


Vivian de Carvalho Amaral
Funding: None.
Conflicts of interest: None.
Submitted on: 23/04/2023
Accepted on: 07/02/2024
How to cite this article: Amaral VC. Systematization of labia majora augmentation with hyaluronic acid filler: the vulvar anatomical vector technique. Surg Cosmet Dermatol. 2024;16:e20240253.
Despite the therapeutic success described by recent studies, the procedure of labia majora augmentation lacked systematization in order to achieve more assertive and reproducible results. To this end, we developed the vulvar anatomical vector technique, in which we mapped five anatomical structures of the vulva where the injection of hyaluronic acid is capable of promoting coaptation, augmentation, reduction of prolapse, and/or improvement of the skin quality of the labia majora. This technique has allowed us to precisely define the sites to be injected and estimate the adequate volume and type of hyaluronic acid to achieve the intended results.
Keywords: Hyaluronic Acid; Vulva; Dermal Fillers; Rejuvenation; Female Genitalia.
The injection of cross-linked hyaluronic acid (HA) for augmentation of the labia majora (LM) has been employed with excellent results and low complication rates.1-4 Despite the therapeutic success reported in recent studies, the procedure lacked systematization to determine the best products and methods to achieve reproducible results.4 Since 2019, we have successfully used a technique for LM augmentation with HA fillers, termed vulvar anatomical vectors, with the aim of ensuring that, after individual assessment, the procedure can be performed safely and effectively.
Four key aspects need to be assessed before LM augmentation, namely:
• LM coaptation: Prolapse of the labia minora and the clitoris are common complaints, which may result from hypertrophy of the labia minora and clitoris or hypotrophy of the LM. If the LM are hypotrophic, their coaptation via filling may reduce prolapse of the labia minora and clitoris.
• LM augmentation: Loss of volume in the LM can cause laxity and wrinkling.
• LM tone: Loss of tone in the area between the LM and the suprapubic region, along with loss of volume, can cause sagging of the LM.
l LM wrinkling.
Eighty-six women aged 27 to 66 years with complaints of LM laxity, wrinkling, and prolapse of the labia minora and clitoris received injections of HA filler. All participants were evaluated and photographed before and immediately after the procedure. Follow-up was conducted at 30 and 180 days.
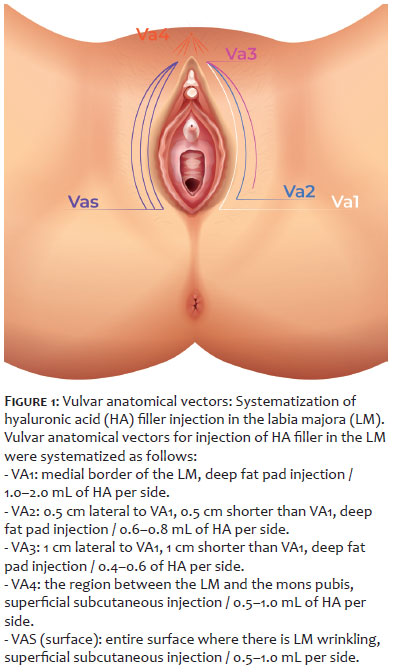
Injection of HA filler in the LM was systematized according to the vectors and amounts injected per side as follows (Figure 1):
VA1: medial border of the LM, deep fat pad injection / 1.0–2.0 mL.
VA2: 0.5 cm lateral to VA1, 0.5 cm shorter than VA1, deep fat pad injection / 0.6–0.8 mL.
VA3: 1 cm lateral to VA1, 1 cm shorter than VA1, deep fat pad injection / 0.4–0.6 mL.
VA4: the area between the LM and mons pubis, superficial subcutaneous injection / 0.5–1.0 mL.
VAS (surface): entire surface where there is LM wrinkling, superficial subcutaneous injection / 0.5–1.0 mL.
First, asepsis and antisepsis of the selected area were performed, followed by injection of 1% lidocaine. Then, punctures were made with a 21-gauge needle to insert a 22-gauge 70 mm disposable cannula for the filler injections.
In vectors VA1, VA2, VA3, and VAS, punctures were made at the upper limit of the LM bilaterally, and multiple small boluses of HA were injected using the retrograde technique. In VA4, a puncture was made approximately 2 cm above the anterior labial commissure, and a retrograde injection of HA in the superficial subcutaneous tissue was performed using the fanning technique.
