


Marisa Gonzaga da Cunha; Ana Lúcia Gonzaga Cunha; Daphine Tironi Giglio; Débora Terra Cardial; Gabrielle Ellert de Almeida
Financial support: None.
Conflict of interest: None.
Submitted on: 10/16/2023
Approved on: 10/03/2024
How to cite this article: Cunha MG, Cunha ALG, Giglio DT, Cardial DT, Almeida GE. Sodium deoxycholate - mechanism of action, application technique, indications, and adverse effects. Surg Cosmet Dermatol. 2025;17:e20250307.
Techniques for removing adipose tissue are always of great interest, and among many described, the applications of sodium deoxycholate (DS) or deoxycholic acid, known as intralipotherapy, have stood out in recent years, following approval by the FDA for the treatment. of submental fat, due to the ease of application and short downtime. The objective of this study was to elucidate, through the available literature, the most frequently asked questions in this regard, and demonstrate that it is an effective and safe alternative for the treatment of localized fat.
Keywords: Atrophy; Adipose Tissue; Fat Body.
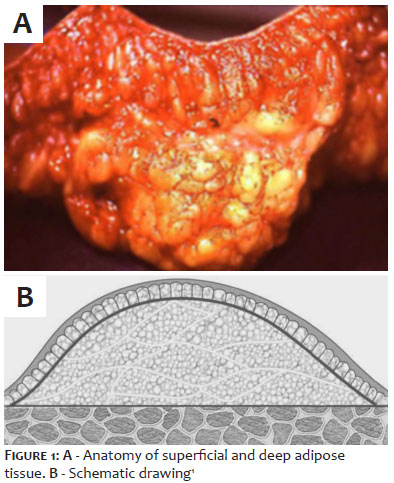
Adipose tissue has been a subject of growing interest, as new surgical and nonsurgical removal techniques have been proposed. Anatomical and histological research has enabled more rational and effective procedures to be developed. In addition, adipose tissue has become of major interest in the study of the anatomy of aging and dermatology.1 Anatomically, adipose tissue is divided into hypodermis or areolar/superficial adipose tissue (SAT) and lamellar/deep adipose tissue (DAT). In some areas of the body, both layers are present, while in others, it is only the hypodermis that covers the entire integument.1 Subcutaneous adipose tissue or DAT originates embryologically in the mesoderm and functions to store energy, protect against mechanical shocks, and allow mobility over deeper structures. It also has an important cosmetic effect, shaping the body contour and presenting significant variation in fat content and thickness among individuals. The location of DAT is determined mainly by genetics and hormones, being responsible for sexual dimorphism.2 It is present only in certain areas of the body, mainly in the abdomen, flanks, trochanteric region, inner upper thighs, knees, and back of the arms. Proportionally, during weight loss, it reduces less in thickness than SAT, since its adipocytes are predominantly α2 adrenergic receptors (antilipolytic).3 The areas of lipodystrophy are organized as follows from the surface: skin (epidermis and dermis), hypodermis or SAT, a horizontal fibrous layer of connective tissue (membranous layer or superficial fascia), DAT, which covers the deep fascia and muscles.3,4
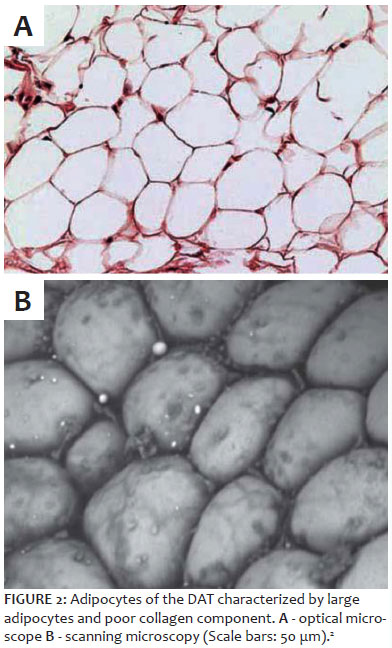
DAT differs from the hypodermis in appearance: it has larger, flatter, and less defined adipose tissue lobules, with less evident fibrous septa, generally oriented obliquely and connected to the membranous layer of the deep fascia of the muscles (Figures 1A and 1B). Sbarbati et al. describe this layer from the peri-adipocyte collagen network as incomplete, extremely fragile, and finely adherent, with few vascular components, which apparently characterizes it as an area of high lipid deposition (Figures 2A and 2B).4 The low structural stability, limited elasticity properties to stretching, and low resistance to compression explain the sliding of this subcutaneous tissue over the deep fascia.3
