


Marcelo Balbinot Lucca1,2; Laura Oliveira Ferreira1; Ana Letícia Boff3; Rodrigo Vettorato1,3
Funding source: None.
Conflict of interest: None.
Submission date: 06/20/2024
Final decision: 06/21/2024
How to cite this article: Lucca MB, Ferreira LO, Boff AL, Vettorato R. Bilateral temporal triangle alopecia mimicking male pattern alopecia in an adult woman: a case report and review of literature. Surg Cosmet Dermatol. 2025;17:e20250380.
INTRODUCTION: Temporal triangular alopecia (TTA) is a nonscarring, noninflammatory, permanent form of alopecia with an unknown etiology, often misdiagnosed as other types of alopecia.
CASE REPORT: A 27-year-old woman presented with triangular patches of alopecia in the temporal regions, resembling male pattern alopecia. Dermoscopy revealed normal follicular openings. Histopathological analysis showed only vellus follicles, with no telogen or terminal follicles, intact sebaceous glands, and no inflammatory infiltrate.
DISCUSSION: Dermoscopy is a valuable diagnostic tool, and histopathology may be performed in selected cases. There is no definitive treatment for TTA. Management options include topical minoxidil, hair transplantation, or surgical excision.
Keywords: Alopecia; Temporal Distribution; Hair Diseases.
Temporal triangular alopecia (TTA) is an asymptomatic, localized, nonscarring, and noninflammatory form of permanent alopecia with an unknown etiology. Although considered uncommon, it is frequently underdiagnosed.1
Typically appearing in childhood, TTA presents as a triangular, rounded, or spear-shaped alopecic patch—often singular—in the frontotemporal region, remaining stable throughout life. Dermoscopy and histopathology are valuable tools for differentiating TTA from other types of alopecia, such as alopecia areata, trichotillomania, traction alopecia, and congenital aplasia cutis.2,3
In this report, we present a rare case of bilateral TTA mimicking male pattern alopecia in an adult woman and discuss key considerations for its identification.
A 27-year-old Caucasian female presented to our dermatology practice with a long-standing history of hair thinning in the bilateral temporal region, which began at age 7. The condition remained stable over time, with no notable changes or progression, and no involvement of other scalp areas.
Previous investigations1 had suggested a possible diagnosis of trichotillomania, despite the patient denying any hair-plucking behavior. She reported no itching, pain, or other associated symptoms. She was in good health and had been continuously using oral contraceptives, with no other ongoing medications.
Dermatological examination revealed two triangular-shaped alopecia plaques in the temporal regions, each measuring approximately 8 cm in diameter (Figure 1). These plaques contained vellus hairs at the center, surrounded by terminal hairs at the periphery, resembling Hamilton-Norwood type II male pattern alopecia. No erythema or scaling was observed.
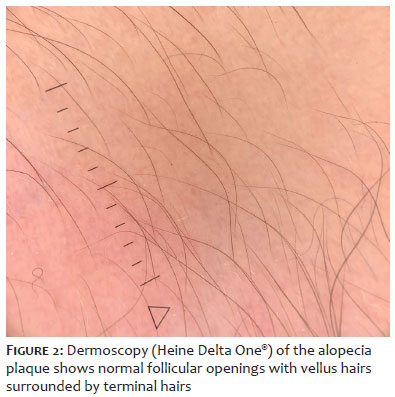
Dermoscopy (Heine Delta One®) revealed normal follicular openings with vellus hairs surrounded by terminal hairs (Figure 2). There were no signs of yellow or black dots, dystrophic hairs, vascular changes, or decreased follicular openings. The pull test was negative.
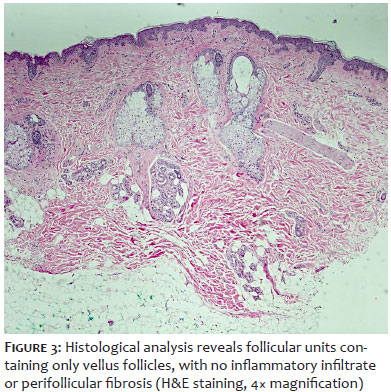
A skin biopsy was performed on one of the plaques. Histological analysis showed only vellus follicles, with no telogen or terminal follicles in the alopecic area. Sebaceous glands were intact, and there was no inflammatory infiltrate. A single terminal follicle was present at the periphery (Figure 3). These findings, combined with clinical assessment, confirmed a diagnosis of TTA.
