


Flavia Alvim Sant'anna Addor1; Ana Claudia Cavalcante Esposito2; Emerson de Andrade Lima3; Lucas Portilho4; Eliana Mika Yamaguchi5; Sylvia Ypiranga5
Financing: L'Oréal Brazil provided funds for the in-person author meetings.
Conflicts of interest: Flávia Addor works as a speaker, researcher, and consultant for L'Oréal Brazil, Galderma, Eucerin and Kenvue. Ana Cláudia Cavalcante Espósito has performed scientific activities with L'Oréal Brazil. Sylvia Ypiranga has worked as a speaker for Galderma.
Submitted on: 04/16/2024
Final decision: 07/25/2024
How to cite this article: Addor FAS, Esposito ACC, Lima EA, Portilho L,Yamaguchi EM, Ypiranga S. Multidisciplinary consensus on the benefits of topical vitamin C. Surg Cosmet Dermatol. 2025;17:e20250366.
Vitamin C, or L-ascorbic acid, is the most abundant antioxidant in human skin and its topical replacement has proven relevant, since this reservoir is consumed by external aggression, and it is used in the prevention and treatment of skin aging. This review was based on bibliographic research in the PubMed and LILACS databases and two consensus meetings between the authors to analyze the evidence for its topical use. The highest level of evidence of skin activity has been found in the pure and stabilized form of ascorbic acid. Derivatives, carriers, and nanoformulas are being developed, however further clinical and comparative studies are needed.
Keywords: Ascorbic Acid; Antioxidants; Skin Aging; Hyperpigmentation; Cosmeceuticals.
Given that the skin is the organ most exposed to external factors that accelerate the skin aging process, such as ultraviolet radiation, smoking, pollution, poor diet and stress,1 the skin care market is the leading segment of the cosmetics industry, accounting for approximately 36% of the global market. Vitamin C, or L-ascorbic acid (AA), is an important ingredient in dermocosmetic products due to its multifunctionality.2,3 AA is an essential nutrient obtained exclusively from exogenous sources, and is the most abundant antioxidant in human skin,4 whose biochemical activity is restricted to its levorotatory (L) form, since the dextrorotatory form has no significant biological activity.5 The first publications on the topical use of AA date back to the early 1960s, and this form is essential for increasing cutaneous bioavailability, given that the levels achievable through topical application are 20 to 40 times higher than with oral AA supplementation.6 Moreover, when the skin becomes saturated with AA through topical application, a reservoir effect occurs in which AA tends to stabilize and remain available in the skin for 3 to 4 days.4,6,7 This storage provides prolonged protection against environmental damage, such as UV radiation, pollution, and smoking, which induces oxidative stress in the skin.1,7–9 Although the effectiveness of topical AA has been demonstrated,8,10 developing formulations for topical use is still challenging due to the molecule's instability, which has stimulated research into AA derivatives and active release technologies. However, although molecular stability has been improved through these innovations, comparative studies on the clinical response and therapeutic action of these new derivatives in comparison with AA are still lacking in the literature. This review will explore the types of AA available for topical use, their proven benefits, and their applicability for clinical dermatology.
This article is the result of two consensus meetings between the authors, dermatologists, and pharmacists held in November 2022. Prior to the meetings, a comprehensive bibliographic search was performed in the PubMed and LILACS databases, using a combination of the keywords "vitamin C" or "ascorbic acid" and "skin" and "topical", to find relevant articles involving three themes: (1) the efficacy, function, and mechanism of action of AA in its different formats; (2) advances in formulation regarding the efficacy, stability, skin penetration, and bioavailability of AA and its derivatives; and (3) the application and clinical efficacy of topical AA in different forms. A third of the selected articles involved authors affiliated with Brazilian institutions, indicating the relevance of the topic in Brazil. In the meetings, the topics were discussed based on the published literature, and while preparing the review's manuscript, other published articles and relevant technical documentation were included by mutual agreement among the authors.
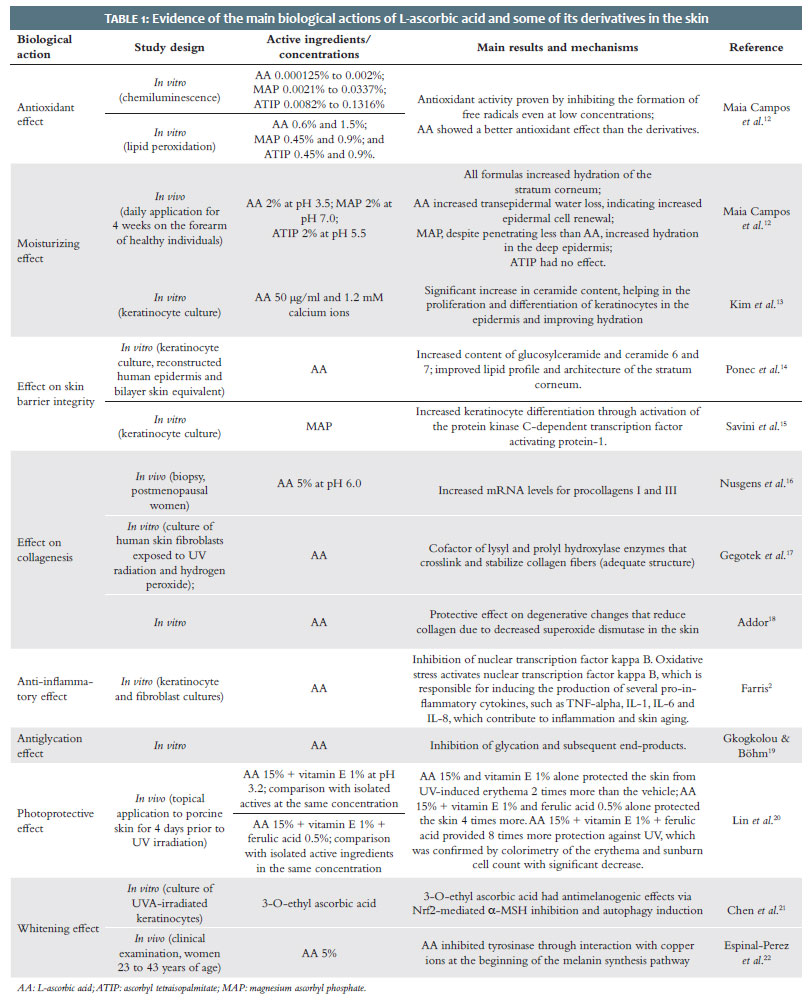
The most discussed functions of AA in the literature are its ability to neutralize free radicals (including reactive oxygen species) and its relevance in collagen synthesis. Table 1 summarizes the evidence of these and the other functions of AA and some of its derivatives in the skin, including anti-inflammatory action, photoprotection, its importance in the skin barrier function, antiglycation action, and brightening action.2,8–11
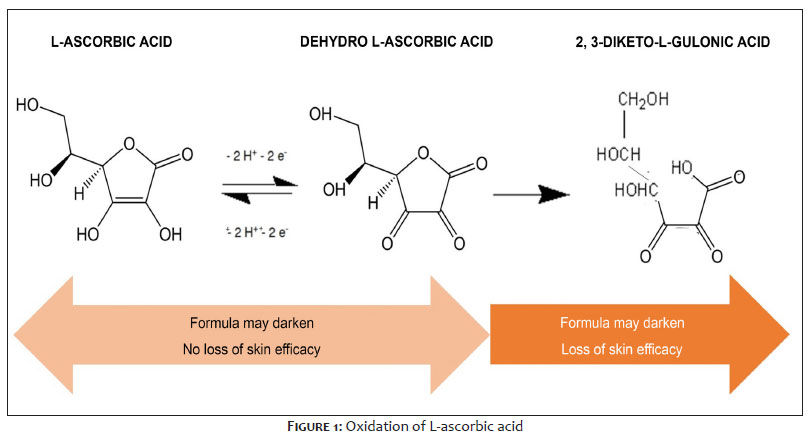
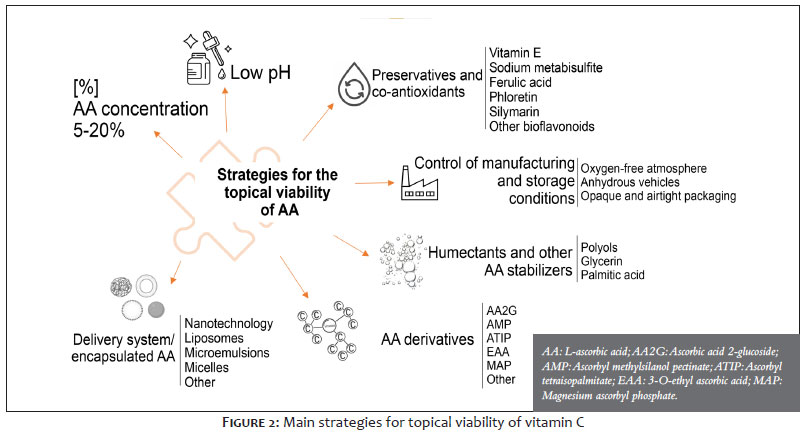
In topical formulations whose main active ingredients are antioxidants, factors such as compatibility, stability, and penetration must be prioritized, ensuring that their action is synergistic and that the active ingredients are not neutralized in the vehicle.7,20 One of the main challenges in using AA is to ensure its chemical stability and topical bioavailability in a suitable vehicle.23,24 Eight types of serum sold in the Brazilian market were evaluated biweekly for AA content with ultra-high performance liquid chromatography, of which only three had concentrations ≥ 5% at baseline and after 60 days. It was also observed that the cost of the AA serum may be related to the product's quality and stability, since the most expensive samples had the highest concentrations of AA throughout the study.25 AA is a very unstable molecule that can easily oxidize, losing its antioxidant capacity, either