


David di Sessa
Submission date: 10/24/2023
Final decision: 03/13/2024
Funding source: Merz Aesthetics LATAM funded medical writing assistance and article processing charges through its affiliate in Brazil – Merz Farmacêutica Comercial Ltda. Despite this support, the study was conducted independently by the medical author, and Merz Farmacêutica Comercial, Ltda. had no participation or influence in the design, conduct, data collection, assessment, or evaluation of the presented data.
Conflict of interest: Dr. di Sessa has been a speaker for Merz Pharmaceuticals.
How to cite this article: Sessa D. Improvement of abdominal laxity with combined use of calcium hydroxylapatite and radiofrequency microneedling. Surg Cosmet Dermatol.2024;16:e20240315.
In clinical practice, not all patients seem to benefit from treatment with calcium hydroxyapatite, often due to the improper indication of this procedure for patients who may require an associated surgical approach. In this context, our objective was to describe a practical method for evaluating and selecting the ideal patient for a non-surgical approach to abdominal skin laxity, along with presenting clinical cases treated with the combined use of calcium hydroxylapatite (CaHA) and microneedling with radiofrequency.
Keywords: Durapatite; Radiofrequency Therapy; Abdomen.
Calcium hydroxylapatite (CaHA) is a biodegradable, resorbable injectable filler, with a well-established safety profile. CaHA is known to induce collagen, proteoglycan and elastin synthesis and promote remodeling of all aspects of the entire extracellular matrix.1
Although CaHA injections have been reported to improve abdominal skin laxity,2 not all patients with this condition appear to benefit from the procedure in the clinical practice. Accurate assessment of abdominal skin laxity is critical to achieving optimal results. Thus, we aim to describe a practical approach to assessing skin laxity and to present clinical cases using a combination of CaHA and radiofrequency microneedling to improve treatment outcomes.
All procedures involving human patients described in this report were conducted in accordance with the ethical standards of our institutional human research ethics committee and with the 1964 Declaration of Helsinki declaration and its subsequent amendments or equivalent ethical standards.
This study was approved by our centralized institutional human research ethics committee (protocol number 67754022.0.0000.5493). Written informed consent was obtained from all the patients to allow the publication of their case details and any accompanying images published.
Eligible patients were men and women over 18 years of age with mild abdominal skin laxity and/or atrophy who agreed to participate in the study. Exclusion criteria included the presence of active skin lesions in the abdominal area, a history of autoimmune disease, use of anticoagulants, body mass index (BMI) greater than 25, or excess skin. Standardized photographs were taken at the following time points: pre-injection, 30 days, and again at 30 and 90 days after the last injection, using consistent lighting, distance, and frontal, oblique, and lateral views.
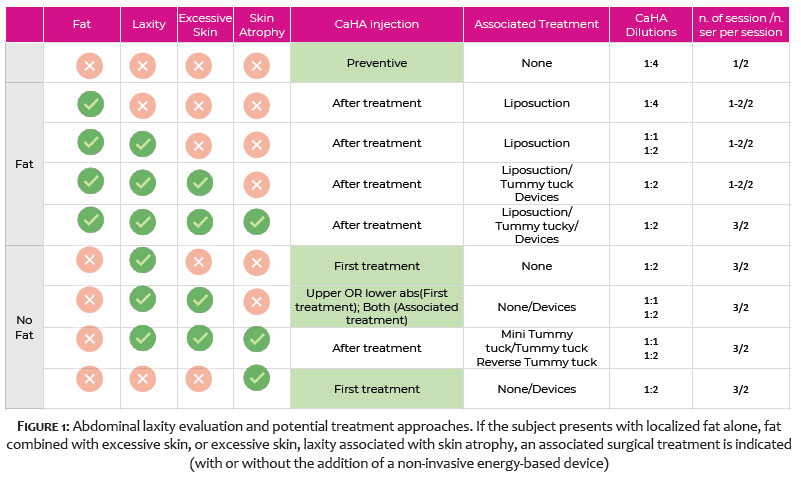
A thorough evaluation of the abdominal area is essential, considering the presence or absence of the following factors: localized subcutaneous fat accumulation, skin laxity, excess skin, and/or skin atrophy. The most important criteria to consider are the presence or absence of fat and excess skin. If the patient presents with localized fat alone, fat and excess skin, or excessive skin, laxity combined with skin atrophy, (possibly in combination with a non-invasive energy-based procedure) may be recommended (Figure 1).