The patient expressed relief at finally receiving a definitive diagnosis after years of uncertainty. We discussed her prognosis and the limited therapeutic options with proven efficacy. As a strategy to improve hair density and thickness, oral minoxidil (0.5 mg/day) was prescribed. The patient was satisfied with the diagnostic clarification and agreed to the treatment plan.
TTA was first described by Sabouraud in 1905 as "congenital triangular alopecia," a term now considered obsolete, as many cases emerge between ages two and nine, while some may present or be diagnosed in adulthood.1,4 In the present case, despite the late diagnosis, the onset at age 7 with no subsequent progression was a key factor in confirming the diagnosis.
The etiology of TTA remains unknown. While typically sporadic, familial cases suggest an autosomal dominant inheritance pattern.1,4 It has also been associated with mosaicism and linked to conditions such as Down syndrome, iris nevus, pigmentovascular phakomatosis, congenital heart diseases, bone and dental abnormalities, intellectual disability, and aplasia cutis congenita.1,5,6
Although considered rare, with an incidence of 0.11%4 and fewer than 200 reported cases, TTA is believed to be underdiagnosed and often mistaken for other forms of alopecia, particularly alopecia areata. TTA is more prevalent in Caucasians and affects both sexes, although men are more frequently affected. In over 95% of cases, TTA occurs in the frontotemporal region, with bilateral involvement, as seen in our case, being less common (18.5% of cases).2
Dermoscopy plays a critical role in distinguishing TTA from other types of alopecia. Inui et al. proposed the following diagnostic criteria3: 1) triangular or spear-shaped alopecia plaque involving the frontotemporal region; 2) dermoscopy showing normal follicular openings with vellus hairs surrounded by terminal hairs; 3) absence of yellow or black dots, dystrophic hairs, and reduced follicular openings on dermoscopy; and 4) minimal hair growth after clinical and dermoscopic confirmation of vellus hairs.
The primary differential diagnoses include alopecia areata, trichotillomania, aplasia cutis congenita, sebaceous nevus, telogen effluvium, and tinea capitis.1,2 Alopecia areata typically presents with a sudden onset of self-limiting alopecic areas, often multiple. Dermoscopic signs include yellow and black dots, broken hairs, exclamation mark hairs, and short vellus hairs. In contrast, dermoscopy of TTA reveals vellus hairs of varying lengths, whereas alopecia areata only presents with short vellus hairs measuring less than 10 mm.7 Trichotillomania is more common in adolescents and rarely occurs in infants. It predominantly affects the parietal and frontal regions, with dermoscopy showing black dots, broken hairs, hair tips resembling a broom or brush, split and curled hair trunk stumps, and, in some cases, bleeding spots and pigmentation. During the resting phase, hairless follicular openings may be observed.8
Aplasia cutis congenita presents clinically as a pink or red atrophic translucent patch, with dermoscopy revealing a translucent area devoid of skin appendage openings.2 Sebaceous nevus is characterized by a yellow-orange, velvety plaque, with dermoscopy showing independently distributed and relatively consistent yellow-red globular structures unrelated to hair follicles.9 Telogen effluvium manifests as acute or chronic diffuse hair loss, with dermoscopy showing normal hair shaft thickness and signs of shorter regrowing hairs, primarily in the frontal and bitemporal areas.10 Tinea capitis is characterized by broken hairs, fine scales, spiral or comma-like hair patterns, and dystrophic hairs, with a positive mycological examination typically confirming the diagnosis.2
Histopathological assessment is essential, as this condition is frequently misdiagnosed as alopecia areata, especially when it manifests in childhood or early adulthood. The classical histopathological presentation includes only vellus follicles in the alopecic area, with no telogen follicles, which are prominent in alopecia areata, or terminal follicles with trichomalacia, as seen in trichotillomania. Follicular "stellae" are absent, and normal terminal follicles may be present at the periphery of the lesion. There is no evidence of inflammatory or scarring processes, and the total number of follicles is preserved.3,4 Congenital cases presumably undergo follicular miniaturization in utero, or terminal hair formation never occurs, preventing "stellae" formation despite the predominance of vellus hairs.11
Currently, no effective treatment exists for TTA, and in most cases, therapeutic intervention is unnecessary.2,4,12,13 Providing reassurance about the benign nature of the condition is crucial. In cases of significant aesthetic or emotional distress, hair transplantation and surgical removal of the lesion are the primary treatment options.6,12,13 Bang et al. described the first successful case treated with topical minoxidil,12 though further evidence is required to confirm its efficacy. In our case, minoxidil was initiated as a strategy to increase overall hair volume and reduce the visibility of alopecic patches.
