


Cláudia Borges Fontan1; Juliana Borges Fontan2; Juliana Paulos de Rezende3; Luciana Carmen Zattar4; Américo Mota5,6
Submitted on: 14/09/2023
Accepted on: 14/02/2024
Funding: None.
Conflicts of interest: None.
How to cite this article: Fontan CB, Fontan JB, Rezende JP, Zattar LC, Mota A. Ultrahigh-frequency ultrasound imaging of the dorsum of the hand for aesthetic procedures. Surg Cosmet Dermatol. 2024;16:e20240300.
Hand rejuvenation has become increasingly popular in recent years. Knowledge of the layered anatomy of the hand is crucial for better aesthetic results. In this context, ultra-high-frequency ultrasound (UHFUS) has been used in minimally invasive procedures all over the body, including the hands. To the best of our knowledge, this is the first study to correlate UHFUS evaluation of the dorsal aspect of the hand before, during, and after injectable procedures. We discuss the layered local anatomy of the hand, whose knowledge is crucial for performing safe and effective aesthetic treatments for rejuvenation, and the correlation of the imaging aspects of different procedures and products, as well as its possible complications.
Keywords: Ultrasonography; Rejuvenation; Hand; Anatomy.
After the face, the hands are one of the most visible parts of the body, and undergo characteristic changes with aging, such as dyschromias, lentigines, actinic and seborrheic keratosis and roughness. In addition, loss of subcutaneous fat volume and muscle atrophy accentuate the prominent tortuous veins, tendons, joints, and bony prominences beneath the skeletal skin of the dorsum of hand.1,2 All of these changes contribute to an older appearance. The literature shows that patient age may be estimated based solely on the appearance of the hands.1 Indeed, the appearance of the hands is also considered the second most telling indicator of chronological age, surpassed only by the appearance of the face.3 Hand rejuvenation procedures have therefore received special attention.
Hand rejuvenation for aesthetic purposes has become increasingly popular among both professional injectors and patients 4,5 seeking to restore the appearance of smooth, youthful hands with satisfactory volume and improved skin quality. To achieve the best results with these emerging aesthetic and cosmetic procedures, a thorough understanding of the local anatomy, accurate determination of the precise anatomical plane of application, and familiarity with the composition and properties of the products used, as well as the proper procedural techniques, are essential.
High-resolution ultrasound (HRUS) may be used to improve safety and accuracy prior to, during, and after these procedures. Ultrahigh-frequency ultrasound (UHFUS) has become increasingly popular for minimally invasive procedures. This is not only because of its unprecedented level of detail, which allows identification of structures previously unimaginable with radiological imaging techniques, but also because it correlates in vivo anatomical, clinical, surgical, and radiological findings with incredible precision.
Although the hands are highly visible, aesthetic procedures are popular, and UHFUS has potential, there are relatively few studies regarding hand rejuvenation. Very few of these studies have used radiological imaging, and none have included detailed anatomical and procedural information along with the use of UHFUS (22–33 MHz).6,7,8
Therefore, the aim of this article is to describe the techniques and procedures performed on the hands as well as the associated imaging findings and detailed anatomy of the hands, thereby adding an innovation to the literature.
Knowledge of the layered anatomy of the hand is crucial for a successful preprocedural and ultrasound analysis. This knowledge is also essential for safe and effective aesthetic treatments, as performing procedures in the wrong anatomical layer can lead to poor aesthetic outcomes and increase the risk of adverse events, such as hematoma formation, intravascular injection, and nerve damage.
