


Taciana Dal’Forno; Martina Souilljee Birck
Financial support: None.
Conflict of interest: None.
Submitted on: 07/25/2023
Final decision: 02/07/2024
How to cite this article: Dal'Forno T, Birck MS. A novel neck rejuvenation protocol using a combination of injectables and technologies in a single session. Surg Cosmet Dermatol. 2024;16:e20240283.
Neck aging encompasses intrinsic and extrinsic factors that need to be understood in order to achieve good treatment outcomes in the area. Minimally or noninvasive methods for neck rejuvenation have gained popularity because they provide individualized, natural, and safe results with no downtime. However, few studies have debated the need for global neck treatment or have offered suggestions and ways to combine different methods in single or multiple sessions.
We report here a novel protocol with the combined use of injectables and technologies in a single session, which act on laxity, fine lines, wrinkles, and skin quality.
Keywords: Neck; Rejuvenation; Combined Modality Therapy.
The combination of minimally invasive procedures in cosmiatry, for patients unwilling to undergo a surgical procedure, aims to provide significant results without scarring and with rapid recovery, safety, and satisfaction. For treatments related to neck rejuvenation, this is no different: more and more patients are looking for alternatives to more invasive treatments. Based on this demand, different methods have been used alone or combined to meet individual treatment expectations, such as injectable agents (botulinum toxin [BTX], hyaluronic acid [HA], poly-L-lactic acid [PLLA], calcium hydroxylapatite [CaHA]), radiofrequency (RF), RF microneedling (RFMN), microfocused ultrasound (MFU), intense pulsed light, and lasers.1
Signs of aging, such as laxity and wrinkles, are typically more intense on the neck than other parts of the body and are particularly more visible in patients who have already undergone facial procedures. Complaints related to the neck, such as increased submental fat, loss of contour, laxity, fine wrinkles, and changes in skin texture, are very common and encourage patients to seek procedures capable of addressing them.2
The present study aims to report the results of a series of cases in which a novel protocol with a combination of injectables and technologies in a single session was used for neck rejuvenation, the so-called "TD Protocol," aiming to improve outcomes and optimize the patient's time.
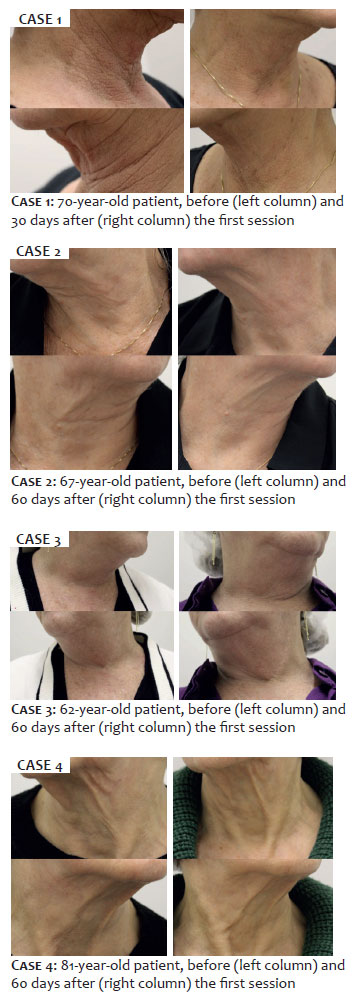
Four female patients, aged 62 to 81 years, were subjected to the single-session protocol. High-resolution digital photographs of the neck were taken before and 30 to 60 days after the protocol. Topical anesthesia (Dermomax®, Aché, Brazil) was applied in all patients for 20 minutes prior to the procedures.
