


Alessandra Haddad1,2; Juliana Sarubi3; Vania Assaly4
Financial support: Galderma financially supported the writing of this manuscript.
Conflict of interest: Dr. Haddad is a speaker, consultant, advisor, and investigator for Galderma Brazil. Dr. Sarubi is a speaker and consultant for Galderma Brazil. Dr. Assaly has no conflict of interest to declare.
Submitted on: 10/07/2024
Approved on: 15/08/2024
Authors' abbreviations: Haddad A, Sarubi J, Assaly V. How to cite this article: Haddad A, Sarubi J, Assaly V. Systematic Global Body Assessment - a tool to support optimal patient selection for non-surgical treatment of skin laxity. Surg Cosmet Dermatol.2025;17:e20250388.
INTRODUCTION: The search for minimally invasive aesthetic procedures to improve non-facial skin laxity has been increasing annually. The biostimulator poly-L-lactic acid stands out as one of the most versatile products for aesthetic procedures in this field.
OBJECTIVE: To develop a systematic assessment framework tool to guide treatment decision-making for skin laxity in extra-facial areas, since there are no reports regarding how to select the most appropriate patients for non-invasive body shaping with biostimulators to date.
METHODS: The authors developed the tool described herein based on their collective experience with treatment of extra-facial skin laxity with poly-L-lactic acid.
RESULTS: This assessment method collates input from four fundamental factors: somatotype/morphotype, skin quality/severity of laxity, distribution and quantity of adipose tissue, and nutritional and hormonal profile.
CONCLUSIONS: Each aspect of the framework has been developed to optimize decision-making and tailor the clinical experience for each patient, enabling clinicians to select the most favorable candidates for biostimulator use, leading to more predictable and optimized outcomes.
Keywords: Rejuvenation; Classification; Skin Aging.
As skin ages, collagen and elastic fibers degrade, and the consequent loss of structural support and subcutaneous fat results in the development of wrinkles and ptosis, changing the contour and reducing the projection of extra-facial areas.1–3 Skin laxity becomes increasingly prominent in the arms, knees, thighs, buttocks, and abdomen, and is one of the main reasons patients seek aesthetic treatments.4 The search for effective and safe non-surgical aesthetic procedures to improve body appearance and contour has increased significantly in recent years, especially with respect to injectable treatments; an increase of 55% in non-surgical treatments for cellulite and 18% for skin laxity was reported in 2019.5 Poly-l-lactic acid is a biodegradable, biocompatible collagen biostimulator that increases dermal collagen content.6–8 Its facial use has been widely described9,10 and recent reports have also demonstrated its application in extra-facial areas,11 such as the buttocks,12,13 thighs,14 arms,13,15 chest/neck,16,17 and back of the hands.18 However, adequate treatment planning tailored to each individual patient's profile is essential. The objective of this paper is to propose a global and systematic body assessment framework and associated tool to assess which patients with sagging skin in extra-facial areas might be eligible for the use of poly-L-lactic acid. This framework is based on four factors: muscle constitution (somatotype/morphotype), skin laxity and quality, adipose tissue, and hormonal/nutritional profile.
The authors developed the tool described herein through experience sharing. The components of the assessment tool were defined based on the authors' collective experience of treating skin laxity in extra-facial areas with poly-L-lactic acid.