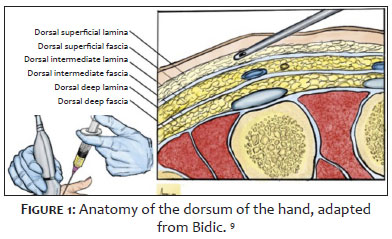
The first anatomical discussion of the dorsum of the hand was in 1939 by Kanavel,9 who described two fasciae: a superficial fascia covering the extensor tendons and a deep fascia covering the interosseous muscles and metacarpal bones. In 2010, Bidic et al.9 correlated histological, anatomical, and ultrasound sections of the dorsum of hand and described three compartments of areolar fatty tissue and three fascial layers. They identified the dorsal superficial, intermediate, and deep laminae, separated by three fascial layers: i) dorsal superficial fascia, which separates the dorsal superficial lamina from the dorsal intermediate lamina; ii) dorsal intermediate fascia (a continuation of the antebrachial fascia of the forearm), which separates the dorsal intermediate lamina from the dorsal deep lamina; and iii) dorsal deep fascia, the muscular fascia that extends from the periosteum on the dorsal side of the metacarpals. The sensory nerve and the dorsal vein are in the dorsal intermediate lamina, and the extensor tendon is in the dorsal deep lamina (Figure 1).
Studies in the last decade have also adopted this layered anatomy approach. For example, Lefebvre-Vilardebo et al.10 describe the fascia and laminae between the skin and tendons as inseparable, forming a 3D sponge-like fascial scaffold in which veins, their perforators, and nerves are found. The studies by Bidic et al.9 and Lefebvre-Vilardebo et al.10 agree that the safest layer for application of volumizing material is the subdermal layer because it is at a safe distance from the neurovascular bundle. Dorsum of hand is compartmentalized by strong septa, so bolus injection of product is less likely to be easily redistributed throughout the dorsum of hand.2
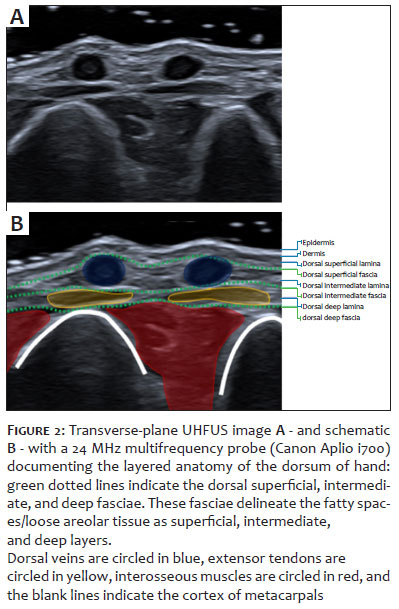
To the extent of our knowledge, after an extensive search of the medical literature, this is the first study of the ultrasonographic anatomy of the dorsum of the hand using UHFUS (22 MHz—GE LOGIC E, General Electric, Milwaukee, WI; and 24 and 33 MHz—Canon Aplio i700 and i800, Canon Medical System Corporation, Japan). By using UHFUS, we found consistency in the ultrasound imaging patterns of the dorsal layers of hand. From surface to deeper layers, the following layers can be identified (Figure 2):
Epidermis: Thin hyperechoic line due to higher keratin content.
Dermis: Hyperechoic band (less hyperechoic than the epidermis), rich in collagen.
Dorsal superficial lamina: Thin hypoechoic band, a very thin layer of fat/areolar tissue, generally not noticeable.
Dorsal superficial fascia: Hyperechoic line.
Dorsal intermediate lamina: Hypoechoic band, a layer of areolar fatty tissue where the dorsal veins are located (oval anechoic structures in the transverse plane and tubular in the longitudinal plane).
Dorsal intermediate fascia: Hyperechoic line, a continuation of the antebrachial fascia of the forearm.
Dorsal deep lamina: Hypoechoic band, a layer of fat/areolar tissue in which the extensor tendons run.
Dorsal deep fascia: Hyperechoic line, the superficial muscular fascia that continues to the periosteum of the dorsal surface of the metacarpals.
By reviewing the literature, we can see that the studies by Bidic et al.9 and by Lefebvre-Vilardebo et al.10 present different descriptions of the anatomy of the fascia and laminae of hand. However, this discrepancy can be attributed to their use of transducers with different frequencies and lower resolutions than those used in the present study.
