


Du Van Truong1; Lam Van Nguyen1; Nam Ky Nguyen2; Luat Thao Huynh3; Mai Huynh Truc Phuong1
Funding source: None.
Conflict of interest: None.
Submission date: 04/28/2024
Final decision:08/28/2024
How to cite this article: Truong DV, Nguyen LM, Nguyen NK, Huynh LT, Phuong MHT. Outcomes of facial skin cancer treatment using local skin flaps at Can Tho City Oncology Hospital from 2021 to 2023. Surg Cosmet Dermatol. 2025;17:e20250368.
BACKGROUND: Reconstructive surgery remains the primary approach for treating facial skin cancer, aiming to restore both anatomy and aesthetics. Local flaps are commonly preferred for facial reconstruction.
OBJECTIVE: To describe the clinical and subclinical characteristics of facial skin cancer and evaluate treatment outcomes using local flaps.
METHODS: A descriptive cross-sectional study with clinical intervention, without a control group, was conducted on 84 patients diagnosed with facial skin cancer and treated at Can Tho City Oncology Hospital from May 2021 to April 2023.
RESULTS: Outcomes were assessed during hospitalization and 6 months postoperatively. Among the 84 patients, 68 had basal cell carcinoma, and 16 had squamous cell carcinoma. The nose was the most frequently treated site, accounting for 43 cases. Lesions smaller than 2 cm comprised 70.2% of cases. After 6 months, 65 out of 84 flap sites (77.4%) exhibited minimal scarring that could be concealed, with an aesthetic success rate of 73.8%.
CONCLUSIONS: Key factors influencing surgical outcomes include the surgeon's experience, lesion location and size, tumor invasion extent, and skin elasticity.
Keywords: Facial Dermatoses; Surgical Flaps; Southeast Asian People.
Skin cancer is typically treated with surgery or chemotherapy, particularly in advanced cases. However, beyond disease management, there is a growing need to address aesthetic concerns. Facial skin cancer not only affects vital anatomical structures but also significantly impacts appearance. Unfortunately, its incidence is rising in many countries.
Surgical correction of facial soft tissue defects presents three main challenges: complete tumor removal to minimize the risk of recurrence, prevention or correction of functional impairments resulting from tumor excision, and reconstruction of the defect to achieve the best possible aesthetic outcome.1 In Vietnam and many other countries, facial skin cancer treatment still involves wide excision followed by reconstruction of the affected area.2
One of the most commonly used methods for facial reconstruction is the local flap technique, which offers several advantages. It provides a well-vascularized tissue source, allows for relatively extensive flap movement, features a long and narrow vascular pedicle compared to traditional skin flaps, and ensures coverage that matches the defect in both tissue thickness and color. Additionally, it enables the concealment of surgical scars within natural skin folds, making it a widely preferred approach in most cases.
At Can Tho City Oncology Hospital, facial skin cancer treatment has been performed since its establishment in October 2007. Most patients present with extensive lesions that significantly impact their appearance, complicating defect reconstruction. Despite a considerable number of hospitalizations for facial skin cancer treatment — 119 cases in 2019 and 125 cases in 2020 — few studies have comprehensively evaluated and monitored reconstruction methods following tumor excision. Therefore, this study was conducted to assess the outcomes of facial skin cancer treatment using the local flap technique.
This was a cross-sectional descriptive study with clinical intervention, without a control group, conducted on a sample of 84 patients. The study was conducted from May 2021 to April 2023 at the Department of Surgery I, Can Tho City Oncology Hospital, Vietnam.
Patients included in the study had a confirmed diagnosis of facial skin cancer through histopathological examination and had surgical defects eligible for reconstruction using local flaps. Only those who provided informed consent were included. Patients diagnosed with sarcoma, lymphoma, or adnexal skin cancer were excluded due to the distinct histopathological characteristics of these neoplasms.
Before surgery, a clinical examination is performed to determine the location and size of the lesion and to review the patient's medical history. Factors influencing the reconstruction process, including aesthetic considerations, skin elasticity, and the involvement of critical anatomical structures, are assessed. The treatment plan is thoroughly explained to the patient. If tumor invasion beneath the skin is suspected, a CT scan is performed, while an MRI is used to evaluate potential bone invasion. Preoperative assessments include routine hematology tests, liver and kidney function tests, blood protein levels, urinalysis, chest X-ray, electrocardiogram, and echocardiography to assess the patient's overall health.