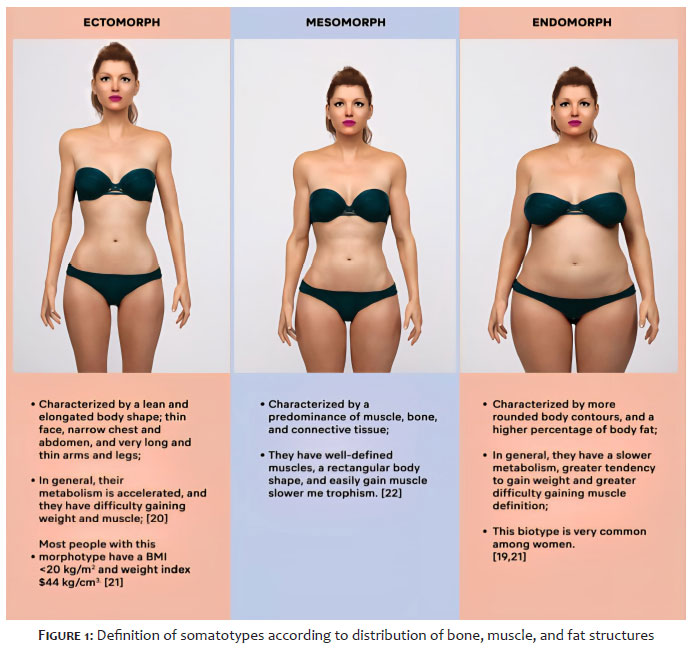
The assessment of somatotypes, also known as morphotypes, classifies the individual's physical structure profile through three primary components: muscle, bone, and body fat. This classification is one of the five clinical items of the global and systematic assessment tool (Table 1). Somatotype influences not only to the concept of weight gain or fat location, but also to how we age, and is determined by racial, genetic and epigenetic factors.19 In clinical practice, this assessment consists of a general inspection of the patient's body in front, lateral and posterior views, seeking to determine the predominant somatotype of the patient (Figure 1).20-22 Based on over 15 years of clinical experience, the authors suggest tailoring poly-L-lactic acid treatment to the patient's predominant somatotype. Overall, the mesomorphic somatotype is usually associated with the best clinical outcomes after poly-L-lactic acid injection, followed by the endomorphic and ectomorphic somatotypes, as summarized in Table 1.
Type I and type III collagen are the most abundant types found in human skin, with type I responsible for skin elasticity and resistance.23 From the age of 30, there is a reduction of around 1% per year in type I collagen, increasing the degree of skin laxity.23–25 Therefore, we selected the degree of laxity and skin quality as the second key consideration when conducting a systematic body assessment. This factor has a direct impact on treatment success: it defines the limits of sagging and the degree of the expected clinical response, as well as helps physicians estimate the number of sessions and vials that will be required. To define eligibility for treatment with poly-L-lactic acid, the authors suggest using a visual analogue scale to grade the severity of body skin laxity (Figure 2). The best and most evident results from poly-L-lactic acid application are obtained in candidates with grade 1 and 2 skin laxity, who usually require only 1 or 2 sessions, while those with grade 3 or 4 will require more treatments (3 to 4 sessions) to achieve satisfactory results.
Adipose tissue contributes substantially to body contouring.26 Although the recommended modality to define the distribution of body fat in gynoid or android patterns is bioimpedance or dual-energy X-ray absorptiometry, this may not be available in all clinics.27 For in-office evaluation, the authors suggest the use of a body fat caliper, which measures skinfold thickness from the superficial subcutaneous cellular tissue. Measurements should be performed on the right side of the body by pinching the skin with the index finger and thumb, while trying to differentiate subcutaneous tissue from muscle tissue. Three measurements should be averaged: the higher the value, the greater the amount of subcutaneous adipose tissue. We suggest a 4-grade classification system according to the amount of adipose tissue present in the treatment area (Table 2).
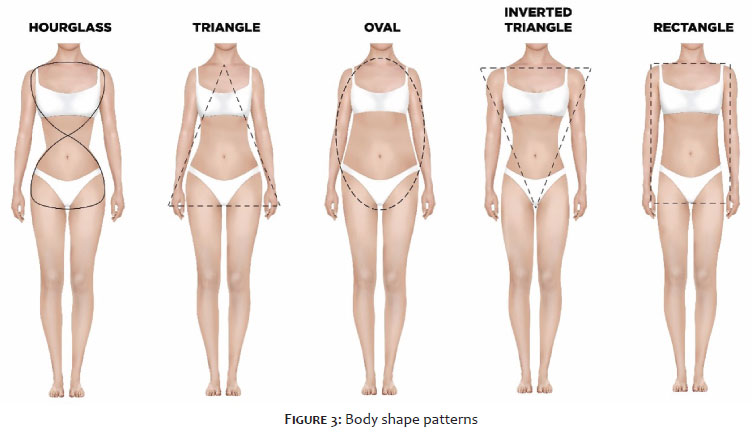
Sex hormones are key determinants of body fat distribution. Estrogen is the main hormone implicated in metabolic regulation, providing protection against the accumulation of adipose tissue28 as well as stimulating collagen production and maintaining skin elasticity.24,25,29,30 Thus, it would be interesting to measure serum levels of sex hormones, transport proteins (sex-hormone binding protein), gonadotropins, and sex steroids; however, these tests are not common in dermatologic clinical practice. We suggest an indirect evaluation by visual determination of body shape (Figure 3).31 Based on the authors' clinical experience, the hourglass and triangle body shapes are most appropriate for treatment with PLLA, as they are likely to denote higher levels of estrogen.28
The body mass index (BMI) is a validated tool widely used to assess for obesity or undernourishment.32 The authors' clinical experience suggests that the ideal BMI for PLLA treatment is in the range of 18.5–24.9 kg/m2; individuals with a BMI <18.4 kg/m2 may not have the expected result due to low levels of body fat and muscle.
