


Gabriela Tomasi Batiston; Jessica Maksoud Oliveira; Pedro Matheus Benelli; Guilherme Bueno de Oliveira; João Roberto Antônio
Submission date: 06/26/2023
Final decision: 12/01/2023
Funding source: None
Conflict of interest: None
How to cite this article: Batiston GT, Oliveira JM, Beneli PM, Oliveira GB, Antônio JR. Mohs surgery for the treatment of eccrine spiroadenoma: a case report. Surg Cosmet Dermatol. 2024;16:e20240271.
Eccrine spiradenoma is a rare benign epithelial neoplasm derived from the ductal and secretory portions of the eccrine sweat glands. It is characterized by slow growth and may, in some cases, undergo malignant transformation. This report describes a case involving a male patient with a painful, slow-growing lesion present for 3 years. The nodular, lobulated lesion was located on the left frontal region. Due to the left. On account of location, size, and vascularization of the lesion, as well as the need to preserve the facial musculature and ensure complete tumor removal of the tumor with minimal functional damage, Mohs surgery was chosen as the treatment technique.
Keywords: Mohs surgery; Skin; Sebaceous Glands
Eccrine spiradenoma is a rare benign adnexal neoplasm traditionally thought to arise from eccrine glands, although recent studies suggest that it may be of apocrine origin. First described in 1956 by Kersting and Helwig in 1956, their original report included a series of 114 patients. Most cases (97%) present themselves as a single mass, with an equal distribution between men and women.1 Clinically, it appears as a pink to gray, solitary, small, painful nodule, typically pink to gray in color, and most often located on the upper ventral region of the body.1 However, recent studies report that eccrine spiradenomas are more likely to occur on the upper limbs.2,3,4 The present report has described a case presented here describes a solitary lesion in the frontal region, which is a rare location for this tumor. The varied presentations of eccrine spiradenoma make it difficult to classify clearly. Yoshida et al.4 has proposed a categorization system based on clinical and histological findings. The clinical classification includes solitary or multiple forms, with additional distinctions to describe their appearance and define the distribution pattern (linear, zosteriform, nevoid, or blascoid). Histologically, eccrine spiradenomas are classified as either benign or malignant, with further distinctions based on histological characteristics (common, vascular, or cystic).5 Due to its many possible presentations, the differential diagnosis can be challenging. Accurate diagnosis is crucial, given the potential for malignant transformation.6 Immunohistochemistry can be particularly helpful, especially in malignant cases of malignancy.6 The primary treatment for both benign and malignant eccrine spiradenomas is the surgical excision. Other treatment options include radiotherapy, carbon dioxide laser ablation, or chemotherapy in cases of multiple or malignant lesions.6 Some authors recommend combining surgical excision (using complex linear closures and random pattern cutaneous flaps for reconstruction) with carbon dioxide laser therapy, resulting in good cosmetic outcomes.7 Because of the potential for malignant transformation, wide surgical excision at the same surgical time or Mohs micrographic surgery is often considered the best approach, as these methods offer conservative treatment, low recurrence rates, and minimize the risk of malignancy.6 In the case presented here, the eccrine spiradenoma was successfully treated using the Mohs technique, achieving complete lesion removal with excellent cosmetic results and preservation of frontal muscle function.