We used cross-linked products with an HA concentration of 20 mg/mL, while products with a lower G prime were used in the VAS vector. No more than 3.0 mL was injected into each side of the LM in a single session. In most cases, 2 mL was injected into each side, and the need to increase the volume was reevaluated after 30 days. Subsequent fillings were performed every 12 months.
The filling procedures yielded the following results according to each vector:
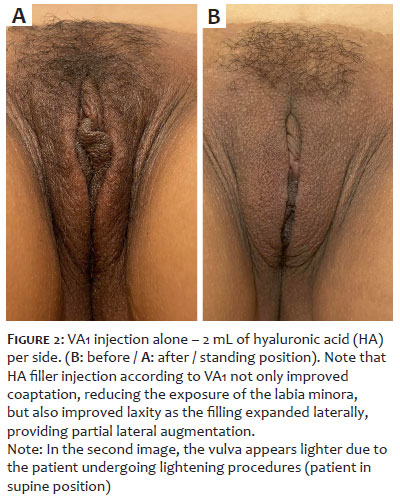
VA1: increased coaptation of the LM, with better accommodation of the clitoris and the labia minora (Figure 2).
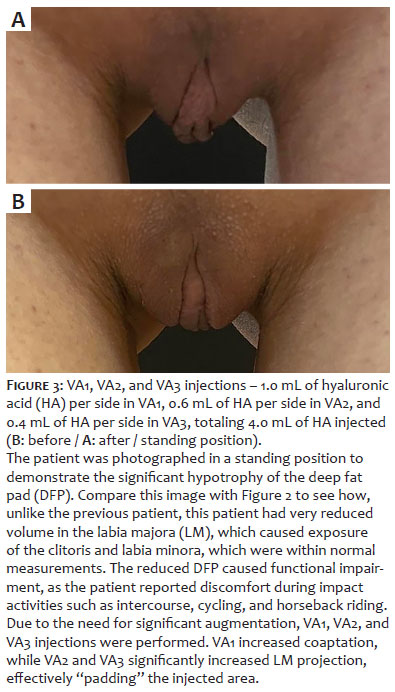
VA2 and VA3: adequate augmentation with increased anterior projection of the LM; well-suited for treating LM laxity (Figure 3).
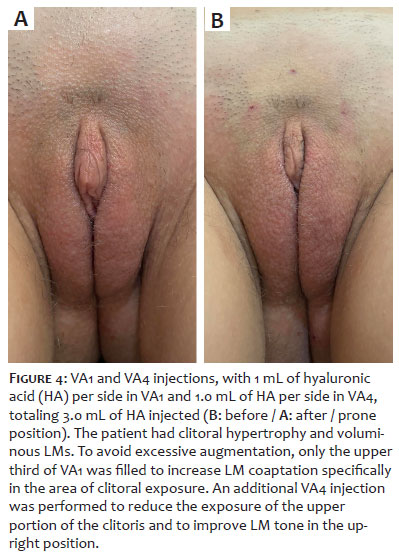
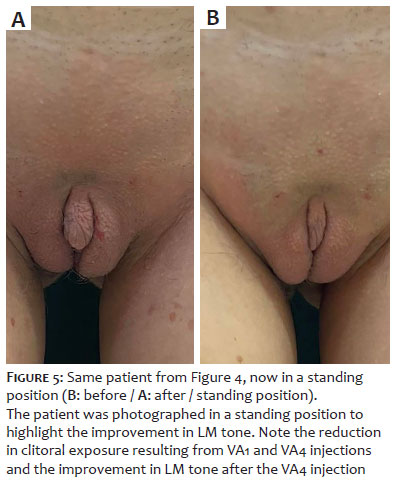
VA4: increased LM tone and reduced visibility of the superior limit of the clitoris when hypertrophic (Figures 4 and 5).
VAS: reduced wrinkling (Figure 6).
Some complications were observed among participants, including biofilm formation 14 days after the procedure due to a wound caused by waxing, promptly treated with oral antibiotics without further complications. In addition, four cold nodules due to accumulation of product were observed and easily resolved with vigorous massage of the affected area. Finally, small bruises at the entry points and local edema also occurred but resolved within 7 days. There were no cases of intravascular injection.