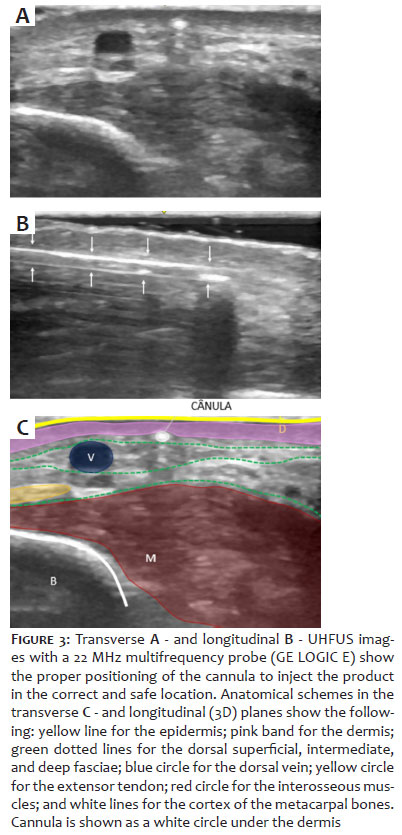
Understanding the layered anatomy of the dorsal hand and its normal appearance on ultrasound is critical to performing injectable aesthetic procedures, not only in preprocedural evaluation but also in guided injections. The recommended target plane for hand rejuvenation injections is the undersurface of dermis, which can be clearly identified via UHFUS. During evaluation, it is also possible to visualize and confirm the proper positioning of the cannula, which appears as a round hyperechoic structure in the transverse plane and tubular in the longitudinal plane (Figure 3).
Hand rejuvenation is a safe, effective procedure. The first study identified in the literature on dorsal hand rejuvenation was published in 1992 and reported results with fat grafting.11 Since that time, a variety of techniques have been described with similar aesthetic results.3 Major techniques for hand rejuvenation include autologous fat transfer (transfer of the patient's own fat), dermal fillers (synthetic materials), and collagen stimulants. Currently, only two fillers are U.S. Food and Drug Administration-approved for hand rejuvenation: Radiesse® (CaHA; Merz North America, Inc., Raleigh, NC) and Restylane-Lyft® (hyaluronic acid; Galderma Laboratories, Fort Worth, TX).7
All of these procedures can be performed with local anesthesia, provide good aesthetic results, and patients report high satisfaction with fewer complications.7 A systematic review showed that Radiesse® and fat grafting were the most commonly used products for hand rejuvenation with the lowest complication rates.3
Ultrasound can be used before procedures to analyze local anatomy and identify previously applied products, an important step in reducing risk. Ultrasound is the only radiological imaging modality capable of being used for product identification or during and after injections. In postprocedural assessment, this method can diagnose and assist in the management of aesthetic and surgical complications.12,13
Once fat is obtained, it is possible to fill the dorsal region of the hand, allowing it to cover visible veins and tendons, resulting in subtle and uniform contours. In addition to the volumizing effect, the fat cells have a beneficial stemming effect, with growth factors that rejuvenate the superficial and deep tissues. The results are stable and, in the long term, the effects and aesthetic satisfaction can last more than 4 to 5 years.
Liposuction sites, material preparation protocols, and injected volumes vary in the literature. The body regions most involved in the harvesting of autologous fat for grafting include the abdomen, flanks, and medial thigh. There was no consensus on centrifugation prior to injection. The fat grafting technique is most commonly performed with cannula, with low pressure, low speed, low volume, multi-tunnels, multi-planes, and multi-points (3L3M). Volumes ranges from 10 to 30 mL, with a total average of 15 mL per hand, using a proximal to distal fan technique.8,11 The exact anatomical layer in which the fat cells are deposited is controversial; there is a greater consensus on the safety and efficacy of injections into the dorsal superficial lamina.11
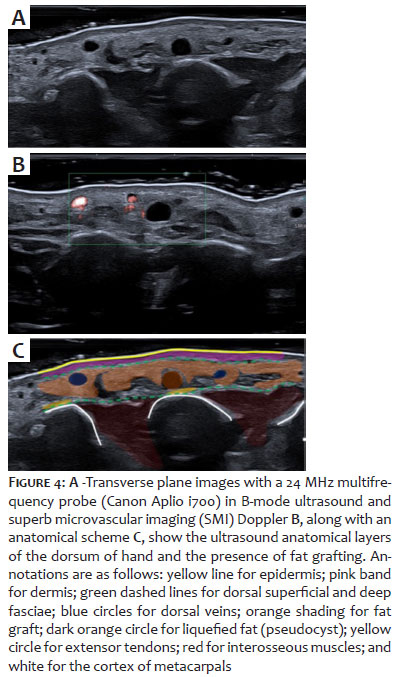
In UHFUS, the main characteristics of autologous fat grafts depend on the preparation or composition: whether when liquefied it appears as anechoic or a "pseudocystic" deposit,14 or if not liquefied, as a local tissue disorganization or lobulated hypoechoic deposits with permeating hyperechoic septa (Figure 4).
