


Bruna Cabral Meira Chaves1; Luciana Ballardin2; Felipe Bochnia Cerci2,3,4
Financial support: None.
Conflicts of interest: None.
Submitted on: 13/06/2024
Approved on: 25/06/2024
How to cite this article: Chaves BCM, Ballardin L, Cerci FB. Transposition flap for reconstruction of lower eyelid wounds adjacent to the tarsus after Mohs micrographic surgery: a case series. Surg Cosmet Dermatol. 2025;17:e20250379.
Skin cancers affecting the eyelid can be a reconstructive challenge due to the complexity of the local anatomy. In addition to precise eradication of the tumor, maximal preservation of the skin is essential for both functional and cosmetic outcomes. Transposition flaps represent an excellent reconstructive option, as they require few incisions and, when well planned, do not cause ectropion, a key consideration in this topography. We describe a case series of lower eyelid reconstructions adjacent to the tarsus following Mohs micrographic surgery, using transposition flaps.
Keywords: Surgical Flaps; Mohs Surgery; Skin Neoplasms; Eyelids; Eyelid Neoplasms.
INTRODUCTION
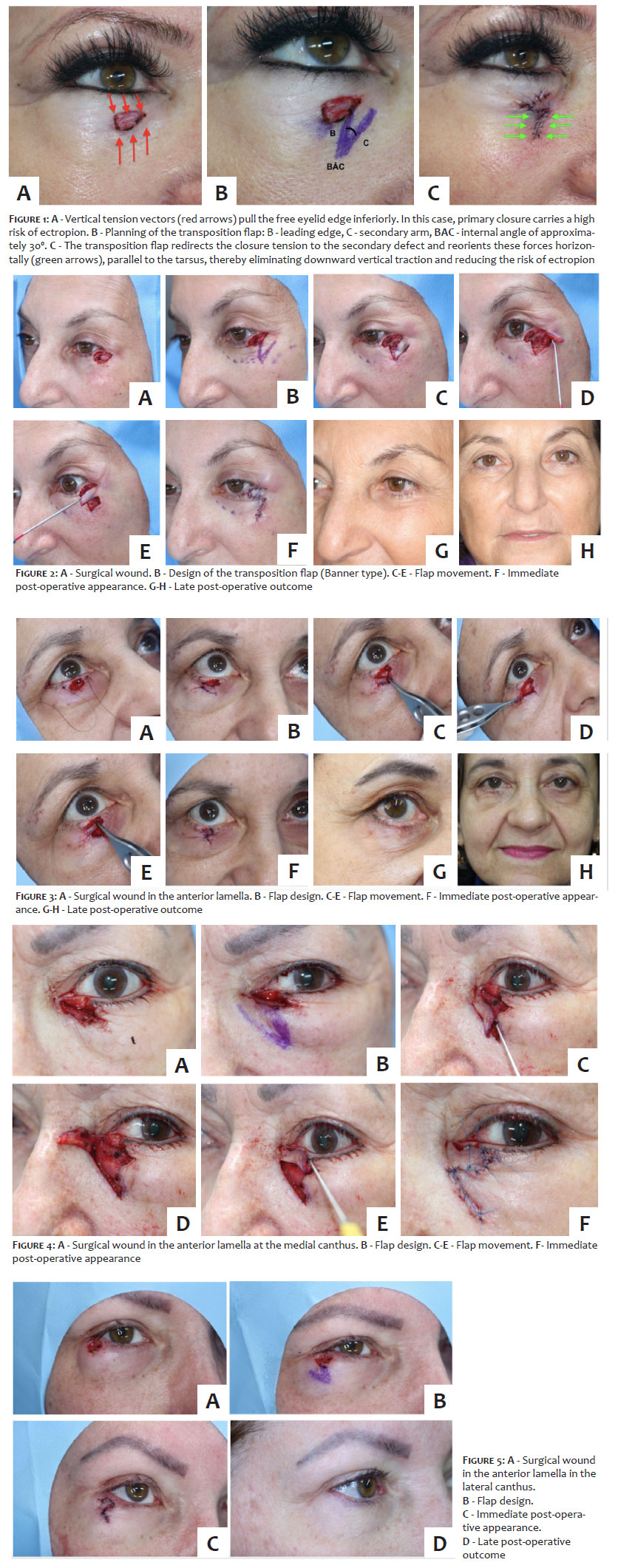
One in ten skin cancers occur in the periorbital region. Within this topography, the lower eyelid is the most commonly affected subunit, representing 55% of cases.1,2 Mohs micrographic surgery (MMS) is indicated in this region because, in addition to providing a higher oncologic remission rate, it maximizes preservation of healthy tissue and reduces surgical morbidity.3 The primary objective of eyelid reconstruction is to preserve function while achieving a good aesthetic result. In this area, primary horizontal closures are rarely feasible due to the risk of ectropion. Among the various flap options, transposition flaps offer a key advantage in free-margin regions, as they redirect the tension vectors involved in the closure, helping to prevent distortion of the eyelid margin. In addition, they require less tissue displacement compared to advancement or rotation flaps, further reducing surgical morbidity.4
CASE REPORTS
We present a case series of reconstructions of surgical defects of the lower eyelid adjacent to the tarsus, involving the anterior lamella (partial thickness). In some cases, the wound also involved a small portion of the tarsus. All reconstructions were performed using transposition flaps encompassing defects located in various regions of the lower eyelid, thereby demonstrating the versatility of this technique. Twelve patients with basal cell carcinoma underwent MMS, including 11 women and 1 man, with a mean age of 55 years (range: 43 to 80). All surgeries were performed in an outpatient setting under local anesthesia with 1% lidocaine and epinephrine. In cases involving the ciliary margin, 0.5% proxymetacaine hydrochloride anesthetic eye drops were added for greater patient comfort due to the proximity to the cornea. After achieving tumor-free margins with MMS, reconstruction was planned by designing the transposition flap to redirect vertical tension vectors into horizontal ones, thereby minimizing the risk of ectropion.