The protocol includes the following treatments in a single session and in the following order:
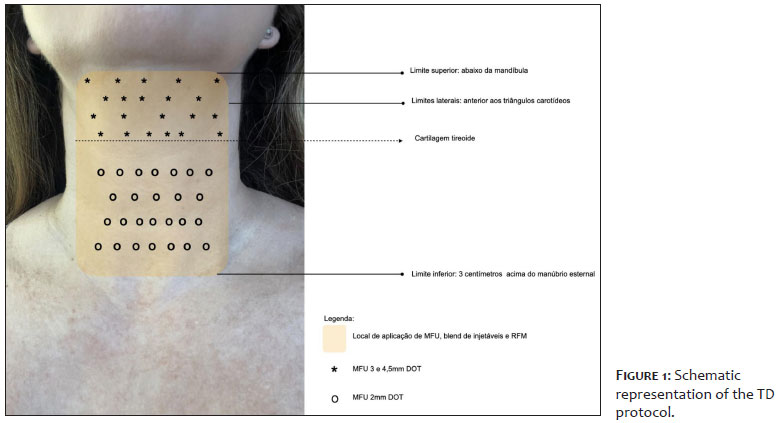
• Application of MFU (UltracelQ+®, Jeisys, South Korea) at a focal depth of 2 mm with up to 120 lines on the anterior aspect of the neck and focal depths of 3.0 and 4.5 mm in the submandibular area, cranial to the thyroid gland, between 120 and 200 lines from each tip;
• Application to the anterior rectangle of the neck, in retroinjection with a 22G 70 mm cannula, of the following mixture in the same 10 mL syringe: one 1.5 mL ampoule of CaHA (Radiesse Duo®, Merz, Germany), 20 units of BTX (Xeomin®, Merz, Germany), 1 mL of HA 20 mg/mL (Belotero Balance®, Merz, Germany), 1 mL of 1% lidocaine without vasoconstrictor, and 2.5 mL of 0.9% saline solution, for a total volume of 6 mL to be injected – modification of technique previously described.3
• Application of RFMN (Eletroderme®, LMG, Brazil) at 3 different depths (2.5, 2.0, and 1.5 mm), with energy of 25, 20, and 15 J and pulse duration of 130, 120, and 110 ms, respectively, complemented by 2 additional passes with the RF turned off and with a needle depth of 1.8 mm.
Figure 1 provides a schematic representation of the application of the TD Protocol.
All patients had improvement in skin laxity and quality based on the analysis of photographs taken before and 30 to 60 days after the procedures and reported high satisfaction with the results. Patients had moderate erythema after application, lasting about 6 hours, and mild erythema and bruising for up to 7 days. Notably, patients reported no pain during RFMN.
Understanding the intrinsic and extrinsic factors of the aging process is essential for a comprehensive approach in treatments for neck rejuvenation. To obtain optimal outcomes, studies have demonstrated that a combination of the multiple minimally invasive procedures available is superior to their use alone.4
Regarding the noninvasive methods used in this study, it is known that MFU is widely used to treat skin laxity,5 minimizing the appearance of submental fat accumulation,6 as it induces thermal damage – coagulative necrosis – precisely targeting the superficial dermis and subcutaneous tissue, thus protecting the epidermis and promoting collagen remodeling in the desired area5. Edema and erythema may occur after MFU application.6 Several studies have reported better results with the combined use of this technology and collagen biostimulators, such as CaHA in the short and long term, with current consensus that CaHA should be applied after MFU, based on the assumption that the microspheres left by MFU-induced thermal damage act as a scaffold for new tissue formation, enhanced after injection of the biostimulator.7
Attenuation of platysmal bands can be achieved with the use of BTX, with more visible effects in younger patients, as it does not improve laxity or submental fat.8 When using BTX in conjunction with other therapies, the timing of injection should be considered. For example, it is recommended that BTX be used 3 weeks after using ablative lasers, but it can be performed immediately after vascular/pigment laser treatment with MFU if there is minimal edema after ultrasound. To enhance the correction of neck lines, the use of dermal fillers, such as HA, can be added to the treatment. When combining this with BTX, it is recommended to inject HA before BTX. HA use is safe immediately after vascular lasers and MFU, but its simultaneous use, on the same day, with ablative or nonablative fractional lasers should be avoided, especially on the face.9 Finally, RFMN produces cell heating through the movement of molecules in a specific tissue using a matrix of needles, leading to collagen denaturation and tissue contraction, thereby promoting dermal remodeling through neocollagenesis. The most common adverse effects include erythema, edema, and pain, alleviated by using topical or injectable anesthetics. Therefore, the use of topical anesthesia and the injectable blend, administered in conjunction with lidocaine before RFMN, reduces patient discomfort in this method. Unlike lasers, RFMN can be used in any skin type as it does not act on specific chromophores, thus being safe in patients with darker skin types.10 Regarding the present protocol, it is under debate whether RFMN used after an injectable agent, such as BTX, could reduce its effect due to the heat generated at the site. Further studies should be conducted to evaluate the efficacy and safety of the protocol described here for neck rejuvenation, as well as its histologic effects.