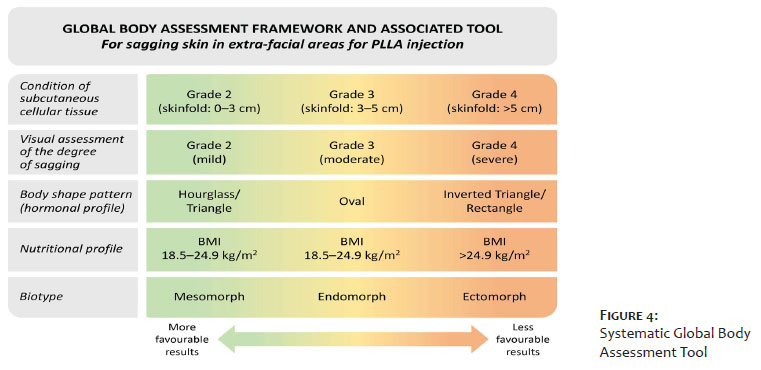
This article proposes a standard framework which has been developed into a tool to evaluate patients who seek treatment for extra-facial skin laxity by applying systematic assessments based on four key factors (Figure 4). Although each of the classic somatotypes has distinctive characteristics, this classification may be considered on a spectrum.21 Most patients have a predominance of two components, which can make it difficult to determine somatotype. Therefore, it is recommended to consider both visual evaluation and anthropometry/adipometry to define somatotype. It is important to emphasize that we are not suggesting that any one somatotype has a greater or lesser response to poly-L-lactic acid treatment, but rather that body constitution may influence the appearance of the skin and body contour, leading to a more or less apparent aesthetic result. Further studies are required to better understand these aspects and their relationship with the results obtained with the use of biostimulators. The objective analysis of skin laxity has been studied previously.33,34 Evaluating the patient's muscle condition is equally important, since muscle mass and tone can interfere with skin laxity in certain body areas; adequate muscle tone enhances aesthetic results, while weak muscles with significant hypotrophy can exacerbate skin laxity.21 The results of treatment will be less visible in these patients, and their expectations should be aligned accordingly. One way to differentiate skin laxity from muscle flaccidity is to evaluate the area using the manual skinfold (pinch) test. In cases of skin laxity, in addition to slow return of the skin, ptosis and formation of spontaneous skinfolds (Grade 3–4) will be observed. Muscle laxity/hypotrophy, in turn, is characterized by a lack of well-defined contours and mobility of the muscle on palpation upon muscle contraction. Regarding adipose tissue, in the authors' experience, grade 1–2 skinfolds (up to a maximum of 4 cm) yield the most favorable results after poly-L-lactic acid application. Nevertheless, studies have shown that gradual weight loss improves the histological structure of the hypodermis, improving skin quality and retractability.26 Thus, patients with Grade 4 adipose tissue or a BMIs in the overweight/obese range should be encouraged to seek professional nutritional guidance and increase the intensity and frequency of physical activity to obtain better results following biostimulator application. Since patients presenting with grade 3/4 fat deposits are less likely to achieve visible results, treatments with other technologies can be considered, either in parallel or instead of poly-L-lactic acid. It is important to note that low food intake and very intense physical activity can also interfere with the outcome of treatment, and more sessions may be required to obtain satisfactory results. Furthermore, post-bariatric surgery patients may have delayed responses to treatment due to changes in adipose tissue structure and skin condition;35 nutritional supplementation is often required in these cases.