There are few nonsurgical therapeutic options for the treatment of DAT, and among them, the application of sodium deoxycholate (SD) or deoxycholic acid has stood out in recent years, after FDA approval for the treatment of submental adipose tissue, due to its ease of application and short downtime. Its application is indicated for small areas of lipodystrophy, often not amenable to other forms of treatment,5 through a technique called intralipotherapy. SD is a synthetic bile salt with a chemical structure identical to the endogenous one, but it does not contain substances of human or animal origin. It causes dose-dependent lysis of mature adipocytes with necrosis, rupture, and dissolution of the adipose architecture and inflammatory response, preserving adjacent structures.5-8 The destruction of fat cells causes a local tissue inflammatory response involving fibroblast infiltration, localized neocollagenesis, and macrophage recruitment to eliminate lipids and cellular debris.9 This article aims to elucidate the mechanism of action of DS, its best indications for the treatment of facial and body adipose tissue, application technique, and adverse effects.
The combination of sodium deoxycholate and phosphatidylcholine is marketed under the trade name Lipostabil®. It is produced and distributed in Europe by Aventis Pharma, and its intravenous application is indicated for the treatment of fat embolism and dyslipidemia.5 Since 2001, it has been used in Brazil for the treatment of lipodystrophy, but the manufacturer never requested its registration with the Brazilian National Health Surveillance Agency (Agência Nacional de Vigilância Sanitária [ANVISA]). In April 2011, the sale and distribution of Lipostabil® and its active ingredient phosphatidylcholine were banned in Brazil.10 However, ANVISA still allowed the active ingredient sodium deoxycholate to be compounded. In 2004 and 2005, the first studies showed that the lipolytic activity of the combination was due to sodium deoxycholate and not phosphatidylcholine, which only acted as a diffuser.12 In 2015, ATX-101 (Kythera Biopharmaceuticals, a subsidiary of Allergan, West Lake Village, California) was approved by the FDA at a concentration of 10 mg/mL for subcutaneous application in the treatment of submental adipose tissue and has been marketed under the name Kybella in the US and Belkyra in Canada. In Brazil, as of 2018, DS was approved for use to reduce adipose tissue—the opinion concluded that studies showed the safety and effectiveness of the drug in eliminating submental adipose tissue and that, given its legal registration, it is a product approved for the intended purposes (ANVISA/MS—1.1047.0185). However, the injectable use of phosphatidylcholine is prohibited in Brazil (ANVISA Resolution No. 30 of January 8, 2003). It is currently approved in the United States and Canada and, according to the product label, only for the treatment of submental adipose tissue. In Brazil, there are no specifications regarding the areas indicated for its use, therefore its use on the body is not considered off-label.