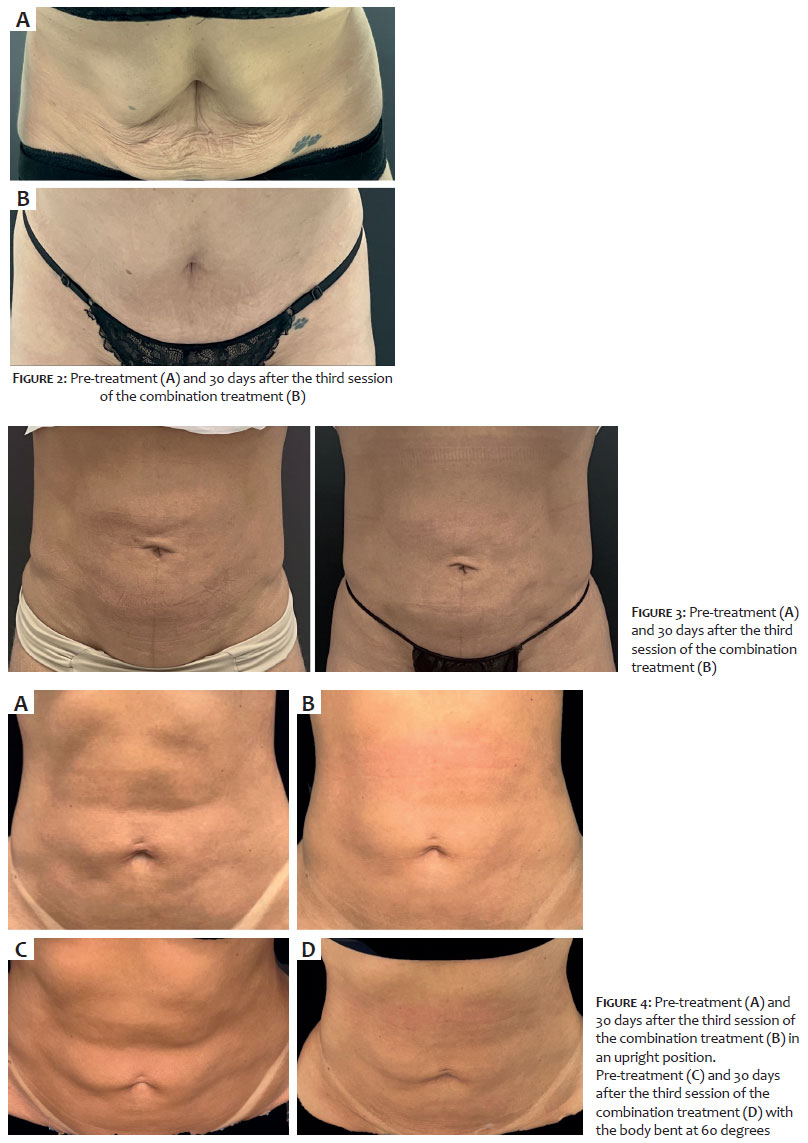
Excess skin can be identified by signs such as a sad umbilicus,3 a supraumbilical fold along the linea alba that can occur after pregnancy or due to aging, sagging skin, or excess skin after liposuction. Other indicators include the presence of an infra-umbilical semilunar line and/or a suprapubic fold. Conversely, patients with skin laxity, but without excessive skin to warrant excisional surgery, or those without localized fat who may benefit from soft tissue contraction after liposuction, are ideal candidates for the combined technique described herein (Figures 2-4).
Anesthesia was administered using a combination of with topical 2% lidocaine, subcutaneous infiltration of a solution containing lidocaine, epinephrine, and saline, along with 70% nitrous oxide inhalation. Radiofrequency (RF) microneedling was applied to the treatment area in four passes: first, in fixed mode (7mm, 30J), followed by cycle mode (6mm, 50-60J), burst mode (7-5-3mm, 30J), and burst mode again (6-4-2mm, 30J). CaHA (Radiesse®; Merz Pharmaceuticals GmbH, Frankfurt, Germany) was injected immediately after the RF microneedling in the same session. The treatment session was repeated after a 30-day interval for a total of three sessions. Two syringes per session of CaHA, diluted 1:2, were injected per session into the subdermal plane using a 22G 70mm cannula with a fanning technique. The total volume was evenly distributed among six entry points (three in the upper abdomen and three in the lower abdomen), with five radial vectors each, injecting 1.5ml per point and 0.3ml per vector. A post-injection massage was performed immediately following the injections. Hydration was recommended as part of the post-procedure care.
We report on 10 female patients between the ages of 35 and 45, all with no relevant medical history (e.g., no use of medications that cause bleeding, no active infections or other inflammatory processes in the treatment area, and no history of autoimmune diseases). All patients showed improvement in abdominal skin laxity, as evaluated by both the subjects and the investigator. No major adverse events were reported.