Aesthetic procedures, especially the use of poly-L-lactic acid, have been increasingly sought by patients who want to improve skin laxity in non-facial areas of the body. Having a method that enables a systematic and individualized evaluation of patients can further improve their satisfaction with poly-L-lactic acid treatment, align expectations, and optimize outcomes. The authors believe that the use of the proposed tool, based on four key factors, can facilitate the selection of candidates for the application of poly-L-lactic acid in extra-facial areas.
Alessandra Haddad
ORCID: 0000-0002-5552-7251
Approval of the final version of the manuscript, Study design and planning, Preparation and writing of the manuscript, Data collection, analysis, and interpretation, Effective participation in research guidance, Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, Critical literature review, Critical review of the manuscript
Juliana Sarubi 0009-0000-4189-6235
Approval of the final version of the manuscript, Study design and planning, Preparation and writing of the manuscript, Data collection, analysis, and interpretation, Effective participation in research guidance, Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, Critical literature review, Critical review of the manuscript
Vania Assaly
ORCID: 0000-0002-4115-2081
Approval of the final version of the manuscript, Study design and planning, Preparation and writing of the manuscript, Data collection, analysis, and interpretation, Effective participation in research guidance, Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, Critical literature review, Critical review of the manuscript
1. El Khatib HA. Classification of brachial ptosis: strategy for treatment. Plast Reconstr Surg. 2007;119:1337–42.
2. Lin MJ, Dubin DP, Khorasani H. Poly-L-lactic acid for minimally invasive gluteal augmentation. Dermatol Surg. 2020;46:386–94.
3. Hart DR, Fabi SG, White WM, Fitzgerald R, Goldman MP. Current concepts in the use of PLLA: clinical synergy noted with combined use of microfocused ultrasound and poly-l-lactic acid on the face, neck, and décolletage. Plast Reconstr Surg. 2015;136:180S–7S.
4. Kaminer MS, Casabona G, Peeters W, Bartsch R, Butterwick K, Chao YYY, et al. Validated assessment scales for skin laxity on the posterior thighs, buttocks, anterior thighs, and knees in female patients. Dermatol Surg. 2019;45(Suppl 1):S12–S21.
5. American Society of Plastics Surgeons. 2019 Plastic Surgery Statistics Report. 2019.
6. Brown SA, Rohrich RJ, Baumann L, Brandt FS, Fagien S, Glazer S, et al. Subject global evaluation and subject satisfaction using injectable poly-l-lactic acid versus human collagen for the correction of nasolabial fold wrinkles. Plast Reconstr Surg. 2011;127:1684–92.
7. Haddad A, Kadunc BV, Guarnieri C, Noviello JS, Cunha MG, Parada MB. Current concepts in the use of poly-L-lactic acid for facial rejuvenation: literature review and practical aspects. Surg Cosmet Dermatol. 2017;9:60–71.
8. Stein P, Vitavska O, Kind P, Hoppe W, Wieczorek H, Schürer NY. The biological basis for poly-l-lactic acid-induced augmentation. J Dermatol Sci. 2015;78:26– 33.
9. Bohnert K, Dorizas A, Lorenc P, Sadick NS. Randomized, controlled, multicentered, double-blind investigation of injectable poly- l -lactic acid for improving skin quality. Dermatol Surg. 2019;45:718–24.
10. Vleggaar D. Facial volumetric correction with injectable poly-l-lactic acid. Dermatol Surg. 2005;31(11 Pt 2):1511–8.
11. Haddad A, Menezes A, Guarnieri C, Coimbra D, Ribeiro E, Sarubi J, et al. Recommendations on the use of injectable poly-l-lactic acid for skin laxity in off- face areas. J Drugs Dermatol. 2019;18:929–35.
12. Mazzuco R, Sadick NS. The use of poly-l-lactic acid in the gluteal area. Dermatol Surg. 2016;42:441–3.
13. Cunha MG, Daza F, Rezende FC, Machado Filho CDS. Poly-l-lactic acid injections in sagging body skin. Surg Cosmet Dermatol. 2016;8:322–9.