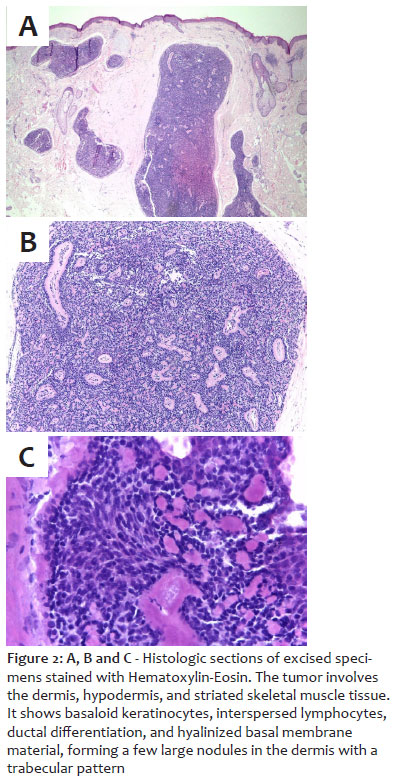
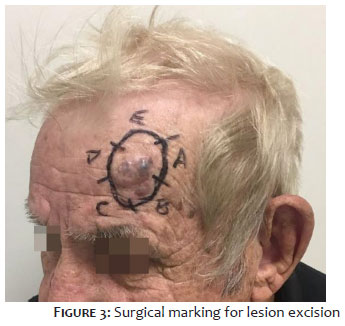
A 72-year-old male patient was referred to the Dermatology Service due to a painful lesion in the left frontal region that had been slowly growing for approximately three years. Upon examination, a nodular, lobulated lesion was observed, measuring 2.0 × 1.8 cm. The lesion was covered by normal skin, with blue-greyish, painful areas, adhered to deeper tissues, and exhibited limited mobility (Figures 1). The initial differential diagnosis included common tumors of the cutaneous appendages, such as cylindroma, eccrine carcinoma, papillary hidradenoma, and eccrine spiradenoma as well as other possibilities, such as B-cell lymphoma, amelanotic melanoma, and cutaneous metastasis. An ultrasound of the lesion revealed hypoechogenic oval images with lobulated contours, in the frontal region, underlying the skin lesion. The lesion measured 2.2 × 2.0 × 1.0 cm at its largest axis, with flow to the Doppler study, showing blood flow. The imaging also indicated a clear cleavage plane from the adjacent cortical bone and preserved muscle planes. An incisional biopsy was performed, revealing diffuse proliferation of ovoid, monomorphic cells, some with a basaloid appearance, arranged in lobes with hyalinized septations. These findings were consistent with the diagnosis of eccrine spiradenoma (Figure 2A). Due to the size of the lesion, location, and vascularity of the lesion, Mohs micrographic surgery was selected as the best treatment approach. This technique was chosen to preserve the frontalis muscle while ensuring complete tumor removal and maximizing tissue preservation. The lesion was also subjected to histopathologic examination of the lesion and immunohistochemistry (Figure 2B and C). Surgical markings were made (Figure 3) and the procedure was performed in an outpatient setting by a dermatologic surgeon with a pathologist involved throughout the surgery. The lesion was divided into five fragments to assess the lateral margins, as determined by palpation and lesion topography, and by two fragments to assess the deep margins. In the first stage of surgery, all lateral margins were free of neoplasia, but two deep fragments have showed positive muscle invasion by an eccrine spiradenoma. Therefore, the surgical margin was extended deeper, and the entire muscle layer was removed. In the second stage, all specimens from the extended margins were free of neoplasia. The tissue was sent for immunohistochemical analysis, which confirmed ductal differentiation was confirmed with epithelial membrane antigen (EMA) and carcinoembryonic antigen (CEA) markers. The immunophenotypic profile in combination with the morphologic findings confirmed the diagnosis of eccrine spiradenoma. The final defect was reconstructed with a rotational flap, with primary closure of the edges of the lesion margins to preserve the position of the ipsilateral eyebrow (Figures 4 and 5).