by ionization in water at neutral or higher pH (greater stability is obtained at pH ≤ 4), or by exposure to light, high temperature, contact with air, or the occurrence of metal ions.26 In fact, AA initially degrades to dehydro-L-ascorbic acid in a reversible manner, but can be irreversibly hydrolyzed to 2,3-diketo-L-gulonic acid (Figure 1), losing its activity and degrading into small molecules. The reversible transformation of AA into dehydro-L-ascorbic acid in the skin functions as an oxidation-reduction system that allows cellular interaction and bioactivity of the two molecules.5 In formulations, the AA degradation process is generally accompanied by a gradual change in color,24 However, the isolated darkening of the formula cannot necessarily be considered as loss of dermatological efficacy, since it is also related to the concentration of free AA and bioavailability in the skin.25 Pinnell et al.7 studied the ideal parameters for enabling percutaneous absorption of AA and supplementing the skin's natural antioxidant reservoir. They found that pure AA (pharmaceutical grade) should be formulated cold in an acidic medium (pH ≤ 3.5) to prevent ionic charge degradation.7 In addition to adjusting the pH, the formulation must contain an ideal concentration of AA (5 to 20%) to promote delivery of the active ingredient through the stratum corneum and hence achieve better results. When testing AA concentrations of 5 to 30% at pH 3.2, skin levels of AA increased, reaching their maximum at 20%, with decreased permeation tending to occur at higher concentrations.2,7 In addition to standardizing the physical-chemical parameters of pure and free AA solution, such as the ideal concentration and pH to ensure stability and dermal penetration,7,20,27 other strategies have been developed to overcome the limitations of topical administration (Figure 2). Efforts to make the topical administration of AA viable are only clinically important when the strategy not only stabilizes AA but ensures its safe penetration into the skin and that it remains free and stable long enough to perform its activity. Adding preservatives and co-antioxidants prevents the degradation of AA. Vitamin E, ferulic acid, and sodium metabisulfite have shown good results, although use of the latter is limited due to its odor.24,28 In addition to ferulic acid, other active plant-based ingredients can be used in synergistic antioxidant systems to stabilize AA.24,29 The flavonoid phloretin stabilizes and increases the cutaneous availability of topically applied AA and ferulic acid.29,30 The lipophilicity of phloretin, which indicates high solubility in skin lipids, can explain its use as a permeation enhancer for other active ingredients.29 Silymarin 0.5%, obtained from the Silybum marianum thistle, synergizes with AA 15% and ferulic acid 0.5% in an aqueous formulation with an acidic pH to reduce lipid peroxidation caused by exposure to UV radiation.31
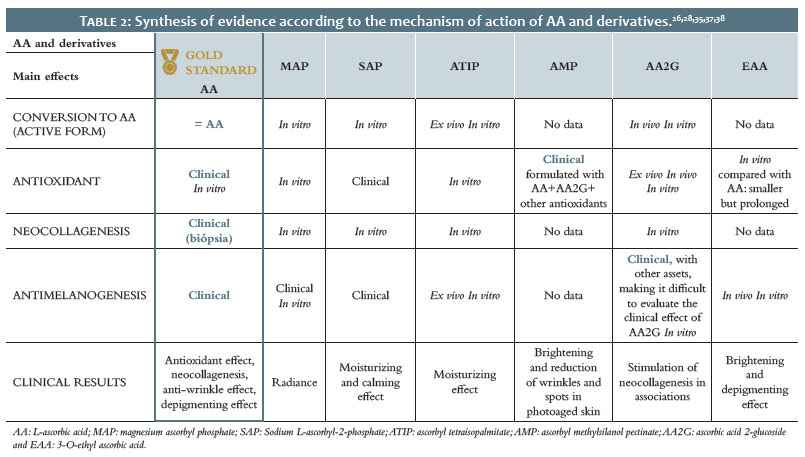
Degradation of topical AA can also be avoided by using polyol-type humectants and solvents, such as glycerin, propylene glycol, and butylene glycol for non-aqueous vehicles with low oxygen permeability.24 Humectants, such as palmitic acid, propanediol, and glycerin, have also positively influenced the stability of AA in anhydrous vehicles or emulsions.24 Based on these results, polyols have been used in water-in-silicone emulsions, with a formulation prepared in a nitrogen atmosphere, to associate pure AA in concentrations of 5 to 10% with glycerin and other polyols that, in addition to preventing contact between AA and the water in the emulsion, facilitate penetration and action directly in the dermis, where collagen fibers are formed.16,32 A number of AA derivatives have been proposed, and some are already being used in dermatology, to facilitate the permeation, stability, and bioavailability of AA. Generally, AA derivatives must be enzymatically converted to AA in keratinocytes and fibroblasts to have an effect.28,33 To date, however, no information could be found on the impact of AA derivatives on the skin's AA reservoir. However, the possibility of numerous combinations of AA derivatives with similar or different solubilities, and even with AA itself in the same formulation, could be advantageous.24 The main AA derivatives used in Brazil, both in industry and in compounding pharmacies, are magnesium ascorbyl phosphate,12,24,26,28 sodium L-ascorbyl-2-phosphate,24,28 ascorbyl tetraisopalmitate,12,24,28,34 ascorbyl methylsilanol pectinate,25,35 ascorbic acid 2-glucoside24,28,36–38 and 3-O-ethyl ascorbic acid21,28,39, which may be known by different trade names. However, the level of scientific evidence for the efficacy of AA is superior to that of derivatives (Table 2). Nanotechnology vectorization and encapsulation have been used to improve topical delivery of the active ingredient and protect AA from degradation.24 These systems include microvectors and nanovectors, liposomes (double lipid membrane with hydrophilic content), microemulsions, and micelles, which can dynamically increase the stability of AA in search of more durable products. However, it is challenging to define the ideal concentration of AA or derivatives and the permeation of AA into the skin.24,28 In general, articles that address the vectorization process have not reported the concentration of free AA in the vectors.28,40
AA: L-ascorbic acid; MAP: magnesium ascorbyl phosphate; SAP: Sodium L-ascorbyl-2-phosphate; ATIP: ascorbyl tetraisopalmitate; AMP: ascorbyl methylsilanol pectinate; AA2G: ascorbic acid 2-glucoside and EAA: 3-O-ethyl ascorbic acid.
