


Renato Roberto Liberato Rostey1; Cristiane Ferreira Rallo de Almeida1; Danilo Olavarria D'Aquino2; Caio Leal Carvalho1
Financial support: None.
Conflicts of interest: None.
Submission on: 03/29/2024.
Approved on: 08/15/2024.
How to cite this article: Rostey RRL, Almeida CFR, D'Aquino DO, Carvalho CL. Treatment of Parry-Romberg syndrome and linear scleroderma en coup de sabre, with application of poly-L-lactic acid (PLLA): assessment of clinical and high-resolution ultrasound response. Surg Cosmet Dermatol. 2025;17:e20250361.
INTRODUCTION: Parry-Romberg syndrome and linear scleroderma en coup de sabre are disorders within the scleroderma spectrum, a disease that presents therapeutic challenges.
OBJECTIVES: We treated three patients with this condition using poly-L-lactic acid (PLLA) with the aim of alleviating facial asymmetries and evaluated the real improvement of scleroderma lesions with high-resolution ultrasound.
METHODS: The patients underwent two to four sessions of biostimulation with PLLA over a 12-month period.
RESULTS: The results were promising, demonstrating favorable cosmetic outcomes with increased thickness of the dermis and hypodermis as evidenced by high-resolution ultrasound.
CONCLUSIONS: Biostimulation with PLLA is a safe and effective treatment option for these patients when administered by trained professionals.
Keywords: Facial Hemiatrophy; Scleroderma, Localized; Dermal Fillers; Ultrasonography.
Parry-Romberg syndrome (PRS) is a rare craniofacial disorder characterized by hemifacial atrophy of the skin, subcutaneous tissue, fat and, in severe cases, underlying muscles, bones, and cartilage.1,2 It is considered a specific form of cutaneous scleroderma.3 Usually onset is observed in the first 20 years of life, although cases of late onset have been described.1 Symptoms progress over 2 to 10 years, a self-limiting period before spontaneous stabilization.4-6 Systemic manifestations of the disease, including dermatological, bone, muscle, ophthalmological, neurological, cardiac, endocrinological, maxillofacial, orthodontic, and oral manifestations can occur.2,7 Histopathology shows atrophy of the subcutaneous fat, reduction of adnexal structures, and mononuclear cell infiltrate.2,8
Linear scleroderma en coup de sabre (LSCS) is a presentation of localized scleroderma, so called because it causes a lesion similar to a saber blow that affects the head.9 It is characterized by a linear cutaneous sclerotic lesion, may be hyperpigmented, and is also accompanied by cranial atrophy, neurological alterations, and seizures.9 Histopathology shows sclerosis of the skin and underlying tissues due to excess collagen deposition, adnexal atrophy, mononuclear cell infiltrate, and perineural inflammation.8
Both PRS and LSCS are more common in women and usually occur before they are 15 years old. Many common characteristics are observed in both diseases, with some authors considering them spectra of scleroderma and others considering them to be the same disease.8 The main differences between the two are no scarring alopecia and sclerosis of the skin in PRS,2 and sclerosis of the skin and scalp with hyperpigmentation and alopecia of the scalp and eyebrows in LSCS.2 Patients can present distinct characteristics of one or the other disease, or even both.10
Treatments to improve the appearance of the atrophy caused by these diseases are commonly attempted, the most common being autologous fat transplantation and fat flap grafts.11 Whenever possible, aesthetic treatment of autoimmune diseases should be attempted, as these are diseases that have a significant impact on patients' psychological state and quality of life.12 Treatments with autologous fat grafting, autologous fat transplantation, hyaluronic acid, poly-L-lactic acid (PLLA), calcium hydroxyapatite, polymethylmethacrylate, lasers, and bone and cartilage grafts have been described.12
The use of PLLA for the treatment of LSCS and PRS was described in 2009.13 Recently, a case of PRS treatment with hyaluronic acid and PLLA has been described.14 A case series demonstrated the use of PLLA in a patient with systemic scleroderma, in one with CREST syndrome, and in another with lupus panniculitis.15 Biostimulation is the ability of a polymer to generate cellular benefit or tissue response in a particular clinical application, by means of a desired controlled inflammatory response, which leads to the slow degradation of the material and culminates in the deposition of collagen in the tissue, conditioned by the properties of the biomaterial, the characteristics of the patient, and the technique used to inject the polymer into the tissue.16
PLLA is a resorbable, biodegradable, biocompatible substance that stimulates the formation of new collagen fibers, which has proven to be safe and has the ability to restore volumetric defects. There are reports in the literature of patients who have been treated with biostimulants and hyaluronic acid fillers with a satisfactory response. Soft tissue augmentation with injectable fillers is a minimally invasive technique that replaces lost facial volume.17 High-resolution ultrasound (HRUS) is already used in dermatology to assess dermal fillers,18 evaluate results19 and complications.20 It is also used for clinical and diagnosis assessment of localized cutaneous scleroderma21 and PRS.22
This study aimed to evaluate and prove that the application of PLLA can improve the clinical aspect and volumetric loss, correct asymmetries, improve the general quality of the affected skin and the aesthetic aspect of skin lesions in patients affected by PRS and LSCS. HRUS measured the thickness of the dermis/hypodermis before and after the procedure, and provided an objective assessment of the response.
