


Gabriele Harumi Seko; Eldislei Mioto; Jéssica Pagan Faria; Rogerio Nabor Kondo
Financial support: None.
Conflicts of interest: None.
Submitted on: 09/19/2023
Approved on: 10/22/2023
How to cite this article: Seko GH, Mioto E, Faria JP, Kondo RN. Interpolation flap on the posterior surface of the ear. Surg Cosmet Dermatol. 2023;15:e20230304.
The posterior surface of the ear is an uncommon site for skin cancer. It has anatomical and cutaneous characteristics that make local reconstruction difficult using standard surgical techniques. We present a case of reconstruction of a defect on the posterior surface of the ear secondary to excision of a basosquamous carcinoma, using an interpolation flap.
Keywords: Carcinoma, Basosquamous; Ear; Surgical Flaps
The skin is the most common organ affected by cancer, which occurs in places where there is more sun exposure, such as face and neck.1 Depending on the size and site of the tumor, a graft or flap needs to be made to reconstruct the defect resulting from the excision.2
The posterior surface of the ear has curves and ridges, with skin that has little mobility for a simple flap; it is difficult to fix compressive dressings in the case of grafting, which can pose a challenge in reconstructing the site with no anatomical distortions.3
An interpolation flap (IF) consists of using tissue from a site not immediately adjacent to the defect, maintaining a vascular pedicle to supply the flap until neovascularization is established between the flap and the recipient bed, and only after integration of these two sites (recipient and flap) the pedicle is sectioned.4
We report a reconstruction of a defect on the posterior surface of the ear, following excision of a basosquamous carcinoma, in which we used an IF, with good aesthetic and functional results.
We treated a patient with a basosquamous carcinoma on the posterior surface of the left ear:
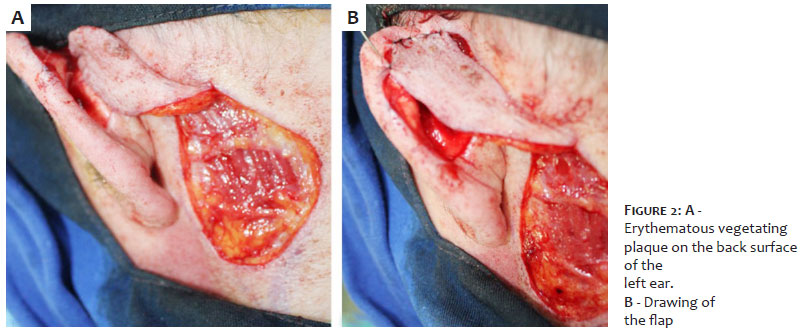
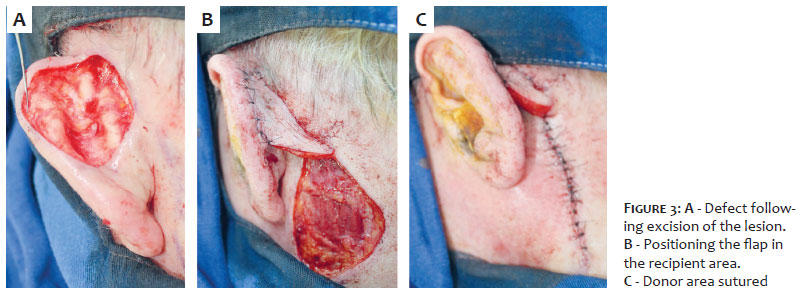
An 83-year-old male patient presented with an erythematous vegetating plaque on the posterior surface of his left ear, measuring 37 × 23mm, whose incisional biopsy confirmed a basosquamous carcinoma, which underwent surgical excision, with margins of 4mm, with a resulting defect measuring 41 × 27mm (Figure 1A). We decided to reconstruct it with an IF.
