


Ana Paula Bald; Luís Fernando Figueiredo Kopke; Ariel Córdova Rosa; Telma Sakuno; Athos Paulo Santos Martini
Financial support: None.
Conflict of interest: None.
Submitted on: 29/07/2023
Approved on: 07/08/2023
How to cite this article: Bald AP, Kopke LFF, Rosa AC, Sakuno T, Martini APS. Supratrochlear artery pseudoaneurysm: A rare complication of skin flap surgery. Surg Cosmet Dermatol. 2023;15:20230288.
Arterial pseudoaneurysm is a rare complication caused by damage to the arterial wall, resulting in a locally confined hematoma connected to the lumen of the artery. We report the case of a patient on anticoagulants who developed nodules at the surgical wound site after Mohs micrographic surgery for basal cell carcinoma. The initial clinical suspicion was the formation of a simple hematoma. However, Doppler ultrasound examination revealed the presence of pseudoaneurysms in the bilateral supratrochlear arteries. We believe this is the first reported case of supratrochlear artery pseudoaneurysm following dermatologic surgery.
Keywords: Aneurysm, False; Carcinoma; Basal Cell; Ultrasonography, Doppler, Color
Pseudoaneurysms are rare complications caused by damage to the arterial wall resulting in incomplete hemostasis and the formation of a locally confined hematoma. Once a hematoma reaches a certain size, it may not resolve spontaneously, resulting in the formation of a pseudomembrane of coagulation cascade products with turbulent blood flow within.1 The most common presentation of a pseudoaneurysm occurs in the femoral artery following vascular surgery. However, rarer cases include visceral pseudoaneurysms due to chronic pancreatitis and traumatic pseudoaneurysms of the superficial temporal artery.1,2 Doppler ultrasound is the gold standard for diagnosis, allowing assessment of size, location, and contact with adjacent structures to guide treatment.3
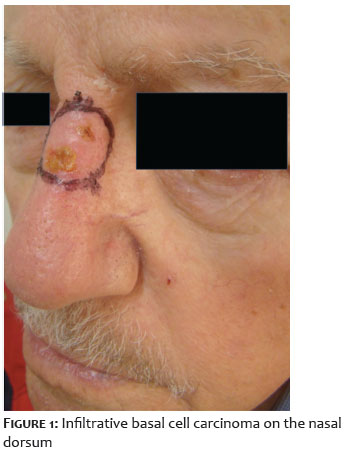
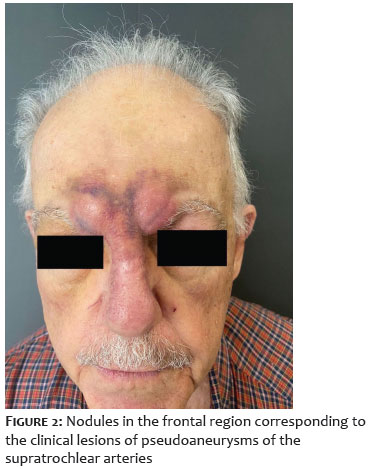
An 84-year-old male patient was diagnosed with an infiltrative basal cell carcinoma (BCC) on the nasal dorsum near the glabellar region (Figure 1). He had a history of chronic atrial fibrillation and was on regular apixaban therapy. The patient underwent Mohs micrographic surgery using the Munich method to treat the BCC, resulting in a 2.6-cm surgical defect after tumor removal and a final 6.5-cm surgical defect. Wound was then closed using the glabellar advancement flap technique (Figure 2). There were no complications or abnormal bleeding during surgery or in the immediate postoperative period.
To prevent hemorrhagic complications, anticoagulation was discontinued five days prior to surgery. As there was no bleeding within the first 48 hours postoperatively and the patient needed to resume apixaban, medication was resumed 72 hours after surgery. On the fourth postoperative day, the patient developed extensive facial ecchymosis. Medication was continued, and the patient was closely monitored. Ecchymosis gradually improved, but on postoperative day 10, two erythematous-violaceous nodules appeared, measuring 2.2 cm in the right glabellar region and 2.4 cm in the left glabellar region. The leading diagnostic hypothesis was the formation of a seroma or hematoma, so bilateral puncture and aspiration of the nodule contents was performed by using a 10ml syringe and a 21G needle, draining a total of 10ml of blood. Lesions were reduced in size after surgery and a compressive dressing was applied.