Marcelo Balbinot Lucca
ORCID: 0000-0001-8395-6742
Approval of the final manuscript version; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic approach of the studied cases; critical literature review; critical manuscript review.
Laura Oliveira Ferreira
ORCID: 0000-0002-6939-7099
Approval of the final manuscript version; data collection, analysis, and interpretation; intellectual contribution to the diagnostic and/or therapeutic approach of the studied cases; critical manuscript review.
Ana Letícia Boff
ORCID: 0000-0002-5207-0567
Approval of the final manuscript version; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic approach of the studied cases; critical literature review; critical manuscript review.
Rodrigo Vettorato
ORCID: 0000-0002-5186-8796
Approval of the final manuscript version; study conception and planning, data collection; analysis, and interpretation, active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic approach of the studied cases; critical manuscript review.
1. Campos JG, Klein AP, Puga C, Akel PBM, Romero SAR, Pinto GM. Use of dermoscopy in the diagnosis of temporal triangular alopecia. An Bras Dermatol. 2015;90(1):123-5.
2. Guan Z, ShiW, Ren M, Bi T, Su H. Clinical and dermatoscopic features of temporal triangular alopecia in infants. Skin Res Technol. 2023;29:e13294.
3. Inui S, Nakajima T, Itami S. Temporal triangular alopecia: trichoscopic diagnosis. J Dermatol. 2012;39:572-4.
4. Yamazaki M, Irisawa R, Tsuboi R. Temporal triangular alopecia and a review of 52 past cases. J Dermatol. 2010;37:360-2.
5. Lederer D, Wilson B, Lefesvre P, Poorten VV, Kirkham N, Mitra D, et al. Atypical findings in three patients with Pai syndrome and literature review. Am J Med Genet A. 2012;158A:2899-904.
6. Unger R, Alsufyani MA. Bilateral temporal triangular alopecia associated with phakomatosis pigmentovascularis type iv successfully treated with follicular unit transplantation. Case Rep Dermatol Med. 2011;2011:129541.
7. Jha AK, Udayan UK, Roy PK, Amar AKJ, Chaudhary RKP. Dermoscopy of alopecia areata-a retrospective analysis. Dermatol Pract Concept. 2017 Apr 30;7(2):53-57.
8. Xingqi Z. Application of dermatoscopy in alopecia. J Clin Dermatol. 2014;43(8): 505-8.
9. Martín JM, Montesinos E, Cordero P, Gonzalez V, Ramon D. Trichoscopy features of trichotillomania. Pediatr Dermatol. 2019;36(2):265-267.
10. Grover C, Khurana A. Telogen efflfluvium. Indian J Dermatol Venereol Leprol. 2013;79:591–603.
11. Sperling L. An atlas of hair pathology with clinical correlations, 2 ed, Editora Informa Healthcare, London, 2012.
12. Bang CY, Byun JW, Kang MJ, Yang BH, Song HJ, Shin J, et al. Successful treatment of temporal triangular alopecia with topical minoxidil. Ann Dermatol. 2013;25:387-8.
13. Chung J, Sim JH, Gye J, Namkoong S, Hong SP, Kim MH, et al. Successful hair transplantation for treatment of acquired temporal triangular alopecia. Dermatol Surg. 2012;38:1404-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}