Although surgical facelift remains the gold standard treatment to correct neck laxity, the intensive search for novel, less invasive interventions has demonstrated that cosmetic procedures are safe and effective for rejuvenation of the neck. Combining different methods can individualize and enhance outcomes, but there are still few studies evaluating multiple combinations in a single session. This protocol provides, for the first time, visible and safe results after sequentially performing, on the same day, well-established cosmetic procedures associated with 5 different methods, including injectables and technologies, in the single-session treatment of neck aging.
Taciana Dal'Forno
ORCID: 0000-0003-0848-9042
Approval of the final version of the manuscript; conception and design of the study; preparation and writing of the manuscript; acquisition, analysis and interpretation of data; effective participation in the conduct of the study; intellectual participation in propaedeutic and/or therapeutic approach to studied cases; critical revision of the manuscript.
Martina Souilljee Birck
ORCID: 0000-0001-92817744
Conception and design of the study; preparation and writing of the manuscript; critical review of the literature.
1. Melo F, Carrijo A, Hong K, Trumbic B, Vercesi F, Waldorf HA, et al. Minimally invasive aesthetic treatment of the face and neck using combinations of a PCL-based collagen stimulator, PLLA/PLGA suspension sutures, and cross-linked Hyaluronic Acid. Clin Cosmet Investig Dermatol.2020;13:333-344.
2. Vanaman M, Fabi SG, Cox SE. Neck rejuvenation using a combination approach: our experience and a review of the literature. Dermatol Surg.2016; 42(Suppl 2):S94-S100.
3. Pecora CS. The gold protocol: A combined treatment approach for neck rejuvenation with calcium hydroxyapatite, botulinum toxin, and hyaluronic acid in the same session. J Cosmet Dermatol. 2024;00:1–9.
4. Mokhallalati AM, Sada R, Badran S, Zahid R, Mohammedali S, Mostafa S, et al. Non- surgical neck contouring. Cosmetol J.2018, 2(2):000111.
5. Khan U, Khalid N. A systematic review of the clinical efficacy of micro-focused ultrasound treatment for skin rejuvenation and tightening. Cureus 2021;13(12):e20163.
6. Doh EJ, Kim J, Lee DH, Paík JY. Neck rejuvenation using a multimodal approach in Asians. J Dermatolog Treat. 2018;29(4):400-404.
7. Casabona G, Teixeira DN. Microfocused ultrasound in combination with diluted calcium hydroxylapatite foí improving skin laxity and the appearance of lines in the neck and décolletage. J Cosmet Dermatol 2018;17(1):66-72.
8. Jabbour SF, Kechichian EG, Awaida CJ, Tomb RR, Nasr MW. Botulinum toxin for neck rejuvenation: assessing efficacy and redefining patient selection. Plast Reconstr Surg. 2017;140(1):9e-17e.
9. Dal'Forno T, Mazzuco R, Hexsel D. Reports of potencial botulinum toxin spread in inflamed tissue. Dermatol Surg. 2020;46(8):1125-1127.
10. Alessa D, Bloom JD. Microneedling options for skin rejuvenation, including non- temperature-controlled fractional microneedle radiofrequency treatments. Facial Plast Surg Clin North Am.2020;28(1):1-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}