This is a clinical trial with a convenience sample of patients from the dermatology outpatient clinic located in Outpatient Clinic III of the Hospital Universitário Júlio Muller, Brazil. This study was submitted to the Research Ethics Committee of and approved under protocol number CAAE 57003722.0.0000.554 on July 28, 2022.
Eligible participants were all adult patients who routinely came to the dermatology outpatient clinic with a diagnosis of localized cutaneous scleroderma, including PRS/LSCS, and who had a stabilized condition. The study included three patients aged 18 years or over who met the criteria for PRS/LSCS confirmed by clinical examination, who did not meet any exclusion criteria and who agreed to participate in the study voluntarily, without any burden on their treatment or gratuities. Exclusion criteria: active disease; infection in the treated area; a history of procedures with fillers; clinical conditions that prevented the technique from being performed (full immunosuppression, blood dyscrasias); and the patient not agreeing to be treated with this therapeutic option.
The patients underwent a clinical examination, a photographic record, a previous HRUS examination of the area to be treated and also of an adjacent area not affected by the disease. All patients provided written informed consent. The thickness of the affected skin obtained by HRUS was compared with the thickness of healthy skin adjacent to the affected area. The product was prepared immediately before the procedures. Each vial of PLLA (Sculptra®) was diluted in 1:8 mL of distilled water, reconstituted by shaking vigorously for 1 minute, aspirated into 5 mL syringes with a further 1 mL of lidocaine without vasoconstrictor in each syringe. The procedure was performed using a small anesthetic button with 0.3 mL of lidocaine with vasoconstrictor, through which the product was inserted and applied using a 22 x 70 mm cannula, in the subdermal plane as close to the skin as possible (Figure 01).
Prior to the following sessions, new photographic and HRUS recordings were made, which were repeated after the last session. The intervals between sessions and HRUS are shown in the respective tables for each patient. This study measured the dermis and hypodermis of the regions without disease and those affected both before and after the injection of PLLA, using a high-resolution dermatological linear transducer of up to 22 MHz (GE Logic and Pro - GE Medical System). The patients received different doses of PLLA, depending on their individual response and the need to correct the asymmetry. The sessions ranged from two to four vials, and intervals lasting 8 to 24 weeks.
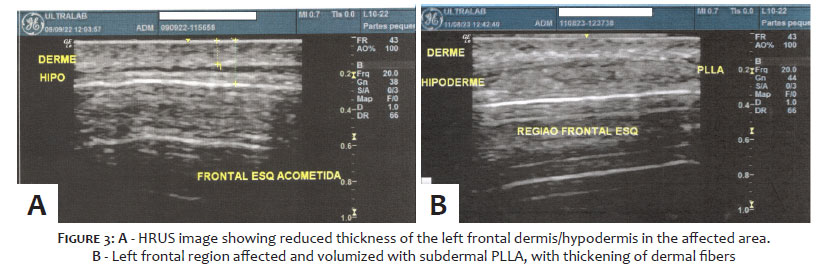
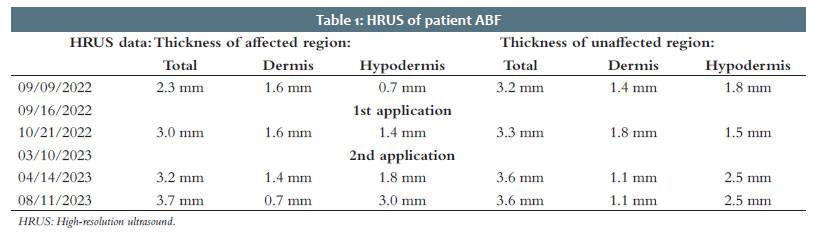
The 26-year-old patient, ABF, was the patient with the smallest affected area, and also the one with the shortest disease progression time (3 years) at the beginning of treatment. She had only undergone topical treatments due to the condition, having used tacrolimus and calcipotriol. She had an atrophic area on her left forehead, madarosis of the tail of the eyebrow and homolateral cilia, and slightly hardened skin. This was compatible with LSCS. She also had congenital bilateral eyelid ptosis, resulting in an improvement in the homolateral eye opening as a result of the retraction caused by the disease, which can be clearly seen in the initial photo (Figure 02).
