


Luís Fernando Figueiredo Kopke1; Aira Novello Vilar2
Financial support: None.
Conflicts of interest: None.
Submitted on: 25/07/2023
Approved on: 11/09/2023
How to cite this article: Kopke LFF, Vilar AN. Examine the slide instead of just reading the report! Surg Cosmet Dermatol. 2024;16:e20240282.
Histopathology reports are the pathologist's description of a microscopic morphological image, which can be understood as long as the basic elements of the histological structures are known. However, actually viewing the morphological image can be more helpful in understanding what is really being described, similar to the examination of radiograms, which is directly performed by the orthopedist despite the report being made by the radiologist. This article discusses this scenario, with the aim of encouraging surgeons to view and inspect morphological images to improve their understanding of the clinical-surgical status and their analysis of the state of the surgical margins or the histological subtype.
Keywords: Mohs Surgery; Official laboratory; Pathology; Reoperation; Skin Neoplasms
Years of experience with surgeons from the most diverse specialties have revealed one fact to us: only a few of them can properly process a surgical specimen and interpret the histopathological findings. Although this is not absolutely necessary, most surgeons only interpret reports and would be unable to argue with the pathologist if they received a false positive report, as they have rarely experienced the routine of histotechnology. Only micrographic surgeons are slightly more experienced in examining histological sections, so the pathologist's report, which rarely describes possible technical artifacts or other biases, becomes an unassailable truth, despite the footnote routinely stating that, in case of any questions, the pathologist should be informed and the case revised.
In our medical literature review on the subject, we hardly found anything specifically about this fact, and sometimes, surreptitiously, possible errors in histotechnical manipulation are poorly analyzed1 or dismissed as "unlikely".2
This short review seeks to encourage surgeons to get used to examining the histological sections of their own surgeries and, over time, to realize that there are a significant series of events that can interfere with the pathologist's report. The pathologist, in turn, can be misled even by a lack of adequate information from the surgeon who sent the material. It's worth noting that every Anatomic Pathology laboratory has its own, often standardized, routine, but the rule is that pathologists routinely receive a large number of ready-made slides of the most varied tissues and cases, processed by their histology technicians. The greater the volume of cases in a department, the greater the chance of errors. No one is infallible. The histopathological sections on the slide, which are the product of histological processing, must be interpreted in the light of all the phenomena that can make the report as accurate as possible. No wonder some laboratories always put a note in their reports: "every histopathological examination must be correlated with the patient's clinical history, otherwise the interpretation of the result is only relative."
In laboratory routine, the surgical specimen first needs to be fixed. Formalin (37% formaldehyde, diluted in a 9:1 or 10% ratio) is usually used.3,4 Buffered formalin is ideal, because if immunohistochemistry (IHQ) is required; unbuffered formaldehyde can be harmful.5,6 Fixation time is also important. It should be a minimum of six hours and a maximum of 72 hours so that the antigens are preserved. Once this time has elapsed, the results of histochemical or immunohistochemical staining may be affected. The volume of formalin required for proper fixation should be given special attention, with the ideal parameter being at least 10 times the volume of tissue to be fixed. After the specimen has been resected, it should be placed in the fixative (formalin) within a maximum of 30 minutes.7,8,4 The process of fixation in formalin will start the hardening process to enable the extremely fine cut it will undergo on the microtome. The length of time it remains in formalin depends on the size of the piece. The larger the piece, the longer the time. Formalin penetrates the tissue at around 1mm/hour. A 2cm specimen takes, on average, 24 hours for the desired initial fixation, while a 10cm specimen would take three to five days.9 Prolonged time in formalin (longer than five days) can lead to deformation of the surgical specimen, sometimes requiring artifices to maintain the shape of the specimen, such as placing a weight on it or even fixing it to a rigid surface in the desired direction, even before it is introduced into the formalin.10 The size of the container that will hold the surgical specimen is also important, as small vials for large specimens may contain an insufficient amount of formalin for good fixation, and deform the specimen if it remains in the vial for longer than necessary. Ideally, the surgical specimen should not be compressed inside the flask and should retain its original shape with a sufficient amount of formalin. Fixation will be completed over the course of around 10 to 12 hours, during which time the specimen will be dehydrated by immersion in alcohol, clarified, and paraffinized until the rigidity required for cutting is achieved. This is usually done automatically in a tissue processor called "technicon."3,4,7,9,10