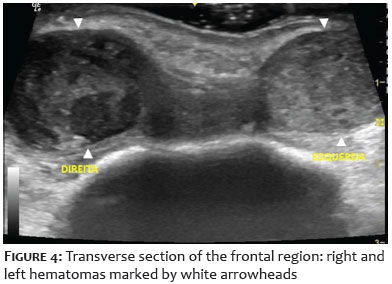
Anticoagulant was therefore discontinued. Patient was re-evaluated 14 days after the procedure and the nodules had increased in size (Figure 3). At that time, he was referred for ultrasound to confirm the diagnosis. A color Doppler ultrasound (Logiq E, GE Medical System CO. LTD.) was performed with a 12 MHz linear multifrequency transducer and showed two hypoechoic nodules in the bilateral frontal region without flow consistent with hematoma (Figure 4).
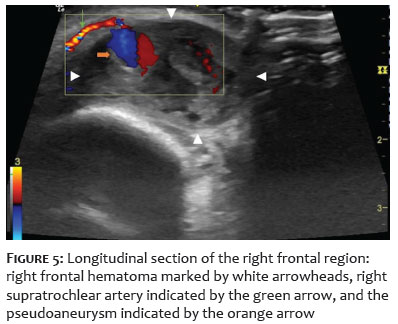
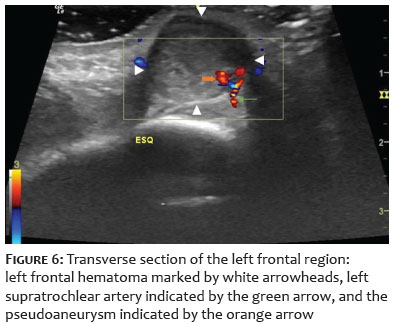
The right-sided hematoma had a heterogeneous echo texture and measured 2.9 × 1.4 × 2.2 cm. Within this nodule, another well-defined anechoic nodule was observed, measuring 0.7 × 0.7 cm, with bidirectional flow on color Doppler examination, fed by the right supratrochlear artery located superficially at the periphery of the hematoma (0.3 cm from the epidermis) (Figure 5). The left-sided hematoma, measuring 2.2 × 1.3 × 1.8 cm, had a more homogeneous echo texture than the right-sided one. Left supratrochlear artery was located deeper (approximately 1.0 cm from the epidermis) at the periphery of the hematoma.
A small nodule measuring 0.2 × 0.2 cm was observed adjacent to the left supratrochlear artery and showed bidirectional flow on color Doppler examination (Figure 6). Visualization of the nodular images along the arteries, combined with the presence of bidirectional color flow on Doppler (yin-yang sign), led to the diagnosis of supratrochlear artery pseudoaneurysm.
After the diagnosis of supratrochlear artery pseudoaneurysm, patient was referred to vascular surgery and underwent ligation of supratrochlear arteries 7 days after the ultrasound with excellent results. Thirty days after the procedure, the patient showed complete resolution of lesions.
Hematomas and seromas are complications that can be expected after dermatologic surgery. These complications should be suspected when patients develop swelling or nodules over the postoperative wound days or weeks after the procedure. However, pseudoaneurysm has never been reported as a complication of dermatologic surgery.
Pseudoaneurysms are caused by a localized rupture of the arterial wall, which may occur because of vascular trauma, resulting in a contained hematoma that maintains a persistent connection to lumen of the arteria.1,2 They can be classified as iatrogenic or noniatrogenic. Iatrogenic pseudoaneurysms are the most common and typically occur after arterial access in endovascular procedures or after surgical vascular anastomoses. Noniatrogenic causes include trauma, infection, and chronic pancreatitis.1
Facial artery pseudoaneurysms are rare. There are a few reports in the literature of pseudoaneurysms of the internal carotid, maxillary, and superficial temporal arteries after cranioencephalic trauma.4-9
Intraoperative bleeding and hematoma formation are well-documented adverse effects in patients taking anticoagulants, including factor Xa inhibitors, such as apixaban.10,11 There is also an increased risk of pseudoaneurysm in patients on anticoagulants and dual antiplatelet therapy.2 Since pseudoaneurysms form due to damage to the arterial wall, we believe that extensive and deep surgical defects near larger vessels are more prone to complications such as pseudoaneurysms in dermatologic surgery.
In the case described, we believe that the use of anticoagulants, together with the trauma caused by the puncture and aspiration of the hematoma, may have contributed to the formation of pseudoaneurysm. The possibility of a pseudoaneurysm should be considered in cases of persistent hematomas, some of which may be pulsatile and painful.