It has been demonstrated that liposomal formulations in vesicles with different lipid compositions containing AA have increased the stability of AA and promoted greater skin retention, suggesting efficacious treatment of skin photoaging.41 The negative liposomal charge favored retention of the active ingredient in the epidermis and dermis.40 Nanotechnology has led to the development of several raw materials for cosmetics (nanovectors, nanocapsules, nanosomes, ethosomes, niosomes, and other nanometric systems) that improve the stability and permeation of AA in the skin, based on different types of materials. Although the supply of dermatological products and ingredients for compounding AA or nanoencapsulated AA derivatives is growing, there are still few studies, especially in vivo studies, regarding the targeting, permeation, and, most importantly, the concentration of free AA delivered to the skin through nanotechnology.33,41,42 In Brazil, magnesium ascorbyl phosphate is available through commercial encapsulation systems in collagen and chondroitin sulfate of marine origin, in both micro- and nanospheres, which reinforce the stability of the derivative to increase skin permeation. However, even with nanotechnology, permeation appears to be limited to the epidermis, with prolonged release of the content through enzymatic degradation.24,41 Ultradeformable elastic nanovesicles (spanlastics), formed mainly from alcohol, propylene glycol, polysorbate 80, and surfactants, which were loaded with AA and compared with AA solution at pH 2.38, have shown better permeation and cutaneous concentration at a dose sufficient to demonstrate antioxidant efficacy, lower metalloproteinase expression in vitro, and clinical improvement of UVB-damaged skin according to histological evaluation.33,43 Nanotechnology requires quality control and particle size control during manufacturing. To ensure safety for topical use, vectors > 100 nm are recommended to avoid the risk of systemic permeation. Few articles have demonstrated the cutaneous bioavailability of AA in nanotechnology formulations, and limited information is available about the concentration of either AA or the derivative used in the delivery system. In general, few studies have compared AA and its nanotechnological form, despite evidence that nanoparticles can release AA for > 8 h in vitro.44 Although nanotechnology is promising for cosmetics, there are regulatory and industrial issues that limit its clinical use.24 It is difficult to determine the specificity and clinical efficacy of each nanotechnological formulation of AA and derivatives.24,28,33 RNA or DNA structures with high affinity and specificity for targets of interest, called aptamers, were the subject of a recent study on AA delivery. The DNA and AA aptamer was proposed as a new possibility for stabilizing AA in cosmetics.33
Both the topical application of AA and its delivery to the skin layers are intrinsically dependent on the characteristics of the formulation.7,24,26 However, comparative studies assessing the stability and effective transdermal penetration of different forms of AA are generally limited to in vitro studies.24,26 Pinnell et al.7 tested two products commercially available in the United States that contain AA derivatives (associated with magnesium ascorbyl phosphate 12% and ascorbyl palmitate 10%) in comparison with a formulation of pure AA 15% (free and stabilized at pH 3.2). Unlike ideally parameterized AA, topical application of formulations with AA derivatives did not significantly increase the AA content in the skin.7 Despite being more stable, these AA derivatives appear to have lower skin penetration than free AA and do not have direct antioxidant activity, requiring conversion to AA by enzymatic reaction.24,26 Later studies indicated that esterifying AA with palmitic acid does not guarantee satisfactory stability levels in topical products, despite the lipid nature of ascorbyl palmitate, probably because it interferes with the barrier function and antioxidant action of vitamin E in the skin.24,26,45 One study suggested using AA 2-glucoside, a derivative of AA, in cosmeceuticals, although its antioxidant activity is lower than that of AA.36 In this derivative, a glucose molecule associated with the hydroxyl group of the second carbon atom of AA protects it from high temperatures, pH, metal ions, light, and other degradation mechanisms. In the skin, it reacts with the alpha-glucosidase enzyme to release AA.36 Thus, AA 2-glucoside was shown to be chemically stable and completely metabolized into AA, which guaranteed antioxidant efficacy (in vitro and ex vivo) at concentrations lower than those recommended for pure and free AA, although in vivo it had lower antioxidant action than AA plus vitamin E.28,37 Another study suggested that AA 2-glucoside may protect cells against ionizing radiation by acting against free radicals, reducing initial DNA damage.38 It has been observed that 3-O-ethyl AA is more lipophilic than AA 2-glucoside, which makes it more easily absorbed by the skin than other water-soluble AA derivatives.39 Several mechanisms have been proposed for the antimelanogenic effect of 3-O-ethyl AA: increased autophagy in melanocytes19; inhibition of alpha melanocyte-stimulating hormone and increase in endogenous antioxidants via Nrf2 in keratinocytes21; lower activity of the transcription factor that regulates melanogenesis in melanocytes21; and lower tyrosinase activity through melanocyte cytoplasmic acidification.46 It was also observed that AA plus magnesium ascorbyl phosphate has lower melanin and tyrosinase activity due to cytoplasmic acidification, which could result from increased transportation of AA across the membrane by the sodium-dependent vitamin C transporter-2.46 This mechanism is an efficient way to inhibit tyrosinase without causing cytotoxicity to melanocytes.46 Encapsulating AA 5% in emulsions containing liquid crystals, based on a combination of cetyl alcohol and polysorbate 60, formed a complex colloidal structure at the oil-water interface that efficiently stabilized AA for 4 months. Subsequently, a controlled clinical trial evaluated the effects of topical application of this