About 1 month after the first application, skin thickness increased by approximately 30% compared to baseline thickness. Finally, 5 months after the second application, skin thickness increased by approximately 61% compared to baseline thickness (Figure 03 and Table 01).
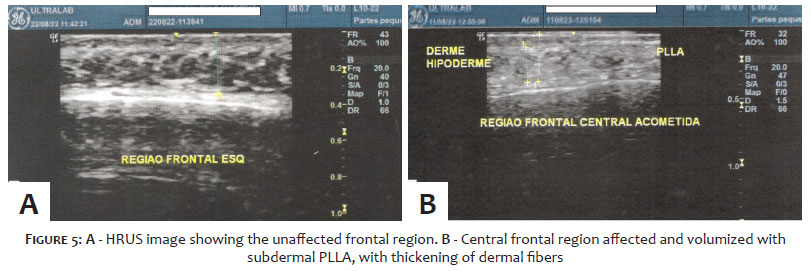
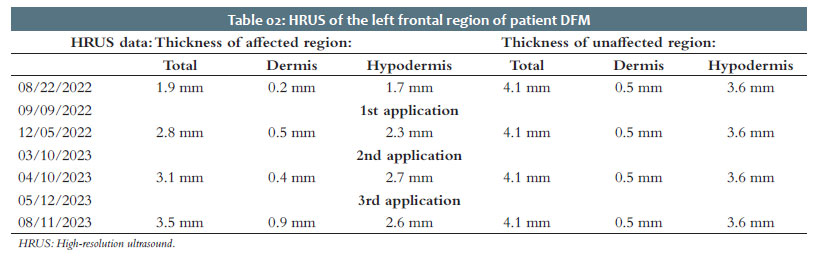
The 27-year-old patient, DFM, presented with alopecia in the left frontoparietal region at the age of 10, followed by the appearance of an atrophic and hardened plaque on the forehead at the beginning of treatment. Initially, she was treated with topical hydrocortisone for around 5 years. The clinical picture is characteristic of LSCS (Figure 04).
In the left frontal region, about 3 months after the first application, skin thickness increased by approximately 47% compared to baseline thickness. And 7 months after the first application, skin thickness increased by approximately 63% compared to baseline thickness. Then, 11 months after the first application, skin thickness had increased by around 84% compared to baseline thickness (Figure 05 and Table 02).
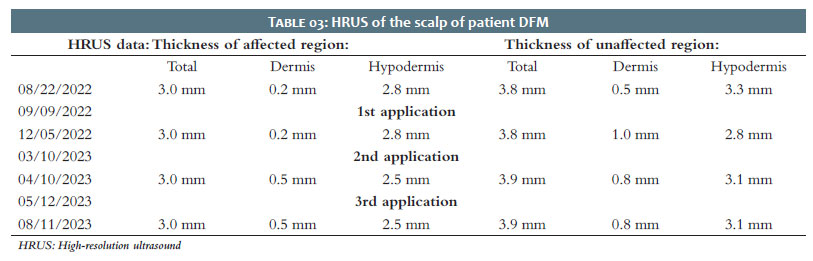
HRUS found no increase in skin thickness in the scalp area. However, an increase in skin firmness and distension was observed, promoting a noticeable visual improvement, both by the examiners and the patient (Table 03).
The 28-year-old patient, DCL, had the largest area of involvement at the start of treatment, with a lesion on practically the entire left hemiface. No hardening of the skin was present, which is typical of PRS. She was the only patient who had already been treated systemically for the disease, with corticosteroid therapy in addition to topical tacrolimus. Magnetic resonance imaging showed no bone or brain involvement. As this was the largest area affected, in each session 1 vial of PLLA was divided unevenly between the two main areas (Figure 06).