After questions regarding the association of phosphatidylcholine and DS, studies initiated by Rotunda in 2004 revealed that this was the truly active ingredient, acting in a dose-dependent manner as a biological detergent, solubilizing cellular phospholipid bilayers and leading to adipocyte lysis.10 SD disrupts the integrity of membranes by introducing its polar hydroxyl groups into the hydrophobic core of the bilayer, solubilizing the membrane. The cell collapses into micelles of phospholipids and detergent molecules.11 Experiments using cell culture, metabolic assays, and histological evaluations have independently verified, by testing isolated DS, that it was capable of inducing cell lysis and resulting necrosis, with most cells destroyed within 15 minutes of incubation with the solution in vitro. These experiments also revealed that mature adipocytes were more resistant to detergent-induced cell lysis in vitro, raising the issue of safety in the event of accidental injections outside the adipose tissue compartments.12 Subsequent studies with histological examinations revealed that DS does not affect the muscle layer, dermis, and epidermis, despite intense necrosis and fibrosis of the subcutaneous cellular tissue.13 DS is insoluble in aqueous solutions, and serial histological studies have demonstrated marked differences in patients treated with mixtures when compared to isolated DS. After injection, specimens have shown small areas of adipose tissue with scattered necrotic and fibrotic effects, with minimal changes after injection of the mixture, as opposed to focal areas of adipose tissue necrosis when DS is used alone.12 Areas injected 1 week before microscopic examination showed small areas of adipose tissue necrosis in the tissue exposed to the solution, while intense inflammation and fibrosis were observed in areas treated with DS alone. After 2 weeks, histological examinations showed large areas of necrosis in the buccal pouch, with inflammation, neovascularization, adipose lysis, and macrophage infiltration with DS alone and more organized adipose necrosis with the solution. After 1 month, a fibrotic appearance was seen in the subcutaneous tissue treated with DS alone, while the areas treated with the combined solution showed a fractional response, with small areas of adipose necrosis separated by islands of normal-appearing adipose tissue. The treatment areas exhibited sterile cellulitis with neutrophil-rich infiltrate in the deep reticular dermis in all patients.12,13 In summary, when injected into subcutaneous adipose tissue, DS causes adipocytolysis and stimulates the local tissue response with macrophage infiltration that removes cellular debris and released lipids, fibroblast recruitment, and neocollagenesis. The process begins 15-20 minutes after application.5,15 Studies have shown that DS alone enters the circulation within a few days after injection, binds to albumin present in plasma, and undergoes fecal elimination in a manner similar to endogenous bile acids.5,13,14
The application of DS, preferably in isolation, is indicated for small and medium-sized areas of lipodystrophy in patients with low BMI (20-25). On the face, the most suitable areas are submental adipose tissue and the jaw. On the body, the most suitable areas are located on the abdomen, waist, flanks, upper outer thighs, upper back of the thighs, below the infragluteal fold, inner knees and arms, back, and anterior and posterior axillary folds.15 These areas have little therapeutic response to other forms of treatment, including liposuction, which can leave residual sagging.15 In addition to the treatment of lipodystrophy itself, other indications in the literature are for liposuction touch-ups and for the treatment of paradoxical adipose tissue after cryolipolysis.16
Infection at the application site, pregnancy, and breastfeeding. No studies in patients under 18 or over 65 have confirmed its safety.
In Brazil, DS must be compounded upon individualized prescription with the patient's name. The most commonly used concentrations are 1% for the face and 2.44% for the body. Studies have not shown any advantages in the 6% concentration.16,17,20 Combinations with other active ingredients do not increase the performance of DS and, furthermore, there is no standardization for these preparations. It should be noted that the numerous products distributed in Brazil, containing phosphatidylcholine or other active ingredients, are registered for cosmetic use only and are not indicated for injectable use.