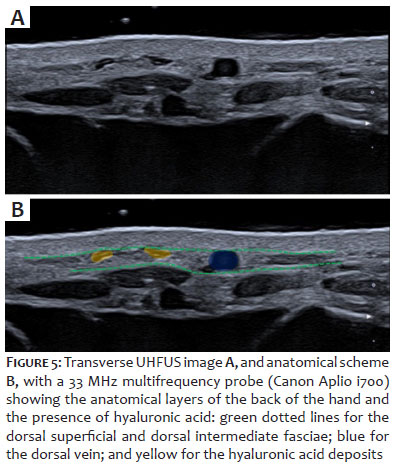
Hyaluronic acid can improve the appearance of wrinkles, provide optimal coverage of prominent veins and visible tendons, and improve subcutaneous atrophy. Typically, 1 ml of hyaluronic acid is used on each side. Results last approximately 12 months.15,16,17,18
In the ultrasound image (Figure 5), the appearance of hyaluronic acid depends on its composition, combination, and density. Pure hyaluronic acid (HA) appears as millimeter-sized anechoic, "pseudocystic" areas.19
Injectable poly-L-lactic acid (PLLA) (SCULPTRA® Aesthetic, Galderma Laboratories) is a semipermanent, biocompatible, biodegradable, immunologically inert product. The induction of neocollagenesis by fibroblasts results from the placement of PLLA in the reticular dermis and subcutaneous tissue planes. Results last up to 2 years, sometimes longer.20
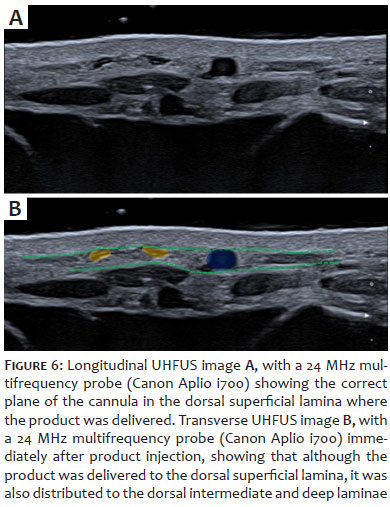
Redaelli described the first series of PLLA cases for hand rejuvenation in 2006. He observed a measurable decrease in the visibility of extensor tendons and an improvement in the appearance of tortuous veins. In the 16 patients available for evaluation at 15 months, results were maintained or improved.21 In UHFUS, PLLA is generally difficult to detect unless it forms nodules, which may or may not be palpable and may present as isoechoic or slightly hyperechoic nodules. With direct application of the product diluted in distilled water, only the anechoic aspect of the diluent infiltrating the tissue can be identified (Figure 6). With ultrasound-guided application of PLLA on the dorsal superficial lamina, we observed its delivery also to the dorsal intermediate and deep laminae, similar to the 3D model reported by Lefebvre-Vilardebo et al.2,10 (Figures 6a and 6b).
In 2007, Busso and Applebaum22 first described the use of calcium hydroxyapatite (CaHA) (Radiesse, Merz Aesthetics) to restore a fuller, more youthful appearance to the hands, reduce skin laxity and wrinkles, and minimize the appearance of prominent underlying structures such as bone, tendons, and veins. Because CaHA is an identical compound to that found in bone, it has high biocompatibility and a low risk of adverse events.