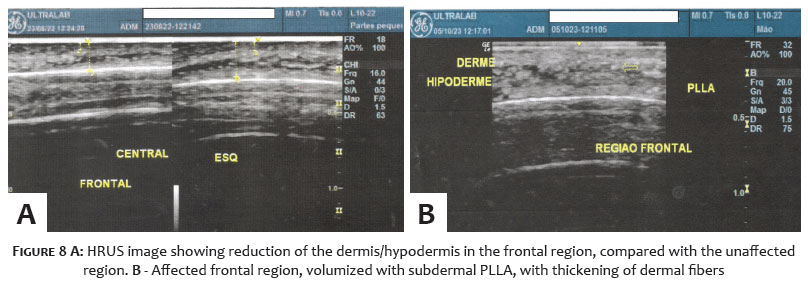
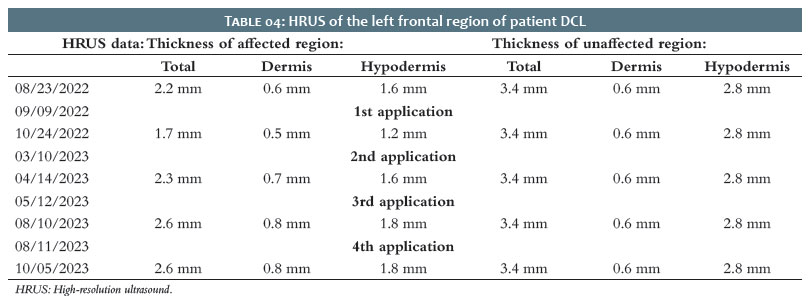
In the left frontal region, a 23% thickness improvement in relation to baseline thickness was seen about 1 month after the first application. We attribute this change to the variation in the measurement site, as clinically it has improved. Following the second application, 7 months after the first, there was an increase of approximately 5% in skin thickness compared to baseline thickness. And 11 months after the first, skin thickness increased by around 18% compared to baseline thickness. Following the fourth application, 13 months after the first application, this 18% increase was maintained (Figure 07, 08 and Table 04).
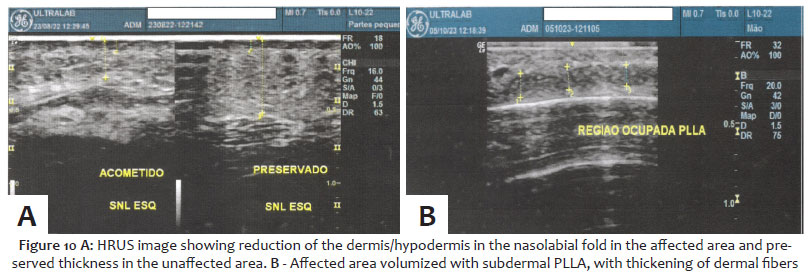
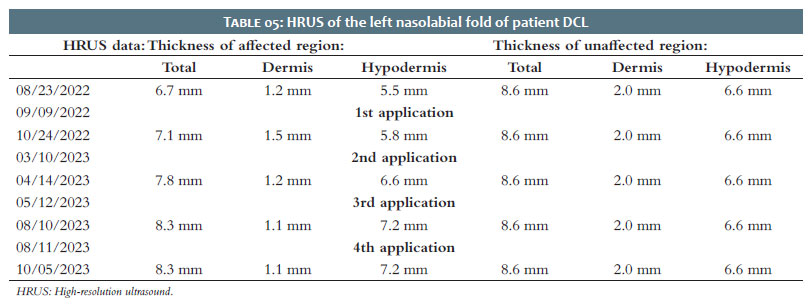
Nearly 1 month after the first application, in the region of the left nasolabial fold, skin thickness increased by around 6% compared to baseline thickness. The second application, 7 months after the first, showed an increase of approximately 16% in skin thickness compared to baseline thickness. Eleven months after the first application, skin thickness increased by around 24% compared to the initial application. Following the fourth application, 13 months after the first, this 24% increase was maintained (Figure 09, 10 and Table 05).