Before each application, photos taken from the front, at a 45º angle and at a 90º angle are recommended to evaluate the treatment results. To each 6 mL vial of 2.44% DS for body use, 1.0 mL of lidocaine can be added to reduce discomfort during application. The injection technique is important to avoid technical adverse events, and it should be noted that this is intralipotherapy and not mesotherapy (or intradermotherapy). The main difference is that in mesotherapy, the application is performed in the dermis, and in intralipotherapy, in the localized adipose tissue, which is a deeper application.16,17,19,20 The application can be performed with 30G 13 mm needles for the body and 9 mm needles for the face. Small amounts should be injected at each application point: 0.1 mL or less per 1 cm on the face and up to 0.2 mL per 2 cm on the body should be observed. Studies have shown that doses greater than 4 mg/cm2 did not produce greater efficacy and resulted in more frequent and severe adverse effects.18,19 The maximum amount recommended by Amore et al. is 5 vials with 10 mL of 1.22% solution.18 The depth should be 9 to 13 mm in most areas of the body and around 6 mm on the face and neck, with the needle always positioned vertically to the skin. It is mandatory to wait a few seconds before removing the needle to avoid superficialization of the product. The application is virtually painless, but erythema and local burning begin a few minutes later. Massaging the area helps to relieve the symptoms. After application, the use of a compression bandage for a few days can reduce edema and local soreness. The use of oral analgesics is generally unnecessary. The application can be done at 4-week intervals, and studies have shown that up to 6 sessions are necessary for complete improvement of adiposity, although most patients improved with 4 sessions or less.18
Studies have not shown any systemic effects with the recommended doses of DS used alone.12 Edema, erythema, hardening, and local soreness are expected adverse effects caused by panniculitis resulting from the application of DS. These effects appear shortly after application and are self-limiting, requiring no treatment. Edema lasts 9-10 days and hardening lasts 17-25 days and tends to be proportional to the degree of lipolysis. In combinations with DS, nausea, dizziness, and malaise were observed shortly after injection.12 True complications include dysphagia, temporary asymmetry of the smile due to paresis of the marginal nerve of the mandible, focal necrosis, and irregularities due to superficial injections, nodules due to increased focal necrosis, and transient alopecia of the treated area, probably due to local inflammation. Comparative studies with DS alone and in combination showed no differences in adverse effects and complications. Septal and lobular panniculitis were noted with thickening of the fibrous septa, adipose necrosis, and formation of persistent granulomas when doses greater than 0.2 mL were used at each site and when DS alone was applied in high concentrations.13 Treatment with DS had no effect on serum glucose, lipid, and plasma inflammation marker levels when used within the recommended doses.21
DS has proven to be an effective and safe alternative for the treatment of lipodystrophy (localized adipose tissue) when applied correctly using the intralipotherapy technique (injection into the subcutaneous adipose tissue), with few and self-limiting adverse effects.21,22 Combination with other active ingredients has not shown improved performance, and combination with phosphatidylcholine is prohibited for injectable use in Brazil.
Marisa Gonzaga da Cunha
ORCID: 0000-0002-4186-0643
Statistical analysis, approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, data collection, analysis, and interpretation, effective participation in research guidance, intellectual participation in the propaedeutic and/or therapeutic conduct of the cases studied, critical literature review, critical review of the manuscript.
Ana Lúcia Gonzaga Cunha
ORCID: 0000-0001-8431-3386
Statistical analysis, approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, data collection, analysis, and interpretation, effective participation in research guidance, intellectual participation in the propaedeutic and/or therapeutic conduct of the cases studied, critical literature review, critical review of the manuscript.
Daphine Tironi Giglio 0009-0005-9775-614X
Approval of the final version of the manuscript, effective participation in research guidance.
Débora Terra Cardial
ORCID: 0000-0003-2482-4234
Preparation and writing of the manuscript, data collection, analysis, and interpretation, intellectual participation in the propaedeutic and/or therapeutic conduct of the cases studied, critical literature review, critical review of the manuscript.
Gabrielle Ellert de Almeida
ORCID: 0000-0002-4707-1100
Approval of the final version of the manuscript, preparation and writing of the manuscript, data collection, analysis, and interpretation, intellectual participation in the propaedeutic and/or therapeutic conduct of the cases studied, critical literature review, critical review of the manuscript.
1. Illouz,YG. Complications of liposuction. Clin Plastic Surg 2006;33(1):129–63.
2. Cunha MG, Cunha ALG, Machado CA. Hypodermis and subcutaneous adipose tissue two. Diferente structures. Surg Cosmet Dermatol 2014;6(4):355-9.
3. Paschoal LHC, Cunha MG, Ciporkin H. Fisiopatologia e atualização terapêutica da lipodistrofia ginóide - celulite. 2nd rev. ed. Rio de Janeiro: Di Livros; 2012.