The classic rhomboid transposition flap, described by Limberg, is used to repair primary rhomboid defects with internal angles of 60º and 120º. DuFourmentel later modified Limberg's flap by reducing the internal angles of the rhombic defects to between 60º and 90º, thereby increasing its versatility and decreasing the size of the standing cones excised.4 Due to the pronounced elasticity of periocular tissue, modifying the flap into a triangular or Banner flap—with acute internal angles between 30º and 60º, without converting the defects into a rhomboid—preserves healthy tissue and offers the additional advantage of allowing greater flexibility in positioning the donor flap. The flap can thus be designed in the orientation best suited to the local tension vectors.5 In practical terms, the lobe of the transposition flap should be designed with consideration for how the donor area will be closed. In other words, the closure vector of the donor site must not create downward traction on the eyelid.
After appropriate planning, the flap was elevated in the subdermal or subcutaneous plane, when the donor area extended into the malar region. Whenever possible, the donor site was kept within the eyelid subunit due to the similarity in skin characteristics. The secondary defect was sutured in the subcutaneous and dermal planes with 5-0 poliglecaprone and in the superficial plane with 6-0 polypropylene. Due to the limited dermal thickness in the eyelid region, the flap was primarily sutured in the superficial plane. When the wound affected the ciliary margin, closure was performed using the minimum number of sutures necessary to avoid contact with the cornea. In these cases, the suture ends were left longer and directed inferiorly to reduce ocular discomfort. All the cases showed satisfactory outcomes, with preservation of both eyelid function and cosmetic appearance. No intraoperative or postoperative complications occurred, and no surgical revisions were required. Figures 1 to 6 illustrate some of these reconstructions.
DISCUSSION
In eyelid topography, beyond the precise eradication of the tumor, maximal preservation of the skin and soft tissues is essential for both functional and cosmetic reasons.1,3 However, due to the limited availability of redundant tissue in this area, there may be a temptation to reduce surgical margins when operating without intraoperative margin control, which increases the risk of inadequate excision. MMS is the recommended treatment for skin cancer of the eyelid. This technique allows for complete excision of the lesion through precise histologic control of surgical margins, resulting in higher oncologic cure.4 At the same time, MMS preserves healthy tissue, reducing wound size and facilitating reconstruction. In addition, it can help avoid full-thickness excision in smaller lesions, safely removing poorly defined tumors and reserving enucleation or exenteration for more complex cases.1-8
There are several reconstructive options following MMS in this region. The choice of repair and the surgical outcome depend, in part, on the surgeon's knowledge of eyelid anatomy and their ability to assess the reconstructive requirements of the post-MMS defect.2 In complex full-thickness cases, a multidisciplinary approach may be necessary. Transposition flaps are a safe option, as they require few incisions and, when well planned, do not lead to ectropion—an essential consideration in this anatomical region. Furthermore, they are quick and simple to perform and, when properly executed, yield excellent results.