The surgical procedure consists of several steps. The lesion is measured in length and width, and its margins and resection borders are marked with ink. The resection margin for basal cell carcinoma is determined based on lesion size and risk factors: 3–5 mm for small lesions under 2 cm and 7–10 mm for larger or high-risk lesions. For squamous cell carcinoma, the resection margin extends 5–15 mm beyond the visible tumor border, including the erythematous halo. The defect is classified as simple or complex to establish a reconstruction plan, which may involve one or multiple stages. The flap is designed to optimally cover the defect while preserving aesthetic units. During excision, the incision line is aligned with natural skin folds whenever possible. Histological samples are collected from four skin edges, the tumor base, and the tumor itself for pathological analysis.
Postoperative follow-up focuses on assessing skin flap perfusion, wound healing, and early complications until hospital discharge. Evaluations are based on feedback from the surgeon, hospitalist, and patient. Photographic documentation is performed at four time points: before surgery, during the procedure, postoperatively, and at follow-up visits scheduled for 7 days, 1 month, 3 months, and 6 months after surgery. Patient records are maintained, and additional follow-up information is collected through phone calls or in-person consultations.
Surgical outcomes are evaluated in three categories: oncological, functional, and aesthetic. The oncological assessment ensures clear resection margins and monitors for local, regional, or distant recurrence. The functional evaluation examines the surgery's impact on the operated area and adjacent structures, identifying any functional impairments. The aesthetic outcome is categorized into three levels: 1) Good: no asymmetry, no visible signs of plastic surgery, or only minor scarring or asymmetry that does not significantly affect facial appearance; 2) Moderate: noticeable but mild asymmetry or facial distortion that does not severely impact appearance; 3) Poor: significant deformity or scarring that visibly alters the patient's facial appearance.
The study included 84 patients aged 26 to 92 years, with an average age of 66.5 ± 0.2 years. The proportion of female patients was higher than that of male patients, with a female-to-male ratio of 1.4. Most patients resided in rural areas (75%), and 52.4% had occupations involving direct exposure to sunlight.
Histopathological analysis identified basal cell carcinoma in 66 patients and squamous cell carcinoma in 18. The most common tumor location was the nose, affecting 51.2% of patients, followed by the cheek and eye regions (both 15.5%), the lips (14.3%), and the brow (3.5%). Lesions measuring 2 cm or less accounted for 70.2% of cases. The average time from lesion onset to hospital admission was 12 months in 47 out of 84 patients (56%). Most patients (74 out of 84) were diagnosed at clinical stages I or II.
Margin control results showed that among the 66 basal cell carcinoma cases, six had at least one positive margin after excision. However, no recurrence was observed during the six-month follow-up period. In the 18 cases of excised squamous cell carcinoma, all margins were tumor-free, but two cases experienced recurrence.