One of the most important steps in histotechnology is painting the surgical edges. Without this, the edge can be fragmented during cutting or processing, and the pathologist may find it difficult to analyze, as they may not be referring to the true surgical edge.4,9 Depending on the situation, the surgeon can paint the surgical edge to suit their liking, which is much better than just placing a surgical wire in a certain position in an attempt to orient the specimen. Drawing a picture of the different colors with the request for the examination can be very useful for the pathologist. Preferably, the surgical edge should be painted before fixation or before the specimen is placed in the "technicon" so as not to contaminate areas unrelated to the surgical edge, such as the cleavage surface, for example.4,8,9,10
Once the specimen has been completely fixed and the surgical edges painted, cleavage (sampling) is performed. Many technicians perform the cleavage right after painting the surgical edges, fixing the paint immediately with acetic acid. The cleavage surface should not be painted and should be rectilinear during cutting. It is also important that the cleavage is performed with a single cut and with the specimen properly fixed; otherwise, a softened surface can deform the specimen, making it difficult to recognize the true surgical edge.
The next step is to embed the specimen in liquid paraffin, ensuring that when it solidifies, the surface desired for cutting fits as perfectly as possible to the straight edge of the paraffin block, preventing the block from being worn down too much during cutting in order to obtain the desired cut. An inclusion lacking the necessary care can leave the specimen poorly positioned in the paraffin block, resulting in an inadequate cutting surface. This is extremely important for cuts parallel to the orientation of the surgical margin ("in face" cuts), which are widely used in peripheral micrographic surgery methods (Mohs and Tübingen Pie).11
The paraffin block is then fixed to the microtome to make the cuts. Depending on the application, such as "in face" cuts, the initial adjustment of the movable head of the microtome must be made in such a way as to cut the entire desired surface on the first attempts. Otherwise, excessive wear on the block could compromise the correct assessment of the surgical edge. Most technicians are skilled and careful, but when the volume of work increases, the speed of processing can generate more wear, as it is easier just to rough up the block than to carefully adjust it, check for wear, adjust it again, until the first cut reaches the entire surface to be examined. Too much wear and our "in face" surgical edge is gone. Once the desired cut has been obtained, it is picked up and placed on the slides, where it will be stained. A coverslip is added to protect the cuts and the process is finished.
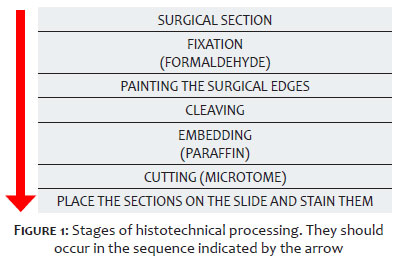
All this processing has been described here because it is essential that the attending physician is aware of every technical detail so that, when examining the slide, they can realize when these steps may not have been properly followed. Pathology laboratories receive a large number of exams of the most varied types every day and it is not uncommon for some technical flaws to be found which can distort the pathologist's report regarding the state of the surgical margins. The pathologist was not present at the surgery and often did not receive any information about the perioperative procedure that could have influenced his judgment. This is not about "doubting the technical capacity of laboratories," because mistakes, who does not make them? The duty of the zealous surgeon would only be to better investigate the situation, and the more information he has or can gather from what has already been done, the better for the patient. We all know that the surgical specimen is never examined in its entirety (not even in micrographic surgery!). Thus, the histopathology report that assesses the surgical margin is actually a logical abstraction of the pathologist's judgment of the histopathological picture and its relationship to the surgical edges, which may represent the real picture (correct report) or contain a false negative or false positive. Figure 1 summarizes the stages of histological laboratory processing of the surgical specimen.