stabilized form for 30 days compared to placebo, finding dermal redensification in high-frequency ultrasound measurements.23 Regardless of the strategy used to keep AA stable, the molecule must remain in or be converted into its free form to perform its biological activity.24,32 It has been found that the bioavailability of free AA in the skin layers (up to the dermis) could be increased by optimizing transcutaneous penetration through the following molecule stabilization parameters: AA in pharmaceutical grade purity; concentrations ranging from 5 to 20%, formulation at a low pH (2-4) and the presence of co-antioxidants, such as bioflavonoids and/or vitamin E.7,26 Using a non-invasive method (Raman spectroscopy), a recent study assessed AA penetration in the skin of 10 healthy individuals after topical application of a serum containing 15% pure AA, free and stabilized at a low pH in combination with other antioxidants (vitamin E 1% and ferulic acid 0.5%). There was a significant increase in total AA in the upper layers of the skin 1h and 6h after application, as well as a significant increase of AA in the dermis after 6h, which demonstrated the epidermal and dermal bioavailability of AA in this serum.27 Raman spectroscopy has also been used in vivo to compare an emulsion containing lipophilic derivatives of vitamins A, C (ascorbyl tetraisopalmitate), and E with an emulsion containing nanoparticles of these derivatives. The nanoparticles contributed to greater penetration of ascorbyl tetraisopalmitate and vitamin E derivative in terms of speed and depth, but they did not significantly improve the penetration of the vitamin A derivative. Although, in both emulsions, the three derivatives penetrated rapidly into the stratum corneum, the nanoparticles did not contribute to deeper penetration and, after 6 h, the lipophilic derivatives had penetrated only to the upper layers of the epidermis.47
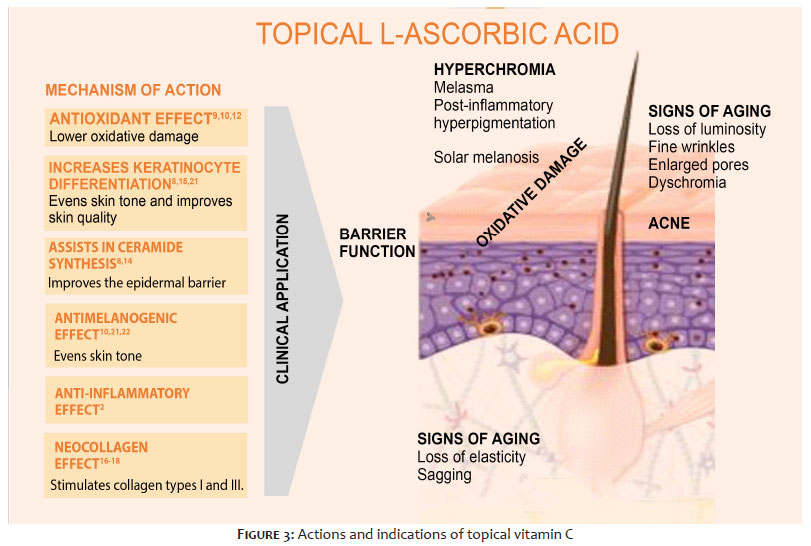
The clinical strategies and applicability of AA in dermatology are quite broad, since the skin requires a high concentration of AA to remain healthy. Topical use (Figure 3) is recommended mainly to treat skin aging, prevent photoaging, and reduce hyperpigmentation, increasing the uniformity of skin tone.1,9
AA has been shown to be a potent topical antioxidant that neutralizes free radicals, which tend to accumulate in the skin due to exposure to exposomal factors, such as UV radiation, pollution, and smoking, which induce or aggravate dermatosis.8,18 This activity is particularly important in the epidermis and corroborates the role of AA as a water-soluble component of the skin's antioxidant defense system, which is regulated by a complex network of enzymatic and non-enzymatic antioxidants, exogenous or endogenous, that protect the intra- and extracellular spaces from free radicals and, consequently, slow the skin aging process.6,18
In addition to protecting against exposure damage, AA is essential for collagen synthesis and regulation of the collagen/elastin balance in the dermis. In a double-blind, controlled trial of 10 individuals with clinical photodamage to the face, 12 weeks of AA 10% treatment reduced photoaging scores and improved facial wrinkles and skin texture on the AA-treated side compared to the placebo side.9,48 In addition to clinical improvement, biopsies have shown increased collagen in the dermis.16,48 A significant improvement in skin histology and clinical appearance was observed in another double-blind, placebo-controlled trial using topical, free AA 5% stabilized in a cream applied to 20 individuals over a six-month period.16,32 The efficacy of AA and its derivatives for skin rejuvenation can be synergistically enhanced through combination with other active ingredients,49,50 such as amino acids, peptides, growth factors, hyaluronic acid, vitamin E, and other antioxidants.28,33 The patient's therapeutic routine may require combination with other active ingredients, such as salicylic acid, niacinamide, or retinol.28 Amino acids, in particular glycine, proline, and lysine or their precursors, can facilitate collagen production.33 Reinforcing the relevance of the synergy of active ingredients in anti-aging efficacy, a gel-cream containing AA 5%, mannose 5%, and fragmented hyaluronic acid demonstrated clinical efficacy in reducing fine wrinkles and sagging, while increasing hydration, luminosity, and skin tone uniformity, which was corroborated by an in vitro study in an equivalent dermis model.50 In an ex vivo study, Neves et al. assessed a serum containing AA 15% associated with neohesperidin, Pinus pinaster bark extract (trade name Pycnogenol), tocopherol, and hyaluronic acid, which, compared to the vehicle, reduced mRNA gene expression of inflammatory mediators associated with skin aging induced by air pollution.49 The same formulation was tested for 90 days in a clinical and instrumental study (n=40), and it was found capable of reducing signs of skin aging, improving the structure of the dermoepidermal junction and reducing pigmentation of the basement membrane. Thus, it proved efficient in protecting the skin against pigmentation/skin aging induced by air pollution.49
In addition to its effects on signs of skin aging, AA also plays a role in the treatment and prevention of skin hyperpigmentation. Melanocytes are highly susceptible to oxidative damage, since melanogenesis is a pro-oxidative pathway. Thus, AA acts on melanogenesis by combating free radicals and inhibiting tyrosinase. In addition, AA favors the differentiation of keratinocytes and improves dermoepidermal cohesion, contributing to uniform skin tone.8,22 Topical AA can help treat melasma and aid in skin maintenance after procedures for solar melanosis.24,26,28 AA 5% and hydroquinone 4% in water-in-oil emulsions were compared in a for 16-week double-blind trial conducted in 16 individuals with melasma (phototypes IV and V). Although there was a faster and much better clinical response with hydroquinone (93.75% showed good to excellent improvement), adverse effects occurred in 68.75% of the patients, while on the side treated with AA they occurred in only 6.25% of the patients, which showed positive results (good to excellent improvement) in 62.5% of cases.22