Transposition flaps typically recruit skin from the same eyelid subunit and, due to the characteristic movement of this technique, redirect the closure tension vectors. The leading edge of the flap should be positioned perpendicularly to the eyelid edge, as the movement of the flap toward the primary defect causes a shift in the tension vectors, distributing the tensile forces to the secondary defect (Figure 1). To close the flap, the first suture should be placed at the proximal portion of the donor area, projecting the flap into the primary defect. To avoid ectropion, the primary tension vector must be oriented horizontally, parallel to the free eyelid margin.4 Flap preparation must be meticulous to preserve adequate vascularization, but thinning the flap is essential for an optimal outcome. Thick flaps may develop trapdoor deformity, and if this does not resolve after a few months, treatment with intralesional corticosteroid infiltration or surgical revision may be necessary.
Secondary intention healing can be useful for small defects, especially near the medial canthus. In other eyelid locations, this approach must be selected with caution, as wound contraction can lead to ectropion. Primary closure, may be appropriate for small to medium-sized defects if the tension vector is oriented parallel (or even oblique) to the eyelid margin; otherwise it is relatively contraindicated due to the risk of ectropion.2
Another reconstructive option is the full-thickness skin graft; however, contraction during the healing process may result in ectropion.2,8 Additional options include advancement and rotation flaps,2,6,7,9 which—due to vector dynamics—require larger incisions and more extensive dissection to recruit skin from the lateral face, thereby increasing surgical complexity and the risk of postoperative complications such as hematomas and bleeding, particularly in anticoagulated patients.
CONCLUSION
Transposition flaps are an important option for the repair of partial-thickness eyelid wounds adjacent to the tarsus and should be familiar to dermatologic surgeons. These flaps are safe, easy to perform, and, when properly planned, avoid extensive tissue dissection, provide adequate vascularization, and yield excellent functional and aesthetic outcomes, as demonstrated in this study.
Bruna Cabral Meira Chaves
ORCID: 00009-0009-8158-2017
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, data collection, analysis, and interpretation, literature review, critical review of the manuscript
Luciana Ballardin
ORCID: 00009-0000-2015-0629
Approval of the final version of the manuscript, preparation and writing of the manuscript, data collection, analysis, and interpretation, literature review
Felipe Bochnia Cerci
ORCID: 0000-0001-9605-0798
Approval of the final version of the manuscript, study design and planning, data collection, analysis, and interpretation, effective participation in research orientation, intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, literature review, critical review of the manuscript
REFERENCES:
1. Blumenthal SR, Swick M, Bayan CA, Ramanathan D, Maher I. Complex eyelid reconstruction: a practical guide for the Mohs surgeon. Dermatol Surg. 2022;48(9):916-23.
2. Archibald LK, Gupta R, Shahwan KT, Swick M, Bakker C, Mattox AR, et al. Periorbital reconstructive techniques following Mohs micrographic surgery or excisions: a systematic review. Arch Dermatol Res. 2023;315(7):1853-61.
3. Bittner GC, Cerci FB, Kubo EM, Tolkachjov SN. Mohs micrographic surgery: a review of indications, technique, outcomes, and considerations. An Bras Dermatol. 2021;96(3):263-77.
4. Scott JF, Bordeaux JS. A conceptual approach to designing transposition flaps. Dermatol Surg. 2020;46(1):9-19.
5. Teske SA, Kersten RC, Devoto MH, Kulwin DR. The modified rhomboid transposition flap in periocular reconstruction. Ophthalmic Plast Reconstr Surg. 1998;14(5):360-6.
6. Harvey DT, Taylor RS, Itani KM, Loewinger RJ. Mohs micrographic surgery of the eyelid: an overview of anatomy, pathophysiology, and reconstruction options. Dermatol Surg. 2013;39(5):673-97.
7. Monheit G, Hrynewycz K. Mohs surgery for periocular tumors. Dermatol Surg. 2019;45 Suppl 2:S70-S8.
8. Sanchez FH, Lerner E. Mohs micrographic surgery in periocular tumors. Surg Cosmet Dermatol 2014;6(4):226-32
9. Yüce S, Demir Z, Selçuk CT, Celebioğlu S. Reconstruction of periorbital region defects: a retrospective study. Ann Maxillofac Surg. 2014;4(1):45-50.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}