


Taciana Dal´Forno; Martina Souilljee Birck
Funding: None.
Conflicts of interest: None.
Submitted on: 04/16/2024
Approved on: 08/01/2024
How to cite this article: Dal'Forno, Birck MS. Scrotodynia successfully treated with botulinum toxin. Surg Cosmet Dermatol. 2025;17:e20250376.
Scrotodynia, or genital dysesthesia, is characterized by chronic scrotal pain lasting at least 3 months, with no identifiable etiology despite thorough investigation. Although it is considered a relatively common condition, the lack of effective therapeutic options significantly impacts the quality of life of affected patients. We report a successful and sustained treatment for scrotodynia with botulinum toxin in a 69-year-old patient who had not responded to appropriately dosed oral medications for chronic pain.
Keywords: Male Urogenital Diseases; Botulinum Toxins; Pain, Intractable.
Chronic scrotal pain, termed scrotodynia or genital dysesthesia, if no etiology is defined after careful investigation, is a relatively common condition. Although still poorly understood, it has a significant impact on patients' quality of life and causes frustration given the limitations of the therapeutic options currently available. This condition is characterized by unilateral or bilateral, constant or intermittent scrotal pain or discomfort lasting more than 3 months.1 This report aims to describe the therapeutic success in managing scrotodynia in a 69-year-old patient using injectable botulinum toxin.
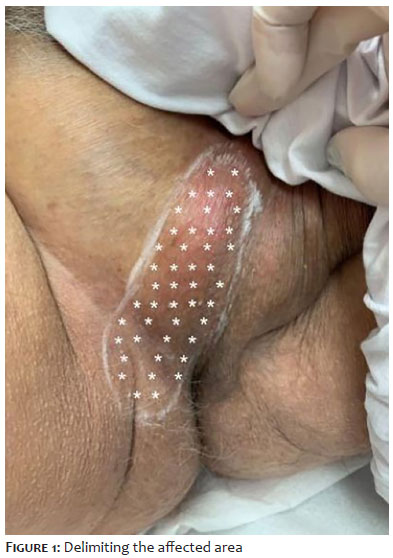
A 69-year-old male patient presented with discomfort, stinging, and superficial itching in the scrotum and right inguinal region, which had been going on for approximately 6 years. He had no history of genital herpes or other conditions in the region. No specific etiology was identified after extensive investigation by a urologist. The patient showed no improvement following the use of oral medications for chronic pain, including anticonvulsants, prescribed by a clinical physcian. On physical examination, no skin lesions were observed in the affected area, nor any other alterations, except for the presence of 2 acrochordons. In view of the refractory nature of the conventional medication, it was decided to treat the patient with botulinum toxin (Dysport®), at a total dose of 90 units (U). The application was made intradermally, at a rate of 2 U per point, distributed over 45 points, with a spacing of 0.5 cm between them, covering the entire symptomatic area, previously identified with the help of the patient, who indicated the areas of greatest discomfort, including the scrotum and part of the right inguinal region (Figure 1). The patient reported a significant improvement in symptoms 2 weeks after the procedure and expressed satisfaction with the therapeutic approach, no longer requiring the use of oral medication for pain relief. In addition, no adverse effects related to the application of the toxin were observed. The patient maintained satisfactory symptom control for a period of 10 months, using this intervention exclusively, with no need for complementary therapies during follow-up.
The management of scrotodynia represents a clinical challenge because, in addition to the need to exclude acute and chronic causes associated with scrotal pain syndrome, there is no consensus to date on the most effective therapeutic approach.2 The available literature mainly addresses the use of drugs used to control neuropathic pain, a pathophysiological mechanism potentially involved in genital dysesthesia, including antibiotics, tricyclic antidepressants, and anticonvulsants.3
As second-line options, surgical procedures such as epididymectomy, vasovasostomy, vasectomy, orchiectomy, and testicular denervation have been described, although they are associated with significant risks, such as infertility, and often unpredictable results.2 Given these limitations, minimally invasive measures with a better long-term safety profile have been progressively explored. There are reports, although based on small series of cases, on the use of radiofrequency spermatic cord ablation, with symptomatic relief for periods ranging from 6 to 9 months.1
On the other hand, botulinum toxin has been consolidated as a therapeutic drug in the management of various pain syndromes of neuropathic origin, including pain located in the genital region, such as anal fissures, vulvodynia, and vaginismus. In these conditions, significant clinical improvement is observed a few days after application, with a sustained response for periods ranging from 12 to 24 weeks.3 The literature also describes the use of botulinum toxin at a dose of 100 U for the management of genital dysesthesia.4
In this context, we decided to apply 90 U of botulinum toxin in this case, distributed in the delimited area of dysesthesia, as indicated by the patient. Significant clinical improvement was observed within 2 weeks of the procedure, and the response was maintained up to the time of writing this report. The absence of adverse effects, coupled with the possibility of discontinuing the oral medications previously used, reinforces the beneficial potential of this intervention in the management of scrotodynia.
This report shows that injectable botulinum toxin can be an effective and safe therapeutic option in the management of scrotodynia, especially in cases refractory to conventional drug therapies. The patient's active participation in delimiting the affected area, as well as the adequate definition of the dose, seem to be determining factors in the success of the treatment. Despite the favorable results observed, studies with a larger number of patients and long-term follow-up are needed to validate the efficacy, safety, and lasting effects of botulinum toxin in the treatment of scrotodynia. l
Taciana Dal'Forno
ORCID: 0000-0003-0848-9042
Statistical analysis, approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, data collection, analysis, and interpretation, effective participation in research guidance, intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, critical literature review, critical review of the manuscript.
Martina Souilljee Birck
ORCID: 0000-0001-9281-7744
Author's contribution: Study design and planning, preparation and writing of the manuscript, data collection, analysis, and interpretation, intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, critical literature review.
1. Wu C, Jarvi K. Chronic scrotal pain. Curr Urol Rep. 2018;19(8):59.
2. Gordhan CG, Sadeghi-Nejad H. Scrotal pain: evaluation and management. Korean J Urol. 2015;56(1):3-11.
3. Raef HS, Elmariah SB. Treatment of male genital dysesthesia with botulinum toxin. JAAD Case Rep. 2021;10:60-2.
4. Khambati A, Lau S, Gordon A, Jarvi KA. Onabotulinum toxin A (Botox) nerve blocks provide durable pain relief for men with chronic scrotal pain: a pilot open-label trial. J Sex Med. 2014;11(12):3072-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}