RF microneedling has been reported as an effective and safe intervention when used safely in combination with other treatment modalities. RF uses low-frequency electromagnetic waves (ranging from 100 kHz to 5 MHz) to generate an electromagnetic field within the skin.4 When skin surface temperatures reach 40° to 45°C, this controlled thermal damage to the reticular dermis stimulates a healing response, promoting neocollagenesis, elastin formation, and angiogenesis, which clinically results in skin tightening and improved skin quality.5 Combining microneedling with RF allows for the delivery of heat at varying depths (from 0.5 to 4 mm), expanding the range of anatomical locations and tissue types that can be effectively treated.4 Additionally, fractional RF microneedling leaves portions of the skin untreated, which reduces healing.4 In an animal model, RF microneedling demonstrated increased levels of tissue remodeling markers, including collagen I and III, compared to microneedling alone group after a single treatment session.6 The Morpheus8 device (InMode Aesthetic Solutions), a fractional RF system with programmable penetration depth and energy delivery, features 24 coated needles that coagulate fat while contracting the reticular dermis and surrounding connective tissue.7 CaHA is a versatile filler, with a well-established safety profile that promotes long-term collagen stimulation, primarily by inducing type 1 collagen deposition. This leads to improved mechanical properties of the skin, unlike type 3 collagen, which is often associated with fibrotic processes.8 Even in high dilutions (1:2 to 1:6), CaHA has been shown to increase type 1 collagen and elastin production up to 7 months after injection in areas such as the neck and décolletage.9 In patients with HIV-related lipoatrophy, a 50% increase in skin thickness was observed 3 months after CaHA application, with 91% of patients maintaining this improvement over an 18-month evaluation period.10 Wasylkowski reported improved skin laxity and dermal thickness in the abdominal region, arms, and thighs, as measured by a skin cutometer and ultrasound, as early as 5 weeks after treatment.2 The abdomen showed the most significant improvement in skin density, with 88% of cases showing improvement compared to baseline. The combination of two well-established non-invasive methods for collagen stimulation, as presented in this preliminary report, improved skin laxity in all patients. This approach offers a promising treatment option for patients with abdominal skin laxity, particularly those with skin atrophy or laxity who prefer to avoid surgery (Figures 2-4). Further studies with blinded evaluations and randomized designs are necessary to validate these findings.
David di Sessa
ORCID: 0009-0006-5534-4267
Approval of the final version of the manuscript, study conception and planning, data collection, analysis, and interpretation, active participation in research supervision, intellectual contribution to the diagnostic and/or therapeutic management of the cases studied, critical review of the manuscript.
1. Gonzalez N, Goldberg DJ. Evaluating the effects of injected Calcium Hydroxylapatite on changes in human skin elastin and proteoglycan formation. Dermatol Surg. 2019;45(4):547-51.
2. Cogorno VW. Body vectoring technique with Radiesse((R)) for tightening of the abdomen, thighs, and brachial zone. Clin Cosmet Invest Dermatol. 2015;8:267-73.
3. Santana KP, Pereira LH, Sterodimas A. Sad umbilicus: prevention and treatment. Aesthetic Plast Surg. 2009;33(3):471-2.
4. Hendricks AJ, Farhang SZ. Dermatologic facial applications of Morpheus8 fractional radiofrequency microneedling. J Cosmet Dermatol. 2022;21(Suppl 1):S1-S9.
5. Dayan E, Burns AJ, Rohrich RJ, Theodorou S. The use of radiofrequency in aesthetic surgery. Plast Reconstr Surg Glob Open. 2020;8(8):e2861.
6. Hong JY, Kwon TR, Kim JH, Lee BC, Kim BJ. Prospective, preclinical comparison of the performance between radiofrequency microneedling and microneedling alone in reversing photoaged skin. J Cosmet Dermatol. 2020;19(5):1105-9.
7. Dayan E, Chia C, Burns AJ, Theodorou S. Adjustable depth fractional radiofrequency combined with bipolar radiofrequency: a minimally invasive combination treatment for skin laxity. Aesthet Surg J. 2019;39(Suppl_3):S112-S9.
8. Almeida AT, Figueredo V, Cunha ALG, Casabona G, Faria JRC, Alves EV, et al. Consensus recommendations for the use of hyperdiluted Calcium Hydroxyapatite (Radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7(3):e2160.
9. Yutskovskaya YA, Kogan EA. Improved neocollagenesis and skin mechanical properties after injection of diluted Calcium Hydroxylapatite in the neck and decolletage: a pilot study. J Drugs Dermatol. 2017;16(1):68-74.
10. Silvers SL, Eviatar JA, Echavez MI, Pappas AL. Prospective, open-label, 18-month trial of Calcium Hydroxylapatite (Radiesse) for facial soft-tissue augmentation in patients with human immunodeficiency virus-associated lipoatrophy: one-year durability. Plast Reconstr Surg. 2006;118(3 Suppl):34S-45S.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}