Patients who have undergone conventional surgery based on the concept of a safety margin and who, typically one to two years later, develop a tumor with the same histopathological characteristics at the same site as the primary tumor, are diagnosed as having a recurrent tumor. How can this be explained if the histopathology report from the previous surgery was "free margins?" Most surgeons are well aware of this situation, because they know that the statement in the report that the margin is free refers to a non-full sample. What many surgeons are not aware of is that, in most cases, this sample is not even 1% of the total surgical margin. There are certainly highly careful laboratories that routinely perform total inclusion with thin slices, especially when the pathologist performs the macroscopy and is dedicated to a specific sub-area such as Dermatopathology. However, the routine of large laboratory groups, which are increasingly common in the market, is to have trained macroscopy technicians to standardize the process, lacking the appropriate technical expertise (medical) to interpret the data in the request and the diagnostic hypotheses and thus decide on a more "customized" form of sampling for each case.4,9 It should also be pointed out that total inclusion often implies a greater number of blocks, with costs that multiply and cause financial losses. But the fact is that many surgeons know that if the sample is not totally representative, a small portion of these results may represent a false negative, i.e. a portion of the tumor was left in the patient, although the report was "free margins." This would justify tumor recurrence. Once there are clinical signs compatible with a tumor at the previously operated site, the decision to reoperate the patient is easy to make. This situation is more frequent the more infiltrative the tumor is.
The report has to include the information, not always observed by the surgeon, about whether the specimen has been fully included or not. The acronyms generally used are: TI (totally included; total inclusion), PI (partially included; partial inclusion); WR (with reservation of material from macroscopy) or LR (lacking reservation of material from macroscopy and therefore totally included) can also be used. The laboratory must not discard the remains of the macroscopy samples for six months, so that the pathologist can, upon request, complete the inclusion of the entire specimen.4 However, lack of familiarity with histotechnology processing means that many surgeons fail to correctly interpret the macroscopy items on the report.
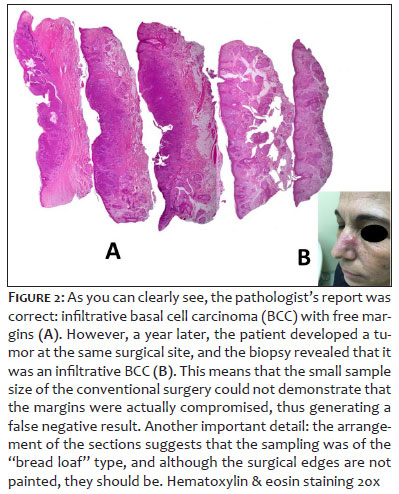
Figure 2 is an example of a false negative.
While the false negative is only noticed when the tumor recurs, the false positive is based only on the histopathological report, since this information will be available a few days after the surgery. At first, this comes as a surprise to both the patient and the surgeon, as the concept of a safety margin, which was initially considered "safe," has not proven to be effective in completely removing the tumor. The clinic no longer helps and what we have is a newly acquired scar. Most surgeons do not have any questions about this report, as they cannot argue with the pathologist because they are not used to examining slides with histopathological sections. The surgeon is left with two options: observe or reoperate.
Is observing wrong or risky? It has long been said that only a third of tumors with reports of compromised margins result in clinical recurrence.12-16 Many surgeons choose to observe. Some because they are suspicious of the report without contesting it. Others believe that skin cancers (mainly basal cell carcinomas) have a "benign behavior, as they do not cause metastases" and that a recurrence would not be a problem.16 Thus, in the absence of clinical signs, waiting for progression does not seem to be a course of action that will worsen the patient's long-term prognosis. However, we have to remember that observation is not treatment, especially if the condition really requires re-intervention.
