with limited systemic scleroderma, reported a painful injury on his scalp for the previous six months. Upon physical examination, the lesion presented as a hyperkeratotic, infiltrated nodule with an erythematous base (Figure 1), 1.5 cm wide in the major axis, located on the left parietal region. The nodule was compatible with suspected squamous cell carcinoma (SCC). An excision with oncologic margins and secondary intention closure using the Figueiredo technique was chosen for the therapeutic surgical approach, given the medium-complexity outpatient setting. Site antisepsis was performed using alcoholic chlorhexidine, and local infiltrative anesthesia was administered with 2% lidocaine and vasoconstrictor. Lesion exeresis included a 4 mm lateral margin reaching the galea at the lower limit (Figure 2). The sterile saline bag was cut and the polypropylene prosthesis placed, maintaining dimensions similar to the surgical defect (Figure 3). To avoid tissue ischemia, the prosthesis was fixed with well-spaced simple stitches using 3-0 nylon. A compressive dressing was applied with gauze, bandage, and Micropore tape. The patient was instructed to remove the secondary dressings 48 hours after the procedure and return in 21 days for prosthesis removal. After 21 days, the patient returned for removal of the prosthesis. The area presented an erythematous, viable granulation tissue, level with the surrounding skin. No debridement was necessary (Figure 4). The patient progressed well, with no complaints, and returned after 45 days with the surgical defect completely healed, reportedly since the 30th day. The histopathological examination reported well-differentiated SCC and exeresis with free margins. The satisfactory aesthetic outcome can be seen in Figure 5, 6 months after the procedure.
The Figueiredo technique is a viable option to manage the healing process in sterile scalp lesions. Considered easy to perform, it does not require a dermatologic surgeon with advanced surgical expertise or a surgical support center at a tertiary hospital. In addition, the technique relies on low-cost, widely available materials, which reduces the burden on the health care system.2-6 Oncologically, it allows for early detection of recurrences and facilitates reintervention, unlike rotation flaps.6-8 It is highly applicable in elderly patients, who have reduced vascular supply, which hinders graft take, as in the case of systemic sclerosis. It also avoids the need to operate on a second surgical site (donor area) in graft procedures, reducing patient discomfort, the likelihood of complications, postoperative recovery time, and the morbidity associated with the procedure. In cases involving flaps, there is also the need to enlarge the surgical area to allow for rotation, increasing both operative time and the amount of anesthesia required. Moreover, many patients have equally photodamaged areas adjacent to the skin tumor to be excised, making them unsuitable for coverage.2,4,5,6 During the healing process, the exudate is replaced by yellowish fibrin. Gradually, this tissue gives way to granulation tissue, which ultimately leads to complete epithelialization of the surgical wound. Because the polypropylene prosthesis is transparent, it allows for reassessment, important in cases involving extensive lesions that require the prosthesis to remain in place for longer than reported in the present case. Healing time depends on wound-related factors, such as infection, and patient-related factors, such as age and skin quality (thickness, vascularization, photodamage degree, etc.).3,4 Some publications have described secondary intention healing in scalp and forehead wounds following Mohs micrographic surgery.6,7 Secondary intention healing relies on two main stages: wound contraction and re-epithelialization. In this case, wound contraction in the area is minimal due to poor tissue elasticity, meaning that healing occurs predominantly through re-epithelialization.7,8 The reepithelialization process begins at the wound edges. Granulation tissue (GT) has to "fill in" the wound before epithelial migration can occur, and GT formation depends on maintaining moisture in the surgical wound (SW). The literature describes cleaning the SW with hydrogen peroxide, using topical antibiotics, daily cleaning, daily application of petrolatum, and four-layer dressings (Vaseline, gauze, cotton, and tape) to prevent secondary infection and allow scar tissue formation. Some authors also suggest using purse-string sutures at the wound edges in order to enhance tissue contraction.7,8 In the circumstances described in this case report, the use of a polypropylene prosthesis offers several advantages. It is durable, remains in place for the period required, protects the operative bed, maintains a moist environment, does not exert compression, and stimulates granulation tissue formation. After the first 48 hours, secondary dressings and ointments can be discontinued while the prosthesis remains in place, and contact with water is permitted. Furthermore, suturing the wound edges enhances the tissue contraction component described above.2,3,4,7,8 Prospective, randomized, controlled trials comparing this method to conventional dressings are needed to assess the potential advantages of the Figueiredo technique in repairing scalp surgical defects undergoing secondary intention healing.
Primary closure is the most common method of skin restoration and should be considered as long as it generates satisfactory aesthetic results and no anatomical distortion. However, there are circumstances when that is not possible. Allowing healing by secondary intention is an alternative to grafts and flaps.6 The Figueiredo technique has been shown to be safe and effective in this case report, there was no local infection associated with prosthesis use, and the patient obtained a satisfactory aesthetic outcome.
Rebecca Perez de Amorim
ORCID: 0000-0002-1170-5685
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Hélio Amante Miot
ORCID: 0000-0002-2596-9294
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Figueiredo LA, Ribeiro RS, Melo ALB, Lima AL, Terra BB, Ventim FC. Polypropylene prosthesis for the treatment of fingertip injuries. Description of surgical technique and results. Rev Bras Ortop. 2017;52(6):685-92.
2. Carrai LHM, Rodrigues EF, Lima TFM, Sasseron MGM, Gomes Neto A. Delayed surgical closure (secondary intention) using the Figueiredo Technique: a case series study. Surg Cosmet Dermatol. 2023;15:e20230212.
3. Muniz AAS, Muniz MT, Figueiredo LA, Figueiredo PH, Oliveira BG. Use of the Figueiredo Technique for the treatment of ring avulsion injury: a case report. BioRes Scientia. 2024;2(2):1-4.
4. Figueiredo LA, Ribeiro RS, Figueiredo PH, Lima ALM, Oliveira FM, Oliveira Júnior DS. Comparison between Atasoy-Kleinert V-Y Advancement Flap and Figueiredo Techniques for the treatment of transverse and dorsal oblique fingertip injuries. Rev Bras Ortop. 2022;59(5): e712–e718.
5. Carvalho RSS, Leitão Júnior PSL, Dias Neto VS, Souza IGL, Rosal LCF, Gomes ACS. Use of polypropylene prosthesis using the Figueiredo Technique for treating thumb degloving in the interior of Minas Gerais – case report. Braz J Health Rev. 2024;7(3):1-11.
6. Sin-Soler M, Yébenes M, Gamissans M, Riera-Martí N, Lara A, Sàbat M. The use of bone wax versus dermal regeneration matrix for the reconstruction of scalp defects. Int J Dermatol. 2024;63(9):1236-41.
7. Becker GD, Adams LA, Levin BC. Secondary intention healing of exposed scalp and forehead bone after Mohs surgery. Otolaryngol Head Neck Surg. 1999;121(6):751-4.
8. Wong N, Zloty D. Secondary intention healing over exposed bone on the scalp, forehead, and temple following Mohs micrographic surgery. J Cutan Med Surg. 2022;26(3):274-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}