Various techniques have been described for treating the atrophies caused by PRS and LSCS and other forms of scleroderma. In this clinical trial, the use of PLLA was chosen for its ability to restore lost volume and stimulate gradual collagen deposition, with the aim of alleviating facial asymmetry.12-15 Although PLLA offers advantages, there are challenges associated with its use in PRS and LSCS.13,14 The main challenge is the time needed to obtain visible results, since collagen production is a gradual process. In addition, the variability in response to treatment can be a limiting factor, with some patients not achieving the desired result. We would also point out that the patients in the study were young, and therefore had preserved ability of the resident cells of the extracellular matrix to synthesize collagen and respond better to treatment with biostimulators. The use of Sculptra® is generally well tolerated, with rare and usually mild adverse effects. The most common side effects include edema, bruising, and tenderness in the treated area. More serious complications, such as infections or granulomas, are rare, but should be closely monitored.13,17
HRUS allows us to add a lot of information in dermatology and injectables, helping with increasingly accurate diagnoses and more assertive surgical and injectable planning. In the case of cutaneous scleroderma, HRUS can provide the attending physician with information on the activity or absence of activity of the disease by assessing the hyperechogenic halo around the vessels in the skin. It also allows for a good separation of the layers of the skin and, in this case in particular, allows for the visualization and measurement of the loss of volume and which layer of the skin has been affected, as well as allowing for the visualization of PLLA, the injected skin plane, and its biostimulus, which is validated by repeated measurement and thickening of the layers of the skin in the affected regions.23-25
Thickness analyses with HRUS can vary according to the experience of the operator, the method being operator-dependent, as well as the sites measured. As no specific marking was made on the skin, as would be the case with a tattoo, there were slight changes in the sites measured at each assessment. This justifies small variations in the thicknesses measured during the evolution of the assessments, though it did not compromise the assessment, as the gain in thickness could be proven by analyzing all the tests performed. The evolution of ultrasound transducers with increasingly higher frequencies has allowed for a more detailed study of the skin and appendages. HRUS has become an important tool for dermatologists and injectors, helping to visualize structures dynamically and in real time. The various types of cosmetic fillers, autologous materials (autologous fat), and biostimulators can be identified and differentiated using dermatological HRUS and a professional ultrasound surgeon trained in the field.18,19,26
In the series of photographs, volumization of the treated area can be seen, which is corroborated by the final gain in skin thickness obtained by HRUS measurements. Both the dermis and the hypodermis showed increased thickness; however, the hypodermis showed a greater gain in thickness compared to the dermis, which can be explained by the collagen cross-linking mechanism that occurs over the months, which causes it to contract and adjust its network. The presence of fibroblasts in the hypodermis also enables the mechanisms of neocollagenesis in this area with the gradual deposition of collagen fibers.
The use of PLLA collagen biostimulator (Sculptra®) has proven to be a safe and feasible method for treating volume loss and asymmetries resulting from PRS and LSCS. Volume replacement, improved skin quality, improved symmetry, and consequent aesthetic improvement lead to improved quality of life for these patients. Proper patient selection, the amount of product to be used, which should always be individualized, and a well-trained professional injector are all important factors in the success of the treatment.
Renato Roberto Liberato Rostey
ORCID: 0000-0001-8656-4111
Statistical analysis, approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, data collection, analysis, and interpretation, effective participation in research guidance, intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, critical literature review, critical review of the manuscript.
Cristiane Ferreira Rallo de Almeida
ORCID: 0000-0002-8525-344X
Approval of the final version of the manuscript, study design and planning, preparation and writing of the manuscript, critical literature review, critical review of the manuscript.
Danilo Olavarria D'Aquino 0009-0002-3767-591X
Data collection, analysis, and interpretation, intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, critical review of the manuscript.
Caio Leal Carvalho 0009-0005-7919-7188
Data collection, analysis, and interpretation, intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Schultz KP, Dong, E, Truong TA, Maricevich RS. Parry romberg syndrome. Clin Plast Surg. 2019;46(2):231-237.
2. Shah SS, Chhabra M. Parry-romberg syndrome [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK574506/
3. De la Torre IG, Castello-Sendra J, Esgleyes- Ribot T, Martinez-Bonilla G, Guerrerosantos J, Fritzler MJ. Autoantibodies in parry romberg syndrome: a serologic study of 14 patients. J Rheumatol. 1995;22(1):73–7.
4. Buonaccorsi S, Leonardi A, Covelli E, Indrizzi E, Perdicchi A, Fini G. Parry-romberg syndrome. J Craniofac Surg. 2005;16(6):1132–5.