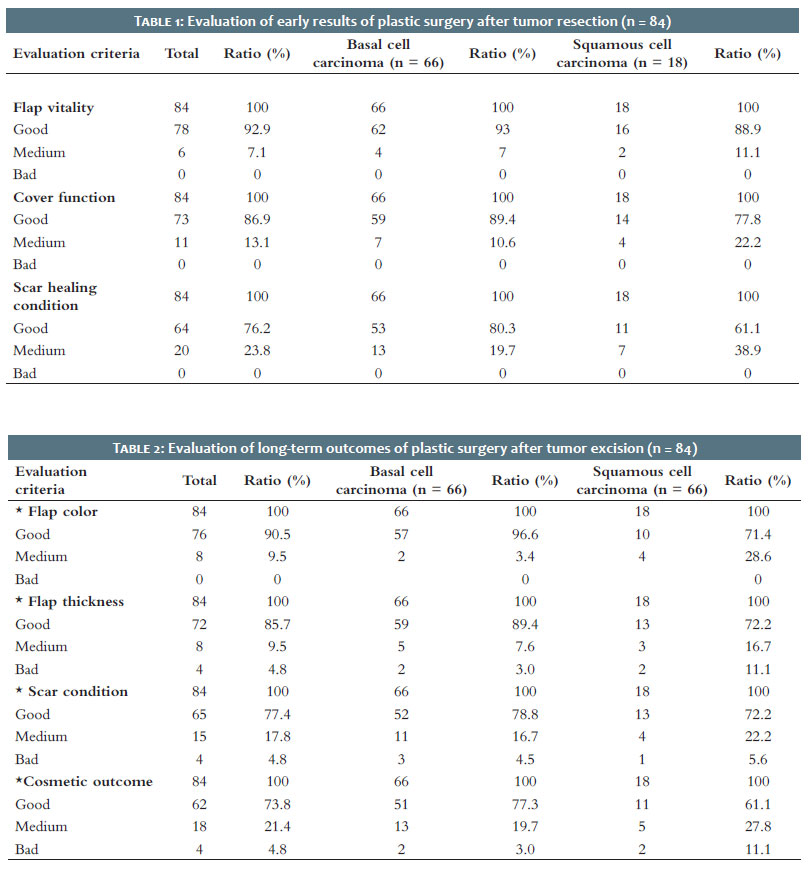
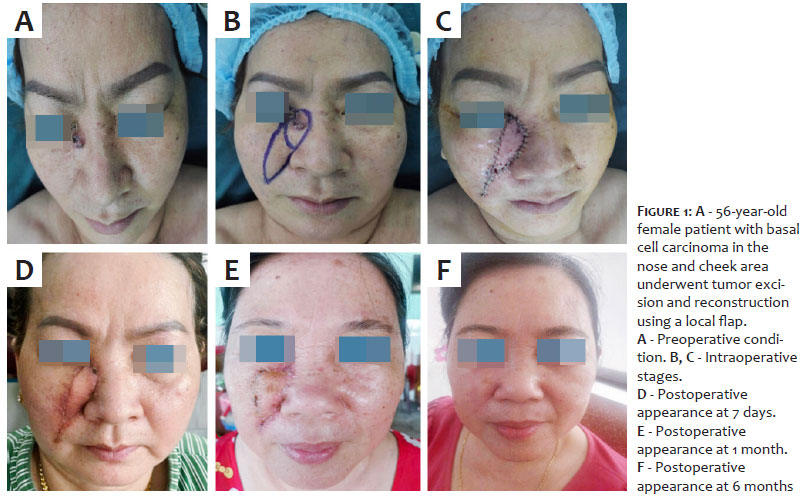
After 6 months of follow-up, the findings were summarized in two tables: one assessing short-term outcomes (1–3 months) and the other evaluating long-term results (3–6 months). A tumor resection algorithm was then developed based on these findings (Figure 1).
Among the 84 cases of facial skin cancer studied, 66 were basal cell carcinoma, and 18 were squamous cell carcinoma. The study population included 36 male patients (42.9%) and 48 female patients (57.1%). Patients ranged in age from 26 to 92 years, with an average age of 66.5 ± 0.2 years. Previous studies reported similar findings, with Trinh Hung Manh documenting an average age of 64.92 ± 0.1 years and Duong Manh Chien reporting an average of 68 ± 13.1 years.1,3 These findings suggest that facial skin cancer is more common in older individuals, with incidence rates increasing progressively with age.