Since that initial report by Busso and Applebaum, additional publications have demonstrated successful restoration of the volume of hand with CaHA in over 100 patients using a variety of techniques and dilutions. Results have ranged from 12 to 24 months.23,24,25
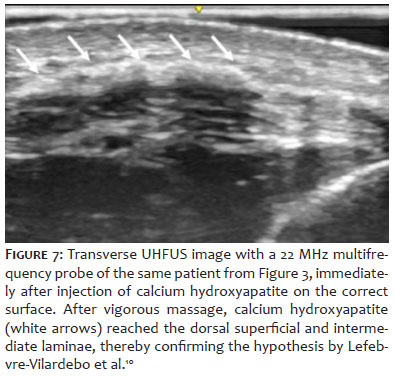
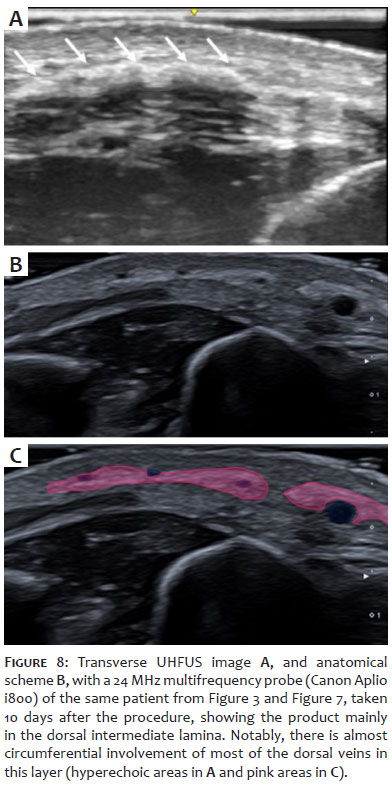
On HRUS, CaHA appears as continuous or focal hyperechoic deposits with or without posterior acoustic shadowing, depending on the concentration (Figure 7 and Figures 8a and 8b).26 On UHFUS, it appears as continuous or focal hyperechoic deposits with or with no posterior acoustic shadowing, depending on the concentration (Figure 7 and Figure 8).27
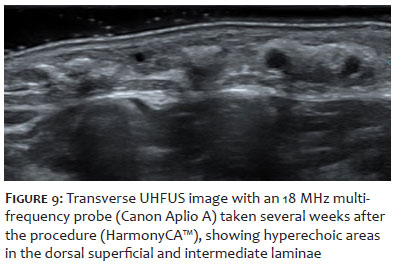
HArmonyCa™ (Allergan Aesthetics, an AbbVie Company) is a hybrid filler that combines the collagen biostimulant calcium hydroxylapatite (55.7%) plus the hyaluronic acid volumizer.28 On UHFUS, it appears as hyperechoic areas with a cloudy pattern without posterior acoustic shadowing22 (Figure 9).
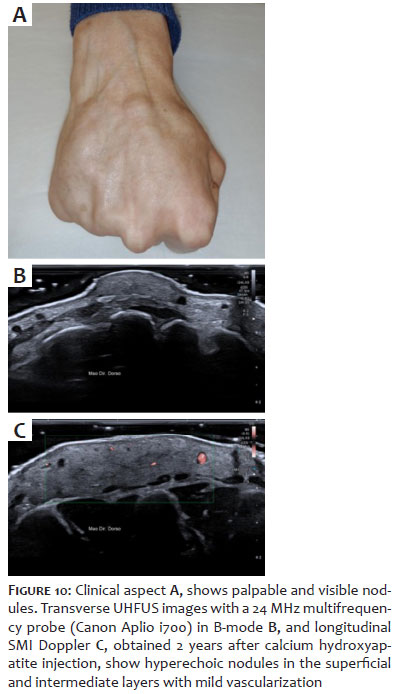
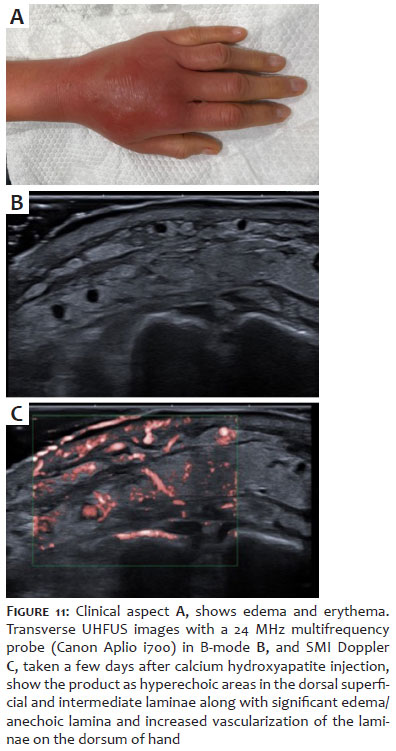
The two most common side effects reported after injectable procedures are hematoma and edema, which are typically mild, transient, and resolve spontaneously within a few days or weeks.7 Ecchymosis and paresthesia have also been reported and can be minimized with the use of cannulas and ultrasound-guided procedures.11 Potential long-term complications include persistent edema, sensory dysfunction, and the formation of nodules or foreign body granulomas7 (Figure 10). More serious complications include local infections that may progress to abscesses11 (Figure 11).