14. Vleggaar D. Soft-tissue augmentation and the role of poly-l-lactic acid. Plast Reconstr Surg. 2006;118:46S-54S.
15. Coimbra DD, Amorim AGF. New techniques poly-l-lactic acid in the rejuvenation of the medial and anterior arms. Surg Cosmet Dermatol. 2012;4:182–5.
16. Melo F, Carrijo A, Hong K, Trumbic B, Vercesi F, Waldorf HA, et al. Minimally invasive aesthetic treatment of the face and neck using combinations of a PCL-based collagen stimulator, PLLA/PLGA suspension sutures, and cross-linked hyaluronic acid. Clin Cosmet Investig Dermatol. 2020;13:333–44.
17. Mazzuco R, Hexsel D. Poly-l-lactic acid for neck and chest rejuvenation. Dermatol Surg. 2009;35:1228–37.
18. Rendon MI, Cardona LM, Pinzon-Plazas M. Treatment of the aged hand with injectable poly-l-lactic acid. J Cosmet Laser Ther. 2010;12:284–7.
19. Carter JEL, Ross WD, Duquet W, Aubry SP. Advances in somatotype methodology and analysis. Am J Physical Anthropol. 1983;26:193–213.
20. Bolonchuk WW, Siders WA, Lykken GI, Lukaski HC. Association of dominant somatotype of men with body structure, function during exercise, and nutritional assessment. Am J Hum Biol. 2000;12:167–80.
21. Olds T, Daniell N, Petkov J, Stewart AD. Somatotyping using 3D anthropometry: a cluster analysis. J Sports Sci. 2013;31:936–44.
22. Ryan-Stewart H, Faulkner J, Jobson S. The influence of somatotype on anaerobic performance. PLoS ONE. 2018;13:1–11.
23. Uitto J. The role of elastin and collagen in cutaneous aging: intrinsic aging versus photoexposure. J Drugs Dermatol. 2008;7:12–6.
24. Chaudhary M, Khan A, Gupta M. Skin ageing: pathophysiology and current market treatment approaches. Curr Aging Sci. 2020;13:22–30.
25. Ganceviciene R, Liakou AI, Theodoridis A, Makrantonaki E, Zouboulis CC. Skin anti-aging strategies. Dermato-Endocrinol. 2012;4:308–19.
26. Silva SL. Anatomic variations of the subcutaneous tissue after ponderal weight lost. Rev Bras Cir Plast. 2010;25:675–8.
27. Kuriyan R. Body composition techniques. Indian J Med Res. 2018;148(5):648–58.
28. Rettberg JR, Yao J, Brinton RD. Estrogen: a master regulator of bioenergetic systems in the brain and body. Front Neuroendocrinol. 2014;35:8–30.
29. Dao H, Kazin RA. Gender differences in skin: a review of the literature. Gend Med. 2007;4:308–28.
30. Rahrovan S, Fanian F, Mehryan P, Humbert P, Firooz A. Male versus female skin: what dermatologists and cosmeticians should know. Int J Womens Dermatol. 2018;4:122–30.
31. Mcainch AJ, Scott D, Armamento-Villareal R, Aguirre LE, Qualls C, Villareal DT, et al. Fat mass follows a u-shaped distribution based on estradiol levels in postmenopausal women. Front Endocrinol. 2018;9:315.
32. World Health Organization. Body mass index (BMI). 2023.
33. Alam M, Pongprutthipan M, Nanda S, Kim NA, Swary JH, Roongpisuthipong W, et al. Quantitative evaluation of skin shrinkage associated with non-invasive skin tightening: a simple method for reproducible linear measurement using microtattoos. Lasers Med Sci. 2019;34:703–9.
34. Hexsel D, Dal'Forno Dini T, Hexsel C. Skin distension test: a new simple tool to evaluate skin laxity. Dermatol Surg. 2021;47(7):1026–7.
35. Light D, Arvanitis GM, Abramson D, Glasberg SB. Effect of weight loss after bariatric surgery on skin and the extracellular matrix. Plast Reconstr Surg. 2010;125(1):343–51.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}