Patient in horizontal dorsal decubitus;
The lesion was marked with methylene blue or a surgical pen with a 4mm margin (Figure 1A). The donor area was marked, starting in the retroauricular area, at the lower margin and parallel to the defect, extending caudally through the posterior cervical area up to 2cm below the earlobe (Figure 1B);
Antisepsis with topical 10% polyvinyl-iodine;
Infiltrative anesthesia with 2% lidocaine with vasoconstrictor;
Incision of the lesion with a 15 blade and en bloc excision of the piece up to the subcutaneous tissue;
Hemostasis;
Incision of the flap, as previously marked. Detachment of the flap and its positioning and suturing at the defect site, maintaining the vascular pedicle (Figure 2);
Detachment of the edges of the donor site with curved Metzenbaum scissors;
Primary suturing of the donor site (Figures 2 and 3);
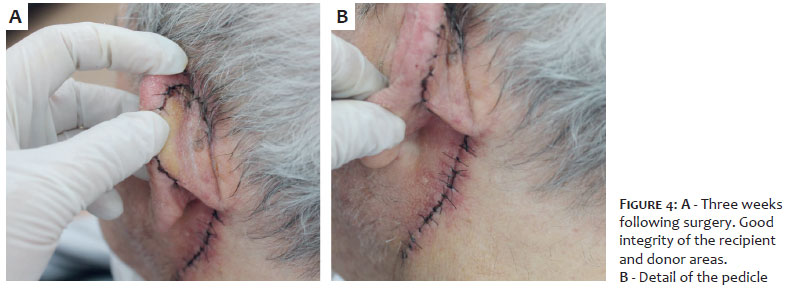
After three weeks (Figure 4), sectioning and repositioning of the pedicle (Figure 5).
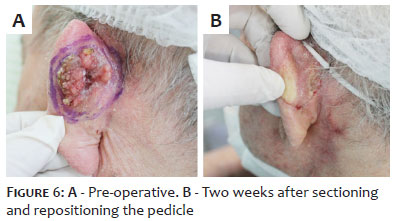
The patient showed good integration between the flap and the recipient area postoperatively. Figure 6 compares the images preoperatively and two weeks following the second stage of the surgery.
Large surgical wounds resulting from excisions of cutaneous neoplasms in the auricular area are challenging for the dermatological surgeon.3 Satisfactory results depend on the technique used and the training to perform it, and the patient's health conditions.4
The posterior surface of the ear is an uncommon site for skin cancer, generally serving more as a donor area because it is less photoexposed.5 For reconstruction of this site, an ideal flap should be thin and flexible, match the color of the recipient area and not have an obvious scar on the donor site.6
Although thick flaps can cause trap doors, which is elevation at the recipient site, the important thing is to maintain the functionality of the ear in the final result, as it supports glasses and hearing aids.7
An IF uses tissue from an area not contiguous to the defect, maintaining a vascular pedicle to supply the flap until neovascularization occurs between the flap and the recipient bed. The disadvantage is that it requires a second stage, after three weeks, when the pedicle will be sectioned after the integration of the two areas (recipient and flap).4 Our patient had a good evolution, maintaining the flexibility of the ear, without a trapdoor, preserving local anatomy and functionality (support for glasses, hearing aid, and protective mask), with the scar hidden in the posterior cervical area.
An IF is a good option for reconstructing defects on the posterior surface of the ear, with good aesthetic and functional results.
Gabriele Harumi Seko
ORCID: 0000-0001-6661-4070
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review.
Eldislei Mioto
ORCID: 0000-0001-5376-9292
Author's contribution: Approval of the final version of the manuscript; critical literature review.
Jéssica Pagan Faria
ORCID: 0000-0001-8727-2348
Approval of the final version of the manuscript; critical literature review.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in the propaedeutic and/or therapeutic conduct of the cases studied; critical literature review.
1. Kondo RN, Maia GB, Bertoncini LA, Silva ST. Retalho em caracol como uma opção de reconstrução de defeito nasal: uma série de dois casos. Surg Cosmet Dermatol. 2021;13:1-5.
2. Kondo RN, Cestari AI, Soares BM, Scalone FDM, Yabar SIA. Pinwheel flap as na option to reconstruct a nasal defect: a series of two cases. Dermatol Arch. .2021;5(1):122-126.
3. Bittner GC, Kubo EM, Fantini BC, Cerci FB. Reconstrução auricular após cirurgia micrográfica de Mohs: análise de 101 casos. An Bras Dermatol. 2021;96(4):408-415.
4. Pavezzi PD, Kondo RN, Pontello Jr R, Lena CP, Kippert JP. Interpolation flap for closing a surgical defect in the cauda helicis. Surg Cosmet Dermatol. 2017;9(4):334-7.
5. Gómez Díaz OJ, Cruz Sánchez MD. Anatomical and clinical study of the posterior auricular artery angiosome: in search of a rescue tool for ear reconstruction. Plast Reconstr Surg Glob Open. 2016;4(12):e1165.
6. Zhang YZ, Li YL, Yang C, Fang S, Fan H, Xing X. Reconstruction of the postauricular defects using retroauricular artery perforator-based island flaps: anatomical study and clinical report. Medicine (Baltimore). 2016;95(37):e4853.
7. McInerney NM, Piggott RP, Regan PJ. The trap door flap: a reliable, reproducible method of anterior pinna reconstruction. J Plast Reconstr Aesthet Surg. 2013;66:1360–1364.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}