Hand rejuvenation has become an increasingly popular procedure because it is a safe and effective method. Different techniques and products are described with similar results.3 Knowledge of the anatomy is critical for injectors to ensure accurate and safe placement of fillers and collagen stimulators on the dorsum of hand.7 UHFUS can assist before the procedure by identifying previously applied products and providing detailed anatomy. During the procedure, UHFUS can guide application of product in the correct layer, avoiding veins and nerves. After the procedure, it can help manage complications.
Comprehensive knowledge of anatomy, product characteristics, and procedural techniques, as well as the ability to evaluate ultrasound at multiple levels (prior to, during, and after procedure), is important for the safe, effective application of all aesthetic hand rejuvenation procedures.
Cláudia Borges Fontan
ORCID: 0000-0002-9687-425X
Approval of the final version of the manuscript; study design and planning; manuscript drafting and writing; critical review of the literature; critical review of the manuscript.
Juliana Borges Fontan
ORCID: 0009-0004-8305-7797
Manuscript design and writing; critical review of the manuscript.
Juliana Paulos de Rezende
ORCID: 0009-0008-3737-9890
Approval of the final version of the manuscript; drafting and writing the manuscript; critical review of the literature; critical review of the manuscript.
Luciana Carmen Zattar
ORCID: 0000-0002-5229-8596
Approval of the final version of the manuscript; active participation in the conduct of the research; critical review of the literature; critical review of the manuscript.
Américo Mota
ORCID: 0000-0003-0477-8330
Approval of the final version of the manuscript; critical review of the manuscript.
1. Bains RD, Thorpe H, Southern S. Hand aging: patients' opinions. Plast Reconstr Surg. 2006;117(7):2212–8.
2. Frank K, Koban K, Targosinski S, Erlbacher K, Schenck TL, Casabona G, et al. The anatomy behind adverse events in hand volumizing procedures: retrospective evaluations of 11 years of experience. Plast Reconstr Surg. 2018;141(5):650e–62e.
3. McGuire C, Boudreau C, Tang D. Hand rejuvenation: a systematic review of techniques, outcomes, and complications. Aesthetic Plastic Surgery. Springer. 2022;46:437–49.
4. Fathi R, Cohen JL, Robins P. Challenges, considerations, and strategies in hand rejuvenation. J Drugs Dermatol. 2016;15(7):809-815.
5. Dissecting the dorsal laminae. (n.d.).
6. Park TH, Yeo KK, Seo SW, Kim JK, Hee JH, Park H, et al. Clinical experience with complications of hand rejuvenation. J Plast Reconstr Aesthet Surg. 2012;65(12):1627–31.
7. Har-Shai L, Ofek SE, Lagziel T, Pikkel YY, Duek OS, Ad-El DD, et al. Revitalizing hands: a comprehensive review of anatomy and treatment options for hand rejuvenation. Cureus. 2023;15(2):e35573.
8. Zhou J, Xie Y, Wang WJ, Herrler T, Hang RL, Zhao PJ, et al. Hand rejuvenation by targeted volume restoration of the dorsal fat compartments. Aesthet Surg J. 2017;38(1):92–100.