Topical application of AA and derivatives has been combined with procedures such as ultrasound, iontophoresis, ablative laser, microneedling, and microdermabrasion to increase the penetration and effects of AA.33,51 The use of iontophoresis after topical application of AA increases the percutaneous absorption of the active ingredient in comparison with simple topical application. A controlled trial investigated 24 individuals treated with a serum containing AA 10% to the entire face and, on only one side, used a portable iontophoresis device at home twice a week for 8 weeks. Standardized images and corneometer measurements were made every 2 weeks, showing significant improvement in hydration and pore closure, although the device had less power than the model developed for medical use.52 Previous studies have shown that iontophoresis following topical application of AA increases collagen production.33 Fractional lasers have been used by dermatologists to treat signs of skin aging, and these procedures can substantially consume skin antioxidants. Combining the procedure with topical AA may reduce inflammation and help restore the skin.51 A study demonstrated that after a fractional laser procedure, 7 daily applications of a serum containing AA 15% (stabilized at acidic pH) in association with ferulic acid and vitamin E reduced edema and erythema more rapidly than the vehicle (hemifacial; n=15). Overall, the serum was well tolerated immediately after fractional laser treatment, and the acidic pH helped inhibit infection. Furthermore, compared to the vehicle, the AA serum prevented a reduction of basic fibroblast growth factor. This marker is important not only in the proliferation of fibroblasts, but also in the synthesis of extracellular matrix macromolecules (glycosaminoglycans and hyaluronic acid) and inhibition of matrix metalloproteinase-1.51 More recently, an article proposed topical application of a serum with AA 15% stabilized at acidic pH and associated with vitamin E and ferulic acid as an adjuvant treatment with Q-Switched Nd:YAG laser therapy. A comparative controlled trial included 18 men and women with melasma or solar melanosis, who applied the serum twice a day for 2 weeks after the laser procedure. On the treated side, they presented a significant reduction in melanin index, but not in post-procedure erythema.53 This laser therapy's brightening potential also enhances the penetration of active topical brightening and antioxidant ingredients for a synergistic effect. A case study on melasma treatment assessed the effect of a topical antioxidant serum containing AA 10% stabilized with phloretin and ferulic acid that was, for 120 days, applied daily and immediately after each biweekly Q-Switched laser session as an adjuvant treatment, due to the role of oxidative stress in this type of dermatosis.54 These practices are consistent with integrated skin care that combines in-office treatments with at-home products to achieve complementary clinical benefits and reduce unwanted side effects. These studies support the efficacy of topical AA application immediately after deliberate barrier-breaking procedures, but the use of cosmetics for post-procedure AA delivery is under investigation by regulatory authorities.33,51
A range of dermocosmetics that include AA is available to dermatologists, featuring different packaging, concentrations, and textures, mainly in serum, gel-cream, and cream forms.3 While product availability makes it easier to adapt to the daily routine of patients, it also requires dermatologists to have in-depth knowledge of pharmacotechnical techniques to best adapt AA therapy to the clinical needs of each patient. In addition to considering the concentration, quality, and molecular form of AA, it is important to select a vehicle that presents a sensory experience adapted to the patient's skin type and profile, which facilitates treatment adherence. However, the main indication for AA in daily facial care seems to be the stimulation of collagen synthesis, which prevents and reduces signs of skin aging, smoothing fine wrinkles, and promoting perceived improvement in skin vitality, brightness, and firmness.28 To this end, the active form of AA should reach deeper layers of the skin, ideally the dermis. Although AA does not absorb UV radiation, its undeniable ability to neutralize free radicals has justified the use of topical AA as a daily antioxidant (before applying sunscreen) to optimize protection against exposomal damage and, consequently, reduce the degradation of collagen and elastin, preventing signs of skin aging.9 Using topical AA to maintain the skin's antioxidant reservoir at adequate levels is an adjuvant strategy to the daily use of sunscreen. These are important complementary mechanisms,7 since UV radiation and high ozone levels due to pollution deplete vitamins C and E from the skin's surface.1,7 Furthermore, laboratory studies have demonstrated a significant reduction in UVB-induced erythema after topical application of AA 10%.2 AA derivatives have been added to sunscreens to prevent lipid peroxidation in oily and acne-prone skin, but the effects of each formula must be verified in vivo. For everyday use, AA has been shown to be a safe active ingredient, even with prolonged use5 in all skin types, including sensitive skin.8,54 However, some products may include warnings about the possibility of skin discomfort due to the high concentration of AA, suggesting a longer interval between applications.5 For sensitive skin, formulations with very low pH should be avoided due to the possibility of