Eccrine spiradenoma is a rare benign tumor that can occur at any age, although it is most commonly seen more frequently between the second and fourth decades of life, with no gender predominance.8 Clinically, spiradenomas present as a dermal or subcutaneous papules or nodules that can appear anywhere on the body. Rarely, these lesions can grow to several centimeters in diameter and may be painful. Due to the nonspecific nature of the clinical presentation, biopsy is required for the diagnosis. However, eccrine spiradenoma should be considered in the setting of a nodular, bluish, and painful lesion. Spiradenomas may present as solitary or multiple lesions, and in some cases may be associated with other tumors such as cylindroma and trichoblastoma. When multiple lesions are present, Brooke- Spiegler syndrome should be considered as a possible diagnosis.9 Histologically, eccrine spiradenomas are usually found in the subcutaneous fat layer, with well-defined margins and a lobulated appearance. Blood flow is often observed in the peripheral region of the tumor, with or without central blood flow.3 In this case, the central region.3 The present work shows a tumor involved the dermis, hypodermis, and striated skeletal muscle tissue, complicating the therapeutic approach challenging. The use of ultrasound as a prognostic tool has been reported in some studies and correlates well with histologic findings. Ultrasound can help assess the extent of the tumor, identify possible recurrence, and determine any association or not with trichoepithelioma or cylindroma.3,4 Treatment for benign or malignant eccrine spiradenomas typically involves conservative excision or simple enucleation.9 Other options, particularly for multiple or malignant cases, include a combination of surgical treatments, radiation therapy, carbon dioxide laser ablation, or chemotherapy if multiplicity or malignancy.6,7
This article presents the clinical case of a 72-year-old male patient with a painful lesion on his forehead that was definitively diagnosed as an eccrine spiradenoma by biopsy incisional biopsy. The Mohs technique was chosen for treatment, and margin expansion was necessary due to the tumor's invasion of the skeletal muscle layer. Complete excision of the lesion was achieved with preservation of frontal muscle function and an excellent cosmetic results. Eccrine spiradenoma has an unclear etiology and presents in different clinical forms, requiring histologic confirmation to determine the most appropriate therapeutic approach, as conservative treatment options are available. Case reports such as this one are essential to guide treatment decisions and shed light on the different therapeutic options for managing this rare condition.
Gabriela Tomasi Batiston
ORCID: 0000-0001-7514-0233
Statistical analysis, Approval of the final version of the manuscript, Study conception and planning, Drafting and writing the manuscript, Data collection, analysis, and interpretation, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of the cases studied, Critical literature review, Critical review of the manuscript
Jessica Maksoud Oliveira
ORCID: 0000-0003-0678-5702
Study conception and planning, Data collection, analysis, and interpretation, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of the cases studied, Critical literature review, Critical review of the manuscript
Pedro Matheus Benelli 0009-0004-1265-4420
Approval of the final version of the manuscript, Critical literature review
Guilherme Bueno de Oliveira 0009-0008-2684-1103
Approval of the final version of the manuscript
João Roberto Antônio
ORCID: 0000-0002-0268-5934
Approval of the final version of the manuscript.
1. Kersting DW, Helwig EB. Eccrine spiradenoma. AMA Arch Derm. 1956; 73(3):199-227.
2. Filho JH, Choi YW, Cho YS, et al. Um caso de espiradenoma écrino: um tumor de tecido mole raramente visto na superfície extensora do braço. Ann Dermatol 2017;29(4): 519–522
3. Hwang CM, Kang BS, Hong HJ, et al. Características ultrassonográficas do espiradenoma écrino. J Ultrasound Med 2018; 37(5):1267–1272.
4. Yoshida A, Takahashi K, Maeda F, Akasaka T. Vários espiradenomas écrinos vasculares: um relato de caso e revisão do trabalho publicado de vários espiradenomas écrinos. J Dermatol. 2010; 37(11):990–994.
5. Ter Pooten MC, Barrett K, Cook J. Familial eccrine spiradenoma: um relato de casoe revisão da literatura. Dermatol Surg. 2003; 29(4):411–414.
6. Han YD, Huan Y, Deng JL, Zhang YG, Zhang CH. MRI appearance of multiple eccrine spiradenoma. Br J Radiol 2007; 80:e27–e29.
7. Jean L. Bolognia. Tratado de Dermatologia. 3 ed . Rio de Janeiro: Elsevier, 2015.
8. Kwon KE, Kim SJ, Choi HJ, et al. Aspecto ultrassonográfico de um espiradenomaécrino: relato de caso. J Clin Ultrasound 2018; 46(7):494–496.
9. Englander L, Emer JJ, McClain D, Amin B, Turner R. Um caso raro de Espiroadenomas Écrinos de Múltiplos Segmentos. J Clin Aesthet Dermatol. 2011; 4 (4):38–44.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}