4. Sbarbati A, Accorsi D, Marchetti L, Orsini G, Rigotti G, Panettiere P. Subcutaneous adipose tissue classification. Eur J Histochem.2010;54(4):226-30.
5. Kamalpour S, Leblanc Jr K. Injection adipolysis: mechanisms, agents, and future directions. J Clin Aesthet Dermatol. 2016;9(12):44–50.
6. Rotunda AM, Suzuki H, Moy RL, Kolodney MS. Detergent effects of sodium deoxycholate are a major feature of an injectable phosphatidylcholine formulation used for localized fat dissolution. Dermatol Surg. 2004;30(7):1001-8.
7. Rose PT, Morgan M. Histological changes associated with mesotherapy for fat dissolution. J Cosmet Laser Ther. 2005;7(1):17-9.
8. Rotunda AM. Injectable treatments for adipose tissue: terminology, mechanism, and tissue interaction. Lasers Surg Med. 2009;41(10):714–20.
9. Duncan D, Rubin JP, Golitz L, Badylak S, Kesel L, Freund J, et al. Refinement of technique in injection lipolysis based on scientific studies and clinical evaluation. Clin Plast Surg. 2009;36(2):195–209.
10. Ministério da Justiça e Segurança Pública (BR). Relatório 2022 – produtos farmacêuticos. 2023.
11. Lichtenberg D, Ahyayauch H, Goñi Fm. The mechanism of detergent solubilization of lipid bilayers. Biophys J. 2013;105(2):289–99.
12. Gupta A, Lobocki C, Singh S, Robertson M, Akadiri OA, Malhotra G, et al. Actions and comparative efficacy of phosphatidylcholine formulation and isolated sodium deoxycholate for different cell types. Aesthetic Plast Surg. 2009;33(3):346–52.
13. Thuangtong R, Bentow JJ, Knopp K, Mahmood NA, David NE, Kolodney MS. Tissue-selective effects of injected deoxycholate. Dermatol Surg. 2010;36(6):899–908.
14. Saluja SS, Avram MM. Overview of non-invasive treatments for submental fat reduction. The PMFA J. 2018;5(6).
15. Sykes JM, Allak A, Klink B. Future applications of Deoxycholic acid in body contouring. J Drugs Dermatol. 2017;16(1):43-6.
16. Herreros FOC, Velho PENF, Moraes AM. Mesoterapia: uma revisão biliográfica. An Bras Dermatol. 2011;86(1):96-101.
17. Amore R, Pinto H, Gritzalas K, Hernández C, Skwara-Guzikowska K, Amuso D, et al. Intralipotherapy, the state of the art. Plast Reconstr Surg Glob Open. 2016;4(10):e1085
18. Georgesen C, Lipner SR. The development, evidence, and current use of ATX-101 for the treatment of submental fat. J Cosmet Dermatol. 2017;16(2):174-9.
19. Pinto H, Hernandez C, Turra C, Manzano M, Salvador L, Tejero P. Evaluation of a new adipocytolytic solution: adverse effects and their relationship with the number of vials injected. J Drugs Dermatol. 2014;13(12):1451–5.
20. Amore R, Amuso D, Leonardi V, Leva F, Sibaud AC, Guida A, et al. Evaluation of safe and effectiveness of an injectable solution acid deoxycholic based for reduction of localized adiposities. Plast Reconstr Surg Glob Open. 2018;6(6):e1794.
21. Reeds DN, Mohammed BS, Klein S, Boswell CB, Young VL. Metabolic and structural effects of phosphatidylcholine and deoxycholate injections on subcutaneous fat: a randomized, controlled trial. Aesthet Surg J. 2013;33(3):400-8.
22. Duncan DI, Palmer M. Fat reduction using phosphatidylcholine/sodium deoxycholate injections: standard of practice. Aesth Plast Surg. 2008;32(6):858-72.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}