irritation. Specific products have been developed for these individuals that combine soothing ingredients, such as acetyl dipeptide-1 cetyl ester (trade name Neurosensine), with 5% to 10% pure and free AA stabilized at pH 4.0 to 6.0 to reduce the possibility of sensitization. Formulations with AA derivatives (stable at pH 5 to 7) or nanoencapsulated AA promise less irritation and also seem suitable for those with sensitive skin. Dermocosmetics with AA are often indicated for use once or twice a day, and deciding about the most suitable product is influenced by several factors, such as a history of sensitive skin, the degree of oiliness, age, the individual needs of each patient, as well as the relationship between AA concentration and skin permeation.9,27,28,40 Clinical trials of topical products containing AA are increasingly important, since different vehicles and combinations with other active ingredients can have different results. The results of AA derivatives can also differ from the free form, even when using the same vehicle. Because interactions between the ingredients can be unpredictable, dermatological studies and clinical evaluations must be performed on each formula to provide clinical confidence. In vitro studies, which indicate possible mechanisms of action, cannot guarantee the same efficacy in vivo. Proof of a product's efficacy must be based on clinical trials. Table 2 shows that, at present, only free AA has shown clinical efficacy and, thus, is considered the gold standard molecule in dermatology. Furthermore, it has been demonstrated that free AA, stabilized in its active form, has the best penetration in both the epidermis and the dermis, preventing and treating of signs of skin aging and skin hyperpigmentation.7,20,30 There are still few comparative studies between AA and its derivatives or standardized clinical trials on different forms developed to provide greater topical efficacy. Thus, new studies are needed to fill this gap. This review has led to the following conclusions: increasingly higher concentrations of AA do not result in more effective products7; in addition to the concentration, the effectiveness of AA depends on the chemical form, vehicle, and even the packaging; pure AA, although easily oxidizable, can be stabilized at an acidic pH and through association with co-antioxidant active ingredients, as well as through specific technologies (polyols, for example); not all AA derivatives can release AA into the skin, and many only permeate the superficial epidermal layers; although some products report that nanovectors containing AA derivatives are can release AA equivalents, no clinical trials have validated this information.
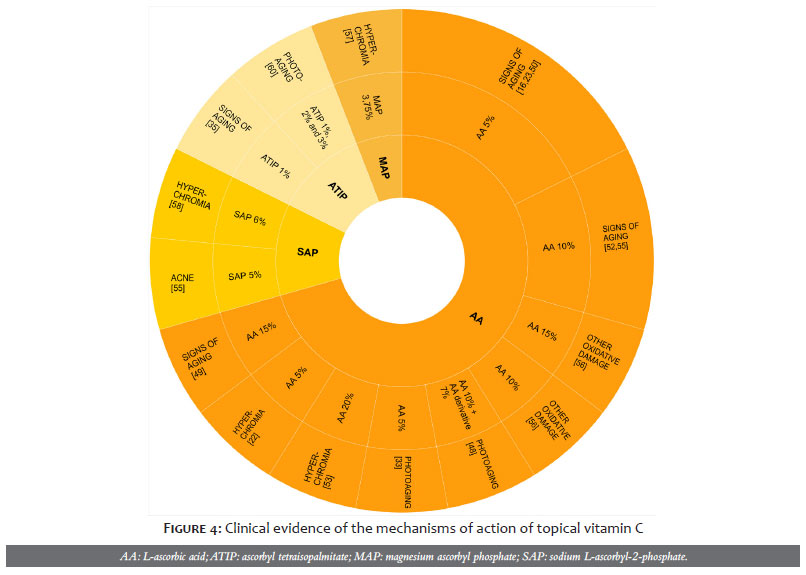
Numerous forms of AA are already available for topical use in dermatology, being recommended for the prevention and treatment of signs of photoaging, either as monotherapy or in combination with other active ingredients or in-office procedures. Clinical practice should be based on published evidence and should encourage research, in addition to transparency regarding technical information, efficacy and safety. For each formulation, the stability, penetration, and bioavailability of AA in the skin must be assessed, and data on clinical efficacy and patient adaptation to the product must be provided. AA is still the gold standard molecule for clinical practice (Figure 4) due to the higher level of evidence16,22,23,32,48–50,52,53 regarding its mechanisms of action and clinical activity than other derivatives34,55–60 and molecules available through nanotechnology.
Flavia Alvim Sant'anna Addor
ORCID: 0000-0003-1851-7342
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, critical review of the literature, critical review of the manuscript.
Ana Claudia Cavalcante Esposito
ORCID: 0000-0001-9283-2354
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, critical review of the literature, critical review of the manuscript.
Emerson de Andrade Lima
ORCID: 0000-0002-6132-5031
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, critical review of the literature, critical review of the manuscript.
Lucas Portilho
ORCID: 0000-0001-9399-1664
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, critical review of the literature, critical review of the manuscript.
Eliana Mika Yamaguchi
ORCID: 0009-0002-0241-3928
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, critical review of the literature, critical review of the manuscript.
Sylvia Ypiranga
ORCID: 0009-0002-8440-0214
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, critical review of the literature, critical review of the manuscript.
1. Burke KE. Mechanisms of aging and development—a new understanding of environmental damage to the skin and prevention with topical antioxidants. Mech Ageing Dev. 2018;172:123-30.
2. Farris PK. Cosmetical vitamins: vitamin c. In: Draelos ZD, Dover JS, Alam M [editors]. Cosmeceuticals e-book: procedures in cosmetic dermatology series. 1st ed. Elsevier Health Sciences; 2014:37-42.
3. Fact.MR. Skincare serums market analysis - global market insights 2022 to 2032.
4. Manela-Azulay M, Bagatin E. Cosmeceuticals vitamins. Clin Dermatol. 2009;27(5):469-74.
5. Vasques LI, Vendruscolo CW, Leonardi GR. Topical application of ascorbic acid and its derivatives: a review considering clinical trials. Curr Med Chem. 2023;30(29):3272-286.
6. Burke KE. Prevention and treatment of aging skin with topical antioxidants. In: Skin Aging Handbook. Elsevier; 2009:149-76.
7. Pinnell SR, Yang H, Omar M, Monteiro-Riviere N, DeBuys HV, Walker LC, et al. Topical L-ascorbic acid: percutaneous absorption studies. Dermatol Surg. 2001;27(2):137-42.
8. Wang K, Jiang H, Li W, Qiang M, Dong T, Li H. Role of vitamin C in skin diseases. Front Physiol. 2018;9.
9. Al-Niaimi F, Chiang NYZ. Topical vitamin C and the skin: mechanisms of action and clinical applications. J Clin Aesthet Dermatol. 2017;10(7):14-7.