Doppler ultrasound has a sensitivity of 94-99% and a specificity of 94-97% for the diagnosis of pseudoaneurysm, making it the diagnostic tool of choice.12 in-yang sign, created by the inflow and outflow of blood during systole and diastole, is used to differentiate pseudoaneurysms from hematomas and true aneurysms.13 Besides, ultrasound helps to determine size, location, and contact with underlying structures, aiding in therapeutic planning.12
Small pseudoaneurysms may resolve spontaneously after compression with bandages. However, pseudoaneurysms larger than 2 cm, those that are growing, or those with large adjacent hematomas should be treated. Therapeutic options include ultrasound-guided compression, ultrasound-guided thrombin injection, and surgical correction.14
Pseudoaneurysm is an extremely rare vascular complication. We believe this is the first reported case involving the supratrochlear artery after dermatologic surgery. The use of anticoagulants is a risk factor for hematoma and pseudoaneurysm formation, and their temporary suspension should be evaluated on a case-by-case basis. In the reported case, the patient developed associated complications even after suspension of the medication according to current guidelines. In this case, Doppler ultrasound was the gold standard test for diagnosis and surgical planning.
Ana Paula Bald
ORCID: 0009-0004-4755-6337
Preparation and writing of the manuscript; critical literature review; critical review of the manuscript.
Luís Fernando Figueiredo Kopke
ORCID: 0000-0002-33505887
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Ariel Córdova Rosa
ORCID: 0000-0003-4040-2891
Preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Telma Sakuno
ORCID: 0000-0001-99496277
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
Athos Paulo Santos Martini
ORCID: 0000-0003-0104-573
Critical review of the manuscript.
1. Peters S, Braun-Dullaeus R, Herold J. Pseudoaneurysm. Hamostaseologie. 2018;38(3):166-172.
2. Stone PA, Martinez M, Thompson SN, Masinter D, Campbell JE, Campbell JRI, et al. Ten-year experience of vascular surgeon management of Iatrogenic pseudoaneurysms: do anticoagulant and/or antiplatelet medications matter? Ann Vasc Surg. 2016;30:45-51.
3. Sarioglu O, Capar AE, Belet U. Interventional treatment options in pseudoaneurysms: different techniques in different localizations. Pol J Radiol. 2019;84:e319-e327.
4. Pinto PS, Viana RS, Souza RRL, Monteiro JLGC, Carneiro SCAS. Pseudoaneurysm of the internal carotid artery after craniofacial traumatism: series of cases and integrative literature review. Craniomaxillofac Trauma Reconstr. 2021;14(4):330-336.
5. Saliba E, Goldberg LJ. Superficial temporal artery pseudoaneurysm: report of two cases and review. J Cutan Pathol. 2022;49(5):482-486.
6. Rubio-Palau J, Ferrer-Fuertes A, García-Díez E, Garcia-Linares J, Martí-Pagès C, Sieira-Gil R. Traumatic pseudoaneurysm of the superficial temporal artery: case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;117(2):e112-4.
7. Choo MJ, Yoo IS, Song HK. A traumatic pseudoaneurysm of the superficial temporal artery. Yonsei Med J. 1998;39(2):180-3.
8. Stapleton CJ, Fusco MR, Thomas AJ, Levy EI, Ogilvy CS. Traumatic pseudoaneurysms of the superficial temporal artery: case series, anatomy, and multidisciplinary treatment considerations. J Clin Neurosci. 2014;21(9):1529- 32.
9. Al-Saadi NJ, Bakathir A, Al-Mashaikhi A, Al-Hashmi A, Al-Habsi A, Al-Azri F. Maxillary artery pseudoaneurysm as a complication of maxillofacial injuries: report of three cases and literature review. Sultan Qaboos Univ Med J. 2019;19(4):e364-e368.
10. Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, Johnson M, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699-708.
11. Chai-Adisaksopha C, Crowther M, Isayama T, Lim W. The impact of bleeding complications in patients receiving target-specific oral anticoagulants: a systematic review and meta-analysis. Blood. 2014;124(15):2450-8.
12. Coughlin BF, Paushter DM. Peripheral pseudoaneurysms: evaluation with duplex US. Radiology. 1988;168(02):339–342.
13. Abu-Yousef MM, Wiese JA, Shamma AR. The “to-and-fro” sign: duplex Doppler evidence of femoral artery pseudoaneurysm. AJR Am J Roentgenol 1988;150(03):632–634.
14. Sarioglu O, Capar AE, Belet U. Interventional treatment options in pseudoaneurysms: different techniques in different localizations. Pol J Radiol. 2019;84:e319-e327.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}