Perhaps the crucial question that should be answered is: is there really a possibility that the patient has a residual tumor, or could this report represent a false positive? In our experience, false positives can occur in three common cases:
• Technical artifacts
• The type of view of the pathologist
• Coincident margin
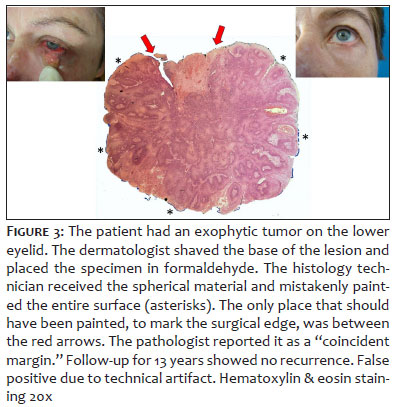
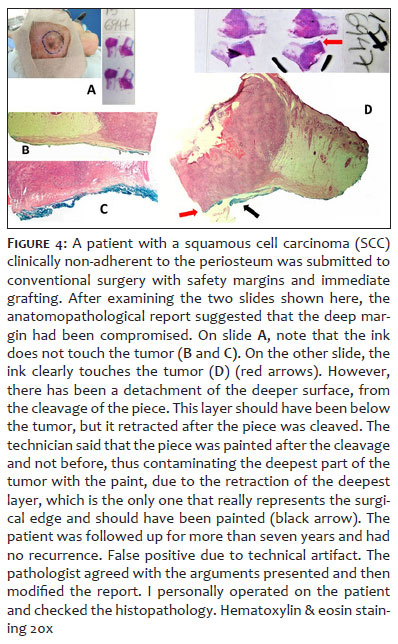
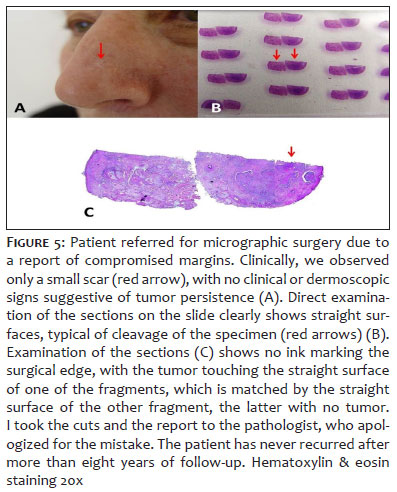
A very common artifact of technique is the failure to demarcate surgical edges with ink or even the contamination of surfaces with ink which are not surgical edges (free edge or even cleavage surface) (Figures 3, 4, 5).
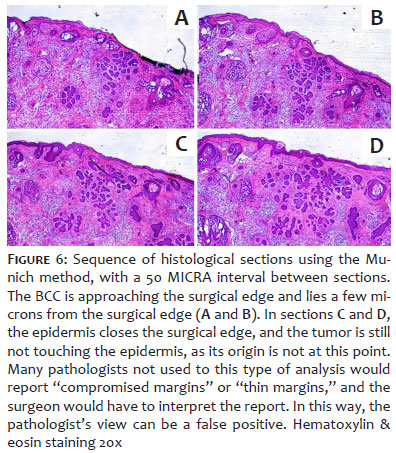
Many pathologists use different terminology that can mean "compromised margins" to surgeons, such as the term "exiguous margins" or margins smaller than 1mm. In micrographic surgery, especially when using the Munich method, a margin of 1mm can be more than enough, and pathologists unaccustomed to interpreting this variation of micrographic surgery could be unsure about stating that the margins are free. Several times I have taken reports of compromised margins to the pathologist and, examining them with a microscope, I was told that "they thought it best to judge the margin compromised because the tumor was so close," even though in the histological sections the tumor mass would not touch the surgical edge. It is therefore important to know what interpretation the pathologist usually gives to these cases, as the professionals involved have different interpretations (Figure 6).
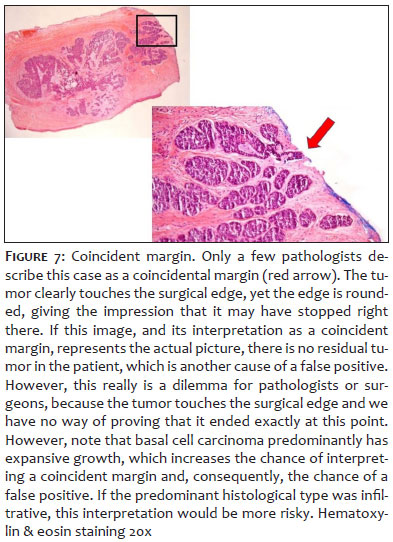
Some pathologists use the term "coincident margins" when the tumor only appears to touch the surgical edge focally. Others prefer to judge this as a compromised or focally compromised margin. Undoubtedly, this can represent a dilemma when, in fact, the tumor only tangents the surgical edge, but does not go beyond it. When examining cases like these, the pathologist's interpretation of a compromised margin is undoubtedly correct, but I've never seen a pathologist write a report stating that it could be a false positive. One of the characteristics of the tumor edge in these circumstances is its rounded or curved appearance. Straight tumor borders coinciding with the surgical edge should really be interpreted as true compromised margins (Figure 7). In some cases, due to the architecture of the lesion, it is easier to imagine that this border is just coincidental (e.g. clearly nodular basal cell carcinoma). However, in micronodular, infiltrative cases or those with small blocks, it can be difficult to say that the margin is only coincidental, excluding the possibility of residual blocks remaining in the patient's surgical bed. For this reason, the histological subtype and the architectural pattern of the tumor should be highly valued in the interpretation.