10. Pullar JM, Carr AC, Vissers MCM. The roles of vitamin C in skin health. Nutrients. 2017;9(8).
11. Pinnell SR. Cutaneous photodamage, oxidative stress, and topical antioxidant protection. J Am Acad Dermatol. 2003;48(1):1-22.
12. Campos PMBGM, Gonçalves GMS, Gaspar LR. In vitro antioxidant activity and in vivo efficacy of topical formulations containing vitamin C and its derivatives studied by non-invasive methods. Skin Res Technol. 2008;14(3):376-380.
13. Kim KP, Shin KO, Park K, Yun HJ, Mann S, Lee YM, Cho Y. Vitamin c stimulates epidermal ceramide production by regulating its metabolic enzymes. Biomol Ther (Seoul). 2015;23(6):525-30.
14. Ponec M, Weerheim A, Kempenaar J, Mulder A, Gooris GS, Bouwstra J, et al. The formation of competent barrier lipids in reconstructed human epidermis requires the presence of vitamin c. J Invest Dermatol. 1997;109(3):348-55.
15. Savini I, Catani MV, Rossi A, Duranti G, Melino G, Avigliano L. Characterization of keratinocyte differentiation induced by ascorbic acid: protein kinase c involvement and vitamin c homeostasis. J Invest Dermatol. 2002;118(2):372-79.
16. Nusgens BV, Humbert P, Rougier A, Colige AC, Haftek M, Lambert CA, et al. Topically applied vitamin c enhances the mRNA level of collagens I and III, their processing enzymes and tissue inhibitor of matrix metalloproteinase 1 in the human dermis. J Invest Dermatol. 2001;116(6):853-9.
17. Gęgotek A, Bielawska K, Biernacki M, Zaręba I, Surażyński A, Skrzydlewska E. Comparison of protective effect of ascorbic acid on redox and endocannabinoid systems interactions in in vitro cultured human skin fibroblasts exposed to UV radiation and hydrogen peroxide. Arch Dermatol Res. 2017;309(4):285-303.
18. Addor FAS. Antioxidants in dermatology. An Bras Dermatol. 2017;92(3):356-62.
19. Gkogkolou P, Böhm M. Advanced glycation end products: keyplayers in skin aging? Dermatoendocrinol. 2012;4(3):259-70.
20. Lin FH, Lin JY, Gupta RD, Tournas JA, Burch JA, Selim MA, et al. Ferulic acid stabilizes a solution of vitamins c and e and doubles its photoprotection of skin. J Invest Dermatol. 2005;125:826-32.
21. Chen SJ, Hseu YC, Gowrisankar YV, et al. The anti-melanogenic effects of 3-O-ethyl ascorbic acid via Nrf2-mediated α-MSH inhibition in UVA-irradiated keratinocytes and autophagy induction in melanocytes. Free Radic Biol Med. 2021;173:151-69.
22. Espinal-Perez LE, Moncada B, Castanedo-Cazares JP. A double-blind randomized trial of 5% ascorbic acid vs. 4% hydroquinone in melasma. Int J Dermatol. 2004;43(8):604-7.
23. Vergilio MM, Aiello LM, Furlan AS, Caritá AC, Azevedo JR, Boliznger MA, et al. In vivo evaluation of topical ascorbic acid application on skin aging by 50 MHz ultrasound. J Cosmet Dermatol. 2022;21(10):4921-6.
24. Caritá AC, Fonseca-Santos B, Shultz JD, Michniak-Kohn B, Chorilli M, Leonardi GR. Vitamin c: one compound, several uses. advances for delivery, efficiency and stability. Nanomedicine. 2020;24:102117.
25. Pizzo JS, Cruz VHM, Rodrigues CA, Manin LP, Visentainer L, Santos OO, et al. Rapid determination of L-ascorbic acid content in vitamin c serums by ultra-high-performance liquid chromatography– tandem mass spectrometry. Int J Cosmet Sci. 2022;44(1):131-41.
26. Stamford NPJ. Stability, transdermal penetration, and cutaneous effects of ascorbic acid and its derivatives. J Cosmet Dermatol. 2012;11(4):310-7.
27. Silva GC, Pinto L, Neto M, et al. Evaluation of vitamin C permeability in the human skin using raman spectroscopy after topical application of a serum containing 15% L-ascorbic acid, 1% vitamin E and 0.5% ferulic acid. In: Poster P0447 EADV. 2020.
28. Enescu CD, Bedford LM, Potts G, Fahs F. A review of topical vitamin C derivatives and their efficacy. J Cosmet Dermatol. 2022;21(6):2349-59.
29. Casarini TPA, Frank LA, Pohlmann AR, Guterres SS. Dermatological applications of the flavonoid phloretin. Eur J Pharmacol. 2020;889.
30. Oresajo C, Stephens T, Hino PD, Law RM, Yatskayer, Foltis P, et al. Protective effects of a topical antioxidant mixture containing vitamin c, ferulic acid, and phloretin against ultraviolet-induced photodamage in human skin. J Cosmet Dermatol. 2008;7(4):290-7.
31. Brieva P, Lynch SM, Su M, Sverdlove MJ, Murtaugh-Frey AN, Galdi A. Serums for reducing lipid peroxidation. US.Patent Number 11446233. 2022.
32. Humbert PG, Haftek M, Creidi P, Lapiere C, Nusgens B, Richard A, et al. Topical ascorbic acid on photoaged skin. clinical, topographical and ultrastructural evaluation: double-blind study vs. placebo. Exp Dermatol. 2003;12(3):237-44.
33. Boo YC. Ascorbic acid (vitamin c) as a cosmeceutical to increase dermal collagen for skin antiaging purposes: emerging combination therapies. Antioxidants. 2022;11(9):1663.
34. Campos PMBGM, Gianeti MD, Camargo FB, Gaspar LR. Application of tetra- isopalmitoyl ascorbic acid in cosmetic formulations: stability studies and in vivo efficacy. Eur J Pharm Biopharm. 2012;82(3):580-6.
35. Bretas B, Mota A, Gianeti M, Seixas V, Lima M, Schwarzer R, et al. Reflectance confocal microscopy and image analysis to evaluate the efficacy of a topical facial serum with 20% vitamin c in improving signs of aging. J Am Acad Dermatol. 2018;79(3):AB243.
36. Huang WY, Lee PC, Huang LK, Lu LP, Liao WC. Stability studies of ascorbic acid 2-glucoside in cosmetic lotion using surface response methodology. Bioorg Med Chem Lett. 2013;23(6):1583-7.