5. El-Kehdy J, Abbas O, Rubeiz N. A review of parry-romberg syndrome. J Am Acad Dermatol 2012; 67:769–84.
6. Tolkachjov SN, Patel NG, Tollefson MM. Progressive hemifacial atrophy: a review. Orphanet J Rare Dis. 2015;10:39.
7. Bucher F, Fricke J, Neugebauer A, Cursiefen C, Heindl LM. Ophthalmological manifestations of parry- romberg syndrome. Surv Ophthalmol 2016;61:693–701.
8. Khamaganova I. Progressive hemifacial atrophy and linear scleroderma en coup de sabre: a spectrum of the same disease? Front Med.2018;4:258.
9. Martins MV, Azevedo I, Rodrigues C, Oliveira M. Linear scleroderma en coup de sabre – a different clinical presentation. acta reumatol port. 2021;46:72-76.
10. Tollefson MM, Witman PM. En coup de sabre morphea and parry-romberg syndrome: a retrospective review of 54 patients. J Am Acad dermatol. 2007;56(2):257-263.
11. Glaser DH, Schutt C, Schollaert-Fitch K, Torok K. Linear scleroderma of the head - updates in management of parry romberg syndrome and en coup de sabre: a rapid scoping review across subspecialties. Eur J Rheumatol 2020;7(Suppl 1): S48-S57.
12. Creadore A, Watchmaker J, Maymone MBC, Pappas L, Lam C, Vashi NA. Cosmetic treatment in patients with autoimmune connective tissue diseases. J Am Acad Dermatol. 2020;83(2):315–41.
13. Onesti MG, Troccola A, Scuderi N. Volumetric correction using poly-L-lactic acid in facial asymmetry: parry romberg syndrome and scleroderma. Dermatol Surg. 2009;35(9):1368-1375.
14. Ha D ‐L, Oh C ‐K, Kim M ‐B. Parry–romberg syndrome treated with injectable poly‐L‐ lactic acid and hyaluronic acid filler: a case report. J Eur Acad Dermatol Venereol. 2020.27;34(6).
15. Pamatmat JJ, Gonzalez CD, Euwer R, Summers E, Smart D, Goff HW. Novel use of poly‐L‐lactic acid filler for the treatment of facial cutaneous atrophy in patients with connective tissue disease. J Cosmet Dermatol. 2021;00:1–5.
16. Griffith LG. Polymeric biomaterials. Acta Materialia. 2000;48(1):263-77.
17. Cunha MG, Engracia M, Souza LG, Machado Filho CD. Bioestimuladores e seus mecanismos de ação. Surg Cosmet Dermatol. 2020;12(2).
18. Schelke LW, Van-Den-Elzen HJ, Erkamp PPM, Neumann HAM. Use of ultrasound to provide overall information on facial fillers and surrounding tissue. Dermatol Surg 2010;36:1843–1851.
19. Wortsman X,Wortsman J, Orlandi C, Cardenas G, Sazunic I, Jemec GBE. Ultrasound detection and identification of cosmetic fillers in the skin. J Eur Acad Dermatol Venerol.2012;26:292–301.
20. Wortsman X. Identification and complications of cosmetic fillers. J Ultrasound Med 2015;34:1163–1172.
21. Bouer M, Chammas MC, Messina MCL, Oliveira IRS, Cerri GG. Correlação clínica e ultra-sonográfica na esclerodermia localizada cutânea. Radiol Bras. 2008;41(2):87–91
22. Quintana-Castanedo L, Sánchez-Orta A, Nuno-Gonzalez A, Herranz-Pinto P. Usefulness of cutaneous ultrasound in the management of parry romberg syndrome. Skin Res Technol. 2021;00:1–2.
23. Sigrist R, Noronha G, Quezada N, Wortsman X. Ultrasonographic pattern of poly-L- lactic acid at high-frequency and ultrahigh-frequency. Dermatol Surg. 2024;50(8):783-785.
24. Habib P, Roddy J, Ch'ng S, Chowalloor P, Keen H. The role of ultrasound in scleroderma skin disease. Tasman Med J. 2021;3(1):2652-1881.
25. Dźwigała M, Sobolewski P, Maślińska M, Yurtsever I, Szymanska E, Walecka I. High-resolution ultrasound imaging of skin involvement in systemic sclerosis: a systematic review. Rheumatol Int. 2021;41:285–295.
26. Fontan C, Cardoso D, Rezende JP, Zattar LC, Mota A. Avaliação ultrasonográfica dos preenchedores e bioestimuladores em diferentes aparelhos de ultrassonografia e com diferentes frequências. JODI. 2023;1:e2023004.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}