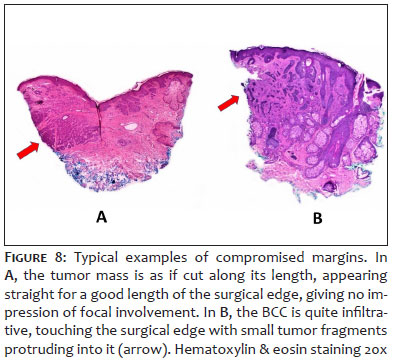
The margin is compromised when the surgical edge, which should be painted, coincides with the tumor edge, which is generally straight (i.e. giving the impression of having been cut). The tumor is otherwise quite infiltrative, so that digitiform projections of it appear sectioned at the surgical edge. Many pathologists do not mention the amount of tumor in the sections that touch the surgical edges, thus failing to distinguish even a possible case of a focal coincident margin as described above, from a case in which a large amount of tumor tissue affects the surgical edge. Surgeons who are aware of this situation may feel more confident about reoperating if they notice that a large amount of tumor tissue has touched the surgical edge (Figure 8).
A histopathological image is nothing more than a morphological analysis. The terminology used in histopathological language can be understood by associating its meaning with a pathology. For example, when the pathologist refers to "basaloid cells arranged in blocks with a palisaded periphery, surrounded by stromal retraction," we all interpret this as a description of basal cell carcinoma. But we really have no idea what the pathologist is actually describing (the image per se). We like to play this joke in lectures. Everyone knows palm trees, a mountain, a cove of white sand, a blue sky.... We immediately put all these elements together in a picture and imagine what is being described. Look at figure 9. It contains all these elements. Is that exactly how you imagined it? In other words, a picture is worth 5,000 words!
We all know that irregularly growing (infiltrative) tumors are more unpredictable in the way they expand, unlike expansive tumors, which tend to be more regular. This is important when it comes to surgical planning, i.e. whether or not we can use the safety margin concept correctly.1 Similarly to the imagery puzzle presented here, the pathologist's description may not fit very well with what the surgeon can perceive by examining the patient's clinical-surgical case and viewing the histopathological image directly. And if the pathologist describes the histological subtype of the tumor! Many reports lack this description, which can even be hampered by the type of material sent to the pathologist, such as fragmented or tiny biopsies.
It is very important to say that this text has absolutely no intention of instilling distrust in histopathology reports, but rather of drawing the attention of surgeons to the limitations that a pathologist may have in interpreting or describing them. Almost never have pathologists been upset that a doctor has asked to see the slides. On the contrary, most pathologists encourage this interaction. How often have we had productive conversations in favor of the patient's well-being when questions have been raised and resolved?
A close analogy is the interpretation of radiological images taken directly by orthopedists and the report issued by radiologists. In this case, we are dealing with known anatomy, unlike the abstract images of a histopathological image. The fact that orthopedists directly examine the image and only then quickly read the report cannot be interpreted as a sign of distrust of the radiologist's report.
It is a lot harder to write a text about this without being misunderstood than it is to talk about it in a lecture or to practice it for years. A concise and objective form that contains everything we have observed over years of practice is difficult to find. However, we believe that this short review can encourage the reader to embark on this journey and get used to examining the histopathology of their own cases. We are confident that you will see a lot that you had not expected and that you will be surprised that such disagreements in interpretation are not so rare. Observing the facts and seeking to understand them has always been the aim of science. If there are unanswered questions, what is wrong with raising them?