37. Jacques C, Genies C, Bacqueville D, Tourette A, Borotra N, Chaves F, et al. Ascorbic acid 2-glucoside: an ascorbic acid pro-drug with longer-term antioxidant efficacy in skin. Int J Cosmet Sci. 2021;43(6):691-702.
38. Maeda J, Allum AJ, Mussallem JT, Froning CE, Haskins AH, Buckner MA, et al. Ascorbic acid 2-glucoside pretreatment protects cells from ionizing radiation, UVC, and short wavelength of UVB. Genes (Basel). 2020;11(3):238.
39. Iliopoulos F, Sil BC, Moore DJ, Lucas RA, Lane ME. 3-O-ethyl-l-ascorbic acid: characterisation and investigation of single solvent systems for delivery to the skin. Int J Pharm X. 2019;1.
40. Maione-Silva L, Castro EG, Nascimento TL, Cintra ER, Moreira LC, Cintra BAS, et al. Ascorbic acid encapsulated into negatively charged liposomes exhibits increased skin permeation, retention and enhances collagen synthesis by fibroblasts. Sci Rep. 2019;9(1).
41. Gupta V, Mohapatra S, Mishra H, Farooq U, Kumar K, Ansari MJ, et al. Nanotechnology in cosmetics and cosmeceuticals—a review of latest advancements. Gels. 2022;8(3):173.
42. Choi S, Han J, Kim JH, Kim AR, Kim SH, Lee W, et al. Advances in dermatology using DNA aptamer "Aptamin C" innovation: oxidative stress prevention and effect maximization of vitamin c through antioxidation. J Cosmet Dermatol. 2020;19(4):970-6.
43. Elhabak M, Ibrahim S, Abouelatta SM. Topical delivery of l-ascorbic acid spanlastics for stability enhancement and treatment of UVB induced damaged skin. Drug Deliv. 2021;28(1):445-53.
44. Kandil SM, Soliman II, Diab HM, Bedair NI, Mahrous MH, Abdou EM. Magnesium ascorbyl phosphate vesicular carriers for topical delivery: preparation, in-vitro and ex-vivo evaluation, factorial optimization and clinical assessment in melasma patients. Drug Deliv. 2022;29(1):534-47.
45. Meves A, Stock SN, Beyerle A, Pittelkow MR, Peus D. Vitamin c derivative ascorbyl palmitate promotes ultraviolet-b-induced lipid peroxidation and cytotoxicity in keratinocytes. J Invest Dermatol. 2002;119(5):1103-8.
46. Miao F, Su MY, Jiang S, Luo LF, Shi Y, Lei TC. Intramelanocytic acidification plays a role in the antimelanogenic and antioxidative properties of vitamin c and its derivatives. Oxid Med Cell Longev. 2019;2019.
47. Mogilevych B, Isensee D, Rangel JL, Dal Pizzol C, Martinello VCA, Dieamant GC, et al. Study of the vitamins a, e and c esters penetration into the skin by confocal raman spectroscopy in vivo. Biophot S Am. 2015:95312A.
48. Fitzpatrick RE, Rostan EF. Double-blind, half-face study comparing topical vitamin c and vehicle for rejuvenation of photodamage. Dermatol Surg. 2002;28:231-36.
49. Neves JR, Grether-Beck S, Krutmann J, Correia P, Gonçalves Júnior JE, Sant'Anna B, et al. Efficacy of a topical serum containing L-ascorbic acid, neohesperidin, pycnogenol, tocopherol, and hyaluronic acid in relation to skin aging signs. J Cosmet Dermatol. 2022;21(10):4462-9.
50. Lesqueves MHS, Caixeta CM, Ribeiro NM. In vivo and in vitro evaluation of the cutaneous anti-aging efficacy of a product containing vitamin C, fragmented hyaluronic acid, and mannose. Surg Cosmet Dermatol. 2015;7(1):37-44.
51. Waibel JS, Mi QS, Ozog D, Qu L, Zhou L, Rudnick A, et al. Laser-assisted delivery of vitamin c, vitamin e, and ferulic acid formula serum decreases fractional laser postoperative recovery by increased beta fibroblast growth factor expression. Lasers Surg Med. 2016;48(3):238-44.
52. Yan C, Ng JNC, Wanitphakdeedecha R. Efficacy of handheld iontophoresis device in enhancing transdermal vitamin c delivery: a split-face clinical trial. J Cosmet Dermatol. 2022;21(2):698-706.
53. Kim J, Kim J, Lee YI, Almurayshid A, Jung JY, Lee JH. Effect of a topical antioxidant serum containing vitamin c, vitamin e, and ferulic acid after Q-switched 1064-nm Nd:YAG laser for treatment of environment-induced skin pigmentation. J Cosmet Dermatol. 2020;19(10):2576-82.
54. Campos V. 28379 Case report of effect of a topical antioxidant serum containing vitamin C, ferulic acid, and phloretin after Q-switched laser for treatment of melasma. J Am Acad Dermatol. 2021;85(3):AB186.
55. Escobar S, Valois A, Nielsen M, Closs B, Kerob D. Effectiveness of a formulation containing peptides and vitamin c in treating signs of facial ageing: three clinical studies. Int J Cosmet Sci. 2021;43(2):131-5.
56. Klock J, Ikeno H, Ohmori K, Nishikawa T, Vollhardt J, Schehlmann V. Sodium
57. ascorbyl phosphate shows in vitro and in vivo efficacy in the prevention and treatment of acne vulgaris. Int J Cosmet Sci. 2005;27(3):171-6.
58. Huh CH, Seo KI, Park JY, Lim JG, Eun HC, Park KC. A randomized, double-blind, placebo-controlled trial of vitamin c iontophoresis in melasma. Dermatology. 2003;206(4):316-20.
59. Ishikawa Y, Niwano T, Hirano S, Numano K, Takasima K, Imokawa G. Whitening
60. effect of l-ascorbate-2-phosphate trisodium salt on solar lentigos. Arch Dermatol Res. 2019;311(3):183-91.
61. Yokota M, Yahagi S. Evaluation of the anti-wrinkle effect of a lipophilic pro-vitamin c derivative, tetra-isopalmitoyl ascorbic acid. J Cosmet Dermatol. 2022;21(8):3503-14.
62. Valacchi G, Pecorelli A, Belmonte G, Pambianchi E, Cervellati F, Lynch S, et al. Protective effects of topical vitamin c compound mixtures against ozone-induced damage in human skin. J Invest Dermatol. 2017;137(6):1373-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}