LM and labia minora dimensions are extremely variable. To avoid over or undertreatment, we considered the dimensions below5 as reference:
Length: LM 7–8 cm / labia minora 3–3.5cm
Width: LM 2–3 cm / labia minora 1–1.5 cm
VA1 injections in patients with LM length > 8 cm were avoided to prevent the distal portion of the LM from becoming saggy. If the area remained wrinkled, the patient was reevaluated after 30 days, and VAS injection was performed with a low-G prime product or collagen biostimulators if necessary.
Patients with significant hypertrophy of the clitoris or labia minora (> 3 cm), grades 2 and 3 by the Colaneri classification,6 were not treated. In these cases, injection of HA filler would not coapt the vulva and could result in excessive augmentation.
The LM are two large cutaneous folds of adipose, connective, and muscle tissue that extend from the mons pubis to the perineum. The adipose tissue is divided into superficial subcutaneous tissue (SST) and deep fat pad (DFP). The SST extends anteriorly toward the pubis as a thick layer of fat, continuous with the SST of the mons pubis, and posteriorly toward the perineum as Dartos fascia, composed of smooth muscle fibers.
SST and DFP are separated by a fibrous tunic, which projects itself from the inguinal canal in a finger-like shape, containing DFP and forming the suspensory ligament of the clitoris. The anatomy of the DFP is closely linked to the inguinal canal, an area that must be protected from contamination. The inguinal canal connects the genital area to the abdominal cavity and conveys the round ligament of the uterus, ilioinguinal nerve, genital branch of the genitofemoral nerve, and blood and lymph vessels.
Because the tissue is very thin, injections in the SST are performed to reduce skin wrinkling but not to increase volume. Therefore, the coaptation and volumizing vectors (VA1, VA2, and VA3) should be done in the DFP, while the VAS vector, which aims to improve skin quality, should be done in the SST.
It is also important to note that VA2 and VA3 injections should not be performed without prior VA1 injection to avoid lateral augmentation from causing LM separation and increased exposure of the clitoris and labia minora. In fact, the natural accommodation of HA in the DFP often means that VA1 injection alone will achieve the desired results without additional injections in VA2 and VA3.
The vulva is supplied by the anterior labial arteries, branches of the external pudendal arteries, posterior labial arteries, and branches of the internal pudendal arteries. To avoid intravascular injection, a thorough understanding of this vascular anatomy is essential, and care should be taken to proceed with prior aspiration and slow, gentle injection. We also use large caliber, blunt-tip cannulas.
HA filler injection in the LM is an excellent technique for beautifying the female genitalia, delivering outstanding results with few complications. We propose a reproducible systematization of the procedure, which takes into account patient complaints and the adequate anatomical sites to be treated, achieving a high therapeutic success rate.
Vivian de Carvalho Amaral
ORCID: 0000-0002-5379-652X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
1. Zerbinati N, Haddad RG, Bader A, Rauso R, D'Este E, Cipolla G, et al. A new hyaluronic acid polymer in the augmentation and restoration of labia majora. J Biol Regul Homeost Agents. 2017;31(2 Suppl.2):153-61.
2. Jabbour S, Kechichian E, Hersant B, Levan P, El Hachem L, Noel W, et al. Labia majora augmentation: a systematic review of the literature. Aesthet Surg J. 2017 16;37(10):1157-64.
3. Hexsel D, Dal'Forno T, Caspary P, Hexsel CL. Soft-tissue augmentation with hyaluronic acid filler for labia majora and mons pubis. Dermatol Surg. 2016;42(7):911-4.
4. Fasola E, Gazzola R. Labia majora augmentation with hyaluronic acid filler: technique and results. Aesthet Surg J. 2016;36:1155-63.
5. Kreklau A, Vâz I, Oehme F, Strub F, Brechbühl R, Christmann C, et al. Measurements of a 'normal vulva' in women aged 15-84: a cross-sectional prospective single-centre study. BJOG. 2018;125(13):1656-61.
6. Colaneri AGF. Nova classificação para hipertrofia dos pequenos lábios vaginais e correlação com as técnicas cirúrgicas indicadas. Rev Bras Cir Plást.2018;33(1):64-73.
7. Fulton J, Caperton C, Weinkle S, Dewandre L. Filler injections with the blunt-tip microcannula. J Drugs Dermatol. 2012;11(9):1098-103.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}