9. Bidic SM, Hatef DA, Rohrich RJ. Dorsal hand anatomy relevant to volumetric rejuvenation. Plast Reconstr Surg. 2010;126(1):163–8
10. Lefebvre-Vilardebo M, Trevidic P, Moradi A, Busso M, Sutton AB, Bucay VW. Hand: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(5):258S- 275S.
11. Conlon CJ, Abu-Ghname A, Davis MJ, Ali K, Winocour SJ, Eisemann ML, et al. Fat grafting for hand rejuvenation. Semin Plast Surg. 2020;34(1):47–52.
12. Zattar LC, Alves IS, Bernal ECBA, Zattar GA, Marcelino ASZ, Cerri LMO, et al. Radiologic approach for skin US. Radiographics. 2022;42(2):E73–4.
13. Zattar LC, Cerri GG. Ultrassonografia Dermatológica, 1 ed. São Paulo: Manole; 2021.
14. Wortsman X, Wortsman J. Sonographic outcomes of cosmetic procedures. 2011;197(5):W910–8.
15. Man J, Rao J, Goldman M. A double-blind, comparative study of nonanimal-stabilized hyaluronic acid versus human collagen for tissue augmentation of the dorsal hands. Dermatol Surg. 2008;34(8):1026–31.
16. Micheels P, Besse S, Sibon M, Elias B. Hand rejuvenation with A hyaluronic acid-based dermal filler: a 12-Month clinical follow-up case series. J Drugs Dermatol. 2021;20(4):451–9.
17. Sadick NS, Anderson D, Werschler WP. Addressing volume loss in hand rejuvenation: a report of clinical experience. J Cosmet Laser Ther. 2008;10(4): 237–41.
18. Khosravani N, Weber L, Patel R, Patel A. The 5-Step filler hand rejuvenation: filling with hyaluronic acid. Plast Reconstr Surg Glob Open. 2019;7(1):e2073.
19. Wortsman X, Wortsman J, Orlandi C, Cardenas G, Sazunic I, Jemec GBE. Ultrasound detection and identification of cosmetic fillers in the skin. J Eur Acad Dermatol Venereol. 2012;26(3):292–3.
20. Butterwick K, Lowe NJ. Injectable poly-L-lactic acid for cosmetic enhancement: learning from the european experience. J Am Acad Dermatol. 2009;61(2):281–93.
21. Redaelli A. Cosmetic use of polylactic acid for hand rejuvenation: report on 27 patients. J Cosmet Dermat. 2006;5(3)233–8.
22. Busso M, Applebaum D. Hand augmentation with Radiesse (Calcium hydroxylapatite. Dermatol Ther. 2007;20(6):385–7.
23. Gargasz SS, Carbone MC. Hand rejuvenation using Radiesse. Plast Reconstr Surg. 2010;125(6):259e–60e.
24. Sadick NS. A 52-week study of safety and efficacy of calcium hydroxylapatite for rejuvenation of the aging hand. J Drugs Dermatol. 2011;10(1):47–51.
25. Bank DE. A novel approach to treatment of the aging hand with Radiesse. J Drugs Dermatol. 2009;8(12):1122–6.
26. Fontan Câmara CB, Cardoso D, de Rezende JP, Zattar LC, Mota A. Ultrasound evaluation of fillers and biostimulators using different ultrasound devices and frequencies. Journal of Diagnostic Imaging. 2023;1(1):e2023004.
27. Wortsman X, Quezada N, Peñaloza O, Cavellieri F, Schelke L, Velthius P. Ultrasonographic patterns of calcium hydroxyapatite according to dilution and mix with hyaluronic acid. J Ultrasound Med. 2023;42(9):2065–72.
28. Urdiales-Gálvez F, Braz A, Cavallini M. Facial rejuvenation with the new hybrid filler HArmonyCa™: clinical and aesthetic outcomes assessed by 2D and 3D photographs, ultrasound, and elastography. J Cosmet Dermatol. 2023;22(8):2186–97.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}