Another fact to be discussed is the scarcity of literature on the specific subject described here. Perhaps this has to do with the risk of being misinterpreted, as mentioned above. We are unaware of any publication with this clear objective and perhaps this article is original.
All this accumulated knowledge has come from our experience in micrographic surgery. More histotechnology and histopathological knowledge would be very useful for surgeons, which is precisely what micrographic surgeons do. We always encourage micrographic surgeons to make their own cuts and this is closely related to all the questions we are asking in this short review.
Finally, we would like to introduce the subject to give you a better understanding of the meaning of the term "compromised surgical margins". For most surgeons, this means further intervention, as most are unable to interpret a false positive. This review also has this objective: to encourage physicians to look a little further in order to better understand this phenomenon.
Luís Fernando Figueiredo Kopke
ORCID: 0000-0002-3350-5887
Approval of the final version of the manuscript; conception and planning of the study; drafting and writing of the manuscript; collecting, analyzing and interpreting data; intellectual participation in the propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Aira Novello Vilar
ORCID: 0000-0002-7458-9677
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studies cases; critical literature review; critical review of the manuscript.
1. Kopke LFF, Bastos JCF, Andrade Filho JS, Gouvêa PS. Margem de segurança: um conceito antigo e relativo. An Bras Dermatol. 2005;80(3):279- 86.
2. Goldwyn RM, Kasdon EJ. The "disappearance" of residual basal cell carcinoma of the skin. Ann Plast Surg. 1978;1(3):286-9.
3. Ministério da Saúde. Apoio ao diagnóstico e à terapia: anatomia patológica, hemoterapia e hematologia, medicina nuclear e patologia clínica. [Internet]. Brasília: Ministério da Saúde; 2014. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/apoio_diagnostico_terapia_a natomia_patologica.pdf.
4. Assis E. Manual de boas práticas em patologia da Sociedade Brasileira de Patologia. São Paulo: Livromed Paulista;2020. p.23-46.
5. Compton CC, Robb JA, Anderson MW. Preanalytics and precision pathology: pathology practices to ensure molecular integrity of cancer patient biospecimens for precision medicine. Arch Pathol Lab Med. 2019;143(11):1346‐1363.
6. Engel KB, Moore HM. Effects of preanalytical variables on the detection of proteins by immunohistochemistry in formalin-fixed, paraffin-embedded tissue. Arch Pathol Lab Med. 2011;135(5):537‐543.
7. Krajian AA, Gradwohl RBH. Histopathological technic. New York: Mosby;1952. p .28-56.
8. Serapião CJ, Serapião MJ, Santana LL. Curso intensivo de histotecnologia da Div.Nac.Câncer. Manaus: Div.Nac.Câncer;1976. Curso intensivo de histotecnologia;p. 32-44.
9. Rosai J. Rosai and Ackerman's surgical patology. 9th ed. New York: Mosby, 2004. p. 1304-1312.
10. Michalany J. Técnica histológica em anatomia patológica. São Paulo: E.P.U; 1980. p. 20-27.
11. Kopke LFF, Konz B. As diferenças fundamentais entre as variações da cirurgia micrográfica. An Bras Dermatol. 1994;69(6):505-10.
12. Gooding CA, White G, Yatsuhashi M. Significance of marginal extension in excised basal cell carcinoma. N Engl J Med. 1965;273(17):923-4.
13. Rosa IP. Posso falar? O caso é o seguinte. São Paulo: Lemar; 2013. p. 131.
14. Fidelis MC, Stelini RF, Staffa LP, Moraes AM, Magalhães RF. Carcinoma basocelular com margens comprometidas: estudo retrospectivo de condutas, evolução e prognóstico. An Bras Dermatol. 2021;96(1):17-26.
15. Richmond JD, Davie RM. The significance of incomplete excision in patients with basal cell carcinoma. Br J Plast Surg. 1987;40(1):63-7.
16. Kopke LFF, Schmidt SM. Carcinoma basocelular. An Bras Dermatol. 2002;77(3):249-85.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}