The female-to-male ratio in this study was 34:50, with a higher number of women. This may be explained by men being less likely to examine their skin and use sunscreen, whereas women are more inclined to seek dermatological evaluation at the first sign of a skin lesion. As a result, potentially malignant tumors are detected earlier in women. Studies suggest women are generally more proactive in protecting their skin from sun exposure, which may help reduce the harmful effects of UV radiation.10
The study also found that 78.6% of patients lived in rural areas, with most working in agriculture and experiencing prolonged sun exposure. The proportion of individuals working outdoors was 52.4%, lower than the 80.9% reported in research by Trinh Hung Manh.3 Sun exposure remains a primary risk factor for UTD, with outdoor workers exhibiting a higher prevalence of the disease. According to David C. Whiteman, an Australian study found individuals with outdoor occupations had a 5.5 times higher risk of developing skin cancer compared to indoor workers, and light skin tone increased this risk up to 10.5 times.11 This increased susceptibility may be due to prolonged exposure to risk factors and compromised immune defense. Additionally, the study highlights that many patients may lack awareness about basal and squamous cell carcinoma or experience delays in diagnosis and treatment due to reliance on traditional medicine or initial misdiagnosis as fungal or inflammatory conditions. Similar findings were reported by Doan Huu Nghi and the Communist Party, where the incidence rate reached 68%.4
Basal cell carcinoma accounted for 78.6% of cases, while squamous cell carcinoma made up 21.4%. These proportions align with findings from research by Trinh Hung Manh.3 Among the 66 basal cell carcinoma cases, six had positive resection margins, yet no recurrences were recorded during the 6-month follow-up. This could be attributed to the typically slow progression of basal cell carcinoma. However, previous research indicates recurrence rates tend to rise over time, particularly within the first 2 years after surgery, and can continue to increase between 2 and 5 years postoperatively. In research by Trinh Hung Manh, the average time between initial surgery and recurrence was 25 months, ranging from as early as 3 months to as late as 51.1 months.
Regarding surgical margins, 78.1% of cases had a resection margin of 5–10 mm from the tumor. The standard margin for basal cell carcinoma is typically 5–10 mm. In two cases of squamous cell carcinoma, the surgical margin was less than 5 mm due to tumor proximity to critical structures, such as eyelid cartilage, where wider excision was not feasible. Among the 18 squamous cell carcinoma cases, two experienced recurrences despite negative surgical margins. One recurrence occurred in a patient with a 4 × 6 cm lesion on the cheek, classified as grade 2 aggressive squamous cell carcinoma, who experienced local recurrence 3 months after surgery.
Facial tumors are relatively easy to detect early, given their visibility. In this study, 54.8% of patients presented with tumors smaller than 5 cm. Tumor staging was determined based on tumor size (T) and lymph node involvement (N), considering the degree of tissue infiltration and clinical findings. Most cases were classified as T1 (54.8%), followed by T2 (34.2%) and T4 (11%).
Tumors measuring ≤2 cm accounted for 70.2% of cases, with male patients tending to present with larger tumors than females. Trinh Hung Manh reported 63.7% of cases had lesions <2 cm,3 while Bach Quang Tuyen found a slightly lower proportion (53.12%).12 The nose was the most frequently affected site, accounting for 51.2% of cases. Of these, 62.8% affected the nasal alae. Other common tumor sites included the cheeks and eye area (15.5% each), lips (14.3%), and forehead (3.5%). A study by Janjua OS et al. reported a similar trend, with nasal tumors comprising 31.5% of cases, followed by cheek lesions at 26.9%.5
The predominance of nasal tumors can be attributed to the nose's central location on the face, where it plays a crucial role in both function and aesthetics. Its prominence makes deformities highly noticeable, affecting not only physical appearance but also psychological well-being. Restoring nasal contour is essential for maintaining facial symmetry and quality of life.6
In skin cancer, tumor invasion depth is often more significant than tumor size in determining surgical complexity and recurrence risk. The choice of reconstruction technique depends largely on the extent of invasion. Local flaps are generally recommended for small to medium-sized lesions, especially those involving the eyelids and nasal wings, where preserving function and aesthetics is critical.7 The most common sites of recurrence include the medial canthus, philtrum, nasolabial fold, and preauricular and postauricular regions.
More than half of the basal and squamous cell carcinoma cases in this study measured ≤2 cm (76.7%), followed by tumors between 2–5 cm (12.3%) and >5 cm (11%). The higher proportion of small tumors compared to previous studies may reflect improvements in early detection and healthcare accessibility. When comparing defect size to flap viability, lesions ≤5 cm had a 92.3% success rate, while those >5 cm had an 87.5% success rate. Studies by Duong Manh Chien and Bui Xuan Truong found no significant difference between defect size and flap survival.8 However, tumor invasion depth did impact flap viability. Simple skin invasion cases had a flap survival rate of 91.8%, whereas those involving cartilage and periosteum had a slightly lower rate of 80%. Deeper tumor invasion, particularly into structures such as the orbicularis oculi muscle, increases the likelihood of recurrence and necessitates more complex reconstructive approaches.
One month postoperatively, scars appeared dark brown, slightly raised, and caused mild tissue retraction. By three months, scars had faded to white, and surrounding tissue gradually returned to normal. At six months, 90.5% of skin flaps had color matching the surrounding tissue, 85.7% had thickness comparable to adjacent skin, and 77.4% of scars (65 out of 84 cases) were minimal. Overall aesthetic success rate was 73.8%.
In a study by Nguyen Quang Ruc, 6-month follow-up results showed 73.1% of patients had good outcomes, 26.9% had good outcomes, and no cases were classified as bad.9
Local flaps are an effective treatment option for facial skin cancer reconstruction. After six months, surgical outcomes showed minimal and inconspicuous scarring in 77.4% of cases, with an overall aesthetic success rate of 73.8%, meeting both surgeon and patient expectations. The surgeon's expertise in designing flaps that appropriately match the location and size of the defect plays a crucial role in surgical success.
Further follow-up is necessary to fully assess the long-term effectiveness of the treatment. For future studies, we recommend the use of frozen section analysis in cases where distinguishing between tumor and healthy tissue is challenging, particularly in high-risk recurrence areas.
Du Van Truong
Statistical analysis, Approval of the final manuscript version, Study conception and design, Manuscript drafting and writing, Data collection, analysis, and interpretation, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of studied cases, Critical literature review, Critical manuscript review
Lam Van Nguyen
ORCID: 0000-0001-5970-0528
Statistical analysis, Approval of the final version of the manuscript, Study conception and design, Manuscript drafting and writing, Data collection, analysis, and interpretation, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of studied cases, Critical literature review, Critical manuscript review
Nam Ky Nguyen
Statistical analysis, Study conception and design, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of studied cases, Critical literature review, Critical manuscript review
Luat Thao Huynh
Approval of the final version of the manuscript, Study conception and design, Data collection, analysis, and interpretation, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of studied cases, Critical manuscript review
Mai Huynh Truc Phuong
Approval of the final version of the manuscript
1. Chien DM, Anh DH. Evaluating the results of local flap reconstruction after excision of basal cell skin cancer in the cheek area. J Med Res. 2022;155(7):67-74.
2. NCCN Guidelines for patients. Basal cell and squamous cell skin cancers. 2022.
3. Manh TH. Research on clinical and histopathological characteristics and evaluate surgical results of treatment of squamous cell carcinoma, basal cell carcinoma of the skin of the head, face and neck area. Res Clin Med Pharm. 2016: 108.
4. Nghi DH. Skin cancer. Oncology. 2001: 223-9.
5. Janjua OS, Qureshi SM. Basal cell carcinoma of the head and neck region: an analysis of 171 cases. J Skin Cancer. 2012:943472:1-4.
6. Manh NT, Lam VN, Tuan LD. Evaluation of clinical characteristics of nasal soft tissue defects surgically treated with forehead skin flaps. Viet Med J. 2022;511(2).
7. Cass ND, Terella AM. Reconstruction of the cheek. Facial Plast Surg Clin N Am.2019;27(1):55-66.
8. Truong BX. Research on wide excision - plastic surgery to treat facial skin cancer
9. [Doctor of Medicine Thesis] Ho Chi Minh City University of Medicine and Pharmacy. 2011.
10. 9. Ruc NQ. Evaluating the results of surgery to reconstruct small and medium soft tissue defects after resection of facial basal cell cancer [Master's thesis in Medicine]. Ha Noi Medical University. 2019.
11. 10. Tuan NAH, Hai VV, Thuong NHC, Dieu DP. Correlation between anthropometric indices of the nasal bone area on adult vietnamese bodies. Viet Med J. 2021;503(1):40.
12. 11. Whiteman DC, Olsen CM, MacGregor S, Law MH, Thompson B, Dusingize JC, et al. The effect of screening on melanoma incidence and biopsy rates. Brit J Dermatol. 2022;187(4):515-522.
13. 12. Tuyen QB, Tho HN, Duc QN. Using local tissue in the treatment of head, face and neck skin cancer. Clin